Panhypopituitarism Presenting as Myxedema Coma Unveiling Sheehan's Syndrome
Mennaallah Eid, Daniel Joseph Toft

TL;DR
A woman with a history of postpartum hemorrhage was later diagnosed with Sheehan's syndrome, a rare pituitary disorder, after presenting with myxedema coma and panhypopituitarism.
Contribution
This case emphasizes the importance of checking free thyroxine levels in diagnosing central hypothyroidism despite normal thyroid stimulating hormone levels.
Findings
The patient had panhypopituitarism and myxedema coma with a history of postpartum hemorrhage.
Delayed diagnosis occurred due to normal thyroid stimulating hormone levels without free thyroxine testing.
The case is consistent with Sheehan's syndrome following postpartum hemorrhage 18 years prior.
Abstract
Myxedema coma (MC) is a rare and life-threatening complication of uncontrolled hypothyroidism. We report a 46-year-old Hispanic female who presented with hemodynamic instability and hyponatremia. She was initially diagnosed with adrenal insufficiency (AI). Further evaluation revealed myxedema features and panhypopituitarism, with partial empty Sella. A thorough history was notable for postpartum hemorrhage 18 years prior and followed by failure of lactation and secondary amenorrhea which is consistent with Sheehan's syndrome. Our case highlights the delayed diagnosis of central hypothyroidism with normal thyroid stimulating hormone levels without checking free thyroxine level and emphasizing the importance of comprehensive evaluation in similar presentations.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
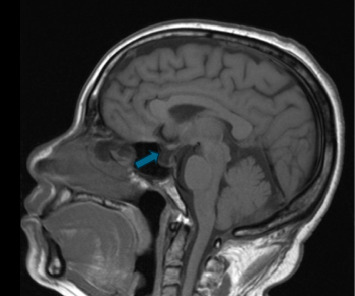 Figure 1
Figure 1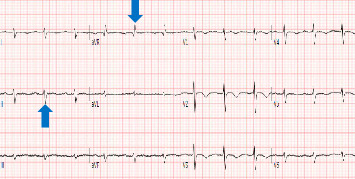 Figure 2
Figure 2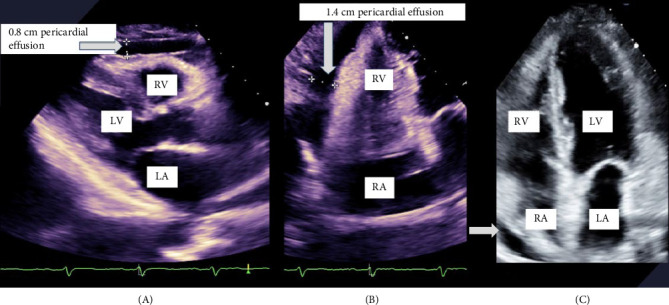 Figure 3
Figure 3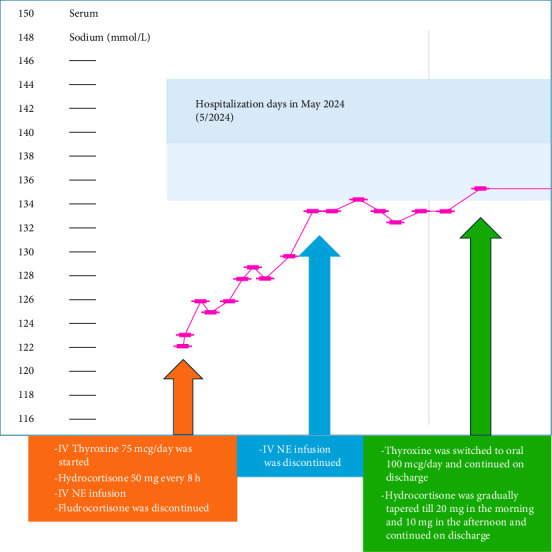 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Pituitary Gland Disorders and Treatments · Thyroid Disorders and Treatments
1. Introduction
Myxedema coma (MC) is a rare complication of extreme decompensated hypothyroidism. It occurs more frequently in primary hypothyroidism than in central hypothyroidism [1], with an estimated mortality rate of 20%–60% [2]. Triggers include infection, surgery, trauma, and prolonged untreated hypothyroidism. Despite its name, coma is an uncommon presentation; instead, most patients present with altered mental status [3]. The diagnosis and management of MC remain a challenging endocrine emergency, requiring a high clinical suspicion [1].
2. Case Presentation
A 46-year-old Hispanic female presented to another facility with fatigue and low energy for weeks. She was found to have hemodynamic instability, severe hyponatremia, low random cortisol, and pericardial effusion. Thyroid-stimulating hormone (TSH) was normal. Initial diagnosis was adrenal insufficiency (AI), and she was managed with intