Health-Related Quality of Life After Laparoscopic Nissen Fundoplication: A Long-Term Single-Center Cohort Analysis
Mauro Sousa, Maria João Samúdio, Luís Castro, Luís Miranda, Fernanda Quirino

TL;DR
This study shows that laparoscopic Nissen fundoplication improves quality of life for GERD patients long-term, with high satisfaction and low reoperation rates.
Contribution
The study provides long-term HRQoL data and satisfaction outcomes after laparoscopic Nissen fundoplication in a single-center cohort.
Findings
84.6% of patients reported satisfaction with the surgical outcome.
53.7% of patients discontinued proton pump inhibitor use after surgery.
GERD-HRQL scores improved significantly in most domains, including heartburn and regurgitation.
Abstract
Introduction and objectives: Gastro-oesophageal reflux disease (GERD) significantly impairs quality of life, particularly in patients with persistent symptoms despite optimal medical therapy. Laparoscopic Nissen fundoplication (LNF) is considered the gold-standard surgical treatment for well-characterised, refractory GERD. This study aimed to retrospectively evaluate long-term health-related quality of life (HRQoL), patient satisfaction, and proton pump inhibitor (PPI) use following LNF in a single-centre cohort. Methods: All consecutive patients undergoing LNF at our institution between January 2009 and December 2019 were retrospectively reviewed. Demographic data, medication use, reoperations, and satisfaction were collected. Symptom burden was assessed using an adapted version of the validated GERD-HRQL questionnaire, administered by a structured telephone interview. Pre- and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
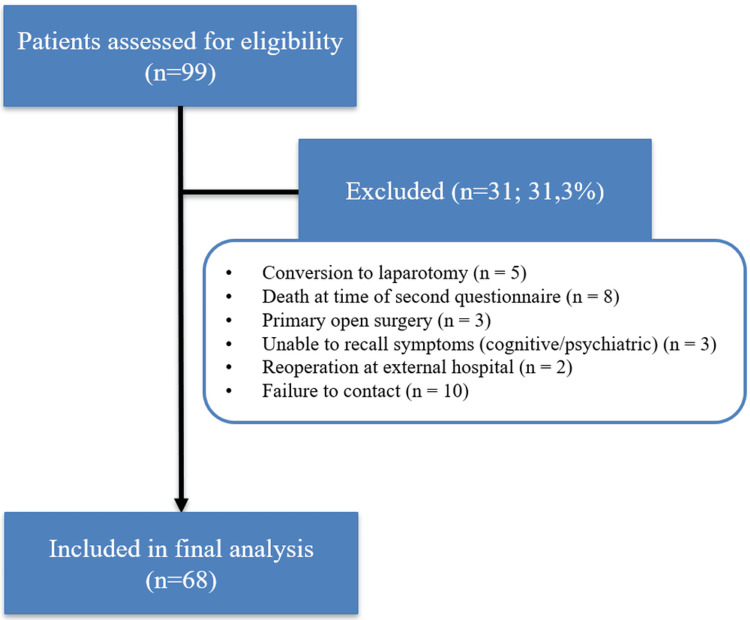 Figure 1
Figure 1| Variables | Results |
| Age, years (IQR) | 66 (57-75) |
| Gender, female, n (%) | 54 (79.4) |
| Postoperative follow-up duration, years (IQR) | 5.5 (3.0-8.0) |
| Reoperation rate, n (%) | 2 (2.9) |
| Perioperative mortality, n (%) | 0 |
| PPI use prior to surgery, n (%) | 61 (91.0) |
| PPI discontinuation after the procedure, n (%) | 36 (53.7) |
| Satisfaction Level | Frequency | Confidence intervals |
| Satisfied, n (%) | 55 (84.6%) | 95% CI: 73.9–91.4% |
| Neutral, n (%) | 4 (6.2%) | 95% CI: 2.4–14.8% |
| Dissatisfied, n (%) | 6 (9.2%) | 95% CI: 4.3–18.7% |
| Symptom | Pre-surgery | Post surgery | Test value | p-value |
| Heartburn | 3.5 (2.0–5.0) | 0 (0–1.0) | Z=–6.545 | <0.001 |
| Heartburn when lying down | 4.0 (2.0–5.0) | 0 (0–1.0) | Z=–6.472 | <0.001 |
| Heartburn when standing | 3.0 (1.0–4.0) | 0 (0–0) | Z=–6.117 | <0.001 |
| Heartburn after meals | 4.0 (2.0–5.0) | 0 (0–1.0) | Z=–6.325 | <0.001 |
| Heartburn alters diet | 3.0 (1.0–4.0) | 0 (0–1.0) | Z=–5.339 | <0.001 |
| Heartburn disrupts sleep | 2.0 (0.0–4.0) | 0 (0–0) | Z=–5.190 | <0.001 |
| Difficulty swallowing | 0 (0.0–1.0) | 0 (0–1.0) | Z=–1.730 | 0.084 |
| Pain with swallowing | 0 (0.0–1.0) | 0 (0–0) | Z=–2.831 | 0.005 |
| Medication affects daily life | 0 (0.0–1.0) | 0 (0–0.0) | Z=–2.911 | 0.004 |
| Regurgitation | 2.5 (1.0–4.0) | 0 (0–1.0) | Z=–5.892 | <0.001 |
| Regurgitation when lying down | 2.0 (1.0–4.0) | 0 (0–1.0) | Z=–5.682 | <0.001 |
| Regurgitation when standing | 1.0 (0.0–2.0) | 0 (0–0) | Z=–4.853 | <0.001 |
| Regurgitation after meals | 2.0 (1.0–4.0) | 0 (0–1.0) | Z=–5.761 | <0.001 |
| Regurgitation alters diet | 3.0 (0.0–4.0) | 0 (0–1.0) | Z=–5.085 | <0.001 |
| Regurgitation disrupts sleep | 0 (0.0–1.0) | 0 (0–0) | Z=–3.331 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Esophageal and GI Pathology · Eosinophilic Esophagitis
Introduction
Gastro-oesophageal reflux disease (GERD) is one of the most common upper gastrointestinal disorders, with a substantial impact on healthcare systems and patient quality of life [1]. Although the majority of patients respond to lifestyle modification and proton pump inhibitors (PPIs), a proportion continue to experience troublesome symptoms, develop intolerance to long-term therapy, or prefer a definitive treatment option [2].
Surgical intervention is well established in this context. Laparoscopic Nissen fundoplication (LNF), first introduced in 1956 and subsequently adapted to minimally invasive techniques, has become the most widely performed anti-reflux operation. According to international consensus and guideline statements, LNF is considered the gold-standard surgical treatment for GERD [3].
Beyond durability of symptom control, reoperation rates, and medication discontinuation, health-related quality of life (HRQoL) is a particularly relevant outcome in GERD. The disease affects not only physical symptoms such as heartburn and regurgitation but also daily functioning, sleep, diet, and social well-being. Patient-reported outcomes are therefore essential to evaluate the long-term benefits of surgery beyond objective physiological measurements [4].
The objective of this study was to retrospectively assess the long-term impact of LNF on HRQoL, patient satisfaction, and PPI use, using an adapted GERD-HRQL questionnaire [5,6] in a single-centre cohort.
Materials and methods
Study design and setting
This was a retrospective cohort study including all consecutive patients who underwent LNF, with or without concomitant hiatal hernia repair, at the Hospital de Santa Maria, Lisbon, Portugal, between January 2009 and December 2019. All procedures were performed by a dedicated surgical team.
Eligibility criteria
Patients were eligible if they had GERD supported by typical symptoms plus objective confirmation on preoperative work-up (endoscopy and/or pathological acid exposure on 24-hour pH monitoring). In line with current practice, pH monitoring was omitted in cases of severe erosive oesophagitis on endoscopy (Los Angeles grade C/D). Exclusion criteria were predefined and are summarised in the flow diagram (Figure 1).
A flow diagram of patient inclusion and exclusionA total of 99 patients were assessed for eligibility; 31 were excluded for predefined reasons, leaving 68 patients for the final analysis.
Participant flow
Of 99 patients initially identified, 68 were included in the final analysis. Thirty-one patients were excluded for the following reasons: conversion to laparotomy (n = 5), death from unrelated causes at the time of the second follow-up questionnaire (n = 8), primary open surgery (n = 3), inability to recall preoperative symptoms due to cognitive or psychiatric conditions (n = 3), reoperation at an external hospital (n = 2), and failure to contact despite multiple attempts (n = 10) (Figure 1).
Surgical technique
All procedures were performed laparoscopically following a standardised approach. The short gastric vessels were routinely divided to ensure a tension-free wrap. The distal oesophagus was mobilised for at least 3 cm into the abdominal cavity, and the hernia sac was dissected when present. A 360° floppy fundoplication was constructed without the use of a calibration bougie. Hiatal closure was systematically performed with three interrupted silk sutures. The majority of patients either had no hiatal hernia or a small type I (sliding) hernia, and in these cases, the hiatal defect was consistently closed with sutures only, without mesh reinforcement.
Outcomes and data collection
The primary outcome was change in disease-specific HRQoL, measured with an adapted GERD Health-Related Quality of Life (GERD-HRQL) questionnaire (Appendix A). This version comprises the original validated 10-item instrument [5,6] (items scored 0 to 5; lower scores indicate better symptom control) [6]. Secondary outcomes included patient satisfaction (0-10 global scale) and PPI use. Follow-up was conducted through structured, interviewer-administered telephone questionnaires. Preoperative GERD-HRQL scores were collected retrospectively by patient recall during these interviews, which is acknowledged as a potential source of recall bias.
Statistical analysis
Data were analysed using IBM SPSS Statistics (version 30.0, IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality using the Shapiro-Wilk test. As most variables were non-normally distributed, results are presented as median (interquartile range, IQR). Comparisons between pre- and postoperative GERD-HRQL scores were performed with the Wilcoxon signed-rank test, with test statistics (Z) and two-tailed p-values reported. Statistical significance was set at p < 0.05.
Analysis of population and missing data
Paired pre- and postoperative comparisons were restricted to patients with both GERD-HRQL assessments (n = 68). A complete-case approach was used, and denominators are specified where responses were missing (e.g., patient satisfaction n = 65/68). No adjustment for multiple comparisons was performed, and p-values are interpreted as exploratory.
Results
A total of 68 patients were included in the final analysis (Table 1). All patients completed both pre- and postoperative GERD-HRQL questionnaires, and patient satisfaction responses were available for 65 of 68 patients (95.6%). Of these, 79.4% (n = 54) were female. The median age was 66 years (range: 27-86 years), and the median postoperative follow-up duration was 5.5 years (IQR: 3.0-8.0 years). The reoperation rate was 2.9% (n = 2), and there were no procedure-related deaths.
Prior to surgery, 91% (n = 61) of patients were on PPIs. Following LNF, 53.7% (n = 36) were able to discontinue PPI therapy. Among those who continued PPIs (46.3%, n = 31), most were taking concurrent medications such as non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, or other agents requiring gastric protection due to increased risk of peptic ulcer disease.
Patient satisfaction (Table 2) was high: 84.6% of respondents reported being satisfied with their surgical outcome (95% CI: 73.9-91.4%), 6.2% were neutral (95% CI: 2.4-14.8%), and 9.2% expressed dissatisfaction (95% CI: 4.3-18.7%). Patient satisfaction responses were available for 65 of 68 patients (95.6%). The median satisfaction score was 8 (on a scale from 0 to 10).
Postoperative symptom improvement (Table 3) was significant across nearly all assessed domains. The GERD-HRQL domains are scored from 0 to 5, with lower values indicating better symptom control. Median scores decreased substantially in relation to heartburn (overall, positional, and postprandial), regurgitation, and symptoms interfering with sleep or diet (p < 0.001 for all). For dysphagia, scores showed a non-significant trend towards improvement (p = 0.084).
Discussion
This study shows that LNF provides significant and durable improvement in disease-specific HRQoL, with high long-term patient satisfaction and low reoperation rates. Nevertheless, nearly half of the patients continued to use PPIs, and dysphagia showed only a non-significant trend towards improvement.
Our results are consistent with previous long-term series of LNF, which also report durable symptom control, high satisfaction rates, and low reoperation rates [7-9]. Compared with these studies, our cohort is of moderate size but has a median follow-up of 5.5 years, which strengthens the reliability of the findings. Similar to prior reports, persistent PPI use remains common, reflecting not only ongoing reflux-related symptoms but also prescriptions for other indications such as gastric protection in patients requiring antiplatelet or anti-inflammatory therapy [10].
The non-significant trend towards improvement in dysphagia highlights the complexity of this symptom, which may persist even after technically successful surgery. Transparent reporting of this result avoids overstatement and aligns with recommendations on the importance of patient-reported outcomes in antireflux surgery [11].
This study has certain limitations. First, its retrospective design introduces the risk of recall bias, since preoperative HRQoL scores were collected retrospectively during follow-up interviews. As such, our findings demonstrate associations rather than causal relationships, and potential confounders (such as lifestyle modifications or the natural course of disease) cannot be excluded. Second, approximately 10% of the initial cohort could not be contacted, representing a potential non-responder bias. Third, as this was a single-centre study conducted at a tertiary referral hospital, the findings may not be generalisable to other settings with different patient populations or surgical expertise. Fourth, while the median follow-up was 5.5 years, the variability (range three to eight years) may mask late symptom recurrence. Finally, the absence of a control group prevents direct comparison with alternative surgical procedures or medical therapy. Persistent use of PPIs in nearly half of the cohort also represents a clinically relevant limitation that should be addressed in preoperative counselling.
Furthermore, we used an adapted version of the GERD-HRQL, in which the original “gassy/bloating feelings” item was omitted and replaced by a six-item regurgitation block. While this adaptation reflects clinical practice and provides useful information, it has not been formally validated, which may limit direct comparability with studies using the original 10-item instrument.
Despite these limitations, our findings provide valuable long-term patient-reported outcome data, reinforcing the role of LNF as a safe and effective surgical option for appropriately selected patients with GERD.
Conclusions
LNF is a safe, effective, and durable surgical treatment for patients with well-characterised, refractory GERD. In this single-centre cohort, the procedure was associated with sustained improvement in symptom control, enhanced HRQoL, and high long-term patient satisfaction. More than half of the patients discontinued proton pump inhibitors after surgery, and the need for reoperation was very low.
These findings highlight the value of LNF not only in reducing symptom burden but also in restoring overall patient well-being in selected individuals. Persistent PPI use and the non-significant trend regarding dysphagia underscore the importance of preoperative counselling, realistic expectations, and tailored postoperative follow-up. Future prospective, multicentre studies are needed to validate these results and further refine patient selection criteria and perioperative management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review Gut El-Serag HB Sweet S Winchester CC Dent J 8718806320142385321310.1136/gutjnl-2012-304269 PMC 4046948 · doi ↗ · pubmed ↗
- 2Effectiveness of laparoscopic fundoplication in relieving the symptoms of gastroesophageal reflux disease (GERD) and eliminating antireflux medical therapy Surg Endosc Papasavas PK Keenan RJ Yeaney WW Caushaj PF GagnéDJ Landreneau RJ 120012051720031273911710.1007/s 00464-002-8910-y · doi ↗ · pubmed ↗
- 3Multi-society consensus conference and guideline on the treatment of gastroesophageal reflux disease (GERD)Surg Endosc Slater BJ Collings A Dirks R 7818063720233652985110.1007/s 00464-022-09817-3 · doi ↗ · pubmed ↗
- 4Laparoscopic Nissen fundoplication controls reflux symptoms and improves disease-specific quality of life in patients with class I and II obesity Surgery Martin Del Campo SE Chaudhry UI Kanji A Suzo AJ Perry KA 1048105416220172882700110.1016/j.surg.2017.07.006 · doi ↗ · pubmed ↗
- 5Quality of life scale for gastroesophageal reflux disease J Am Coll Surg Velanovich V Vallance SR Gusz JR Tapia FV Harkabus MA 2172241831996 https://pubmed.ncbi.nlm.nih.gov/8784314/8784314 · pubmed ↗
- 6The development of the GERD-HRQL symptom severity instrument Dis Esophagus Velanovich V 1301342020071743959610.1111/j.1442-2050.2007.00658.x · doi ↗ · pubmed ↗
- 7Assessment of quality of life after laparoscopic Nissen fundoplication in patients with gastroesophageal reflux disease World J Surg Balci D Turkcapar AG 1161213120071717149710.1007/s 00268-005-0658-9 · doi ↗ · pubmed ↗
- 8Health-related quality of life 10 years after laparoscopic nissen fundoplication-results of a community-based hospital J Laparoendosc Adv Surg Tech A Neuvonen P Iivonen M Sintonen H Rantanen T 1341382420142452824810.1089/lap.2013.0479 · doi ↗ · pubmed ↗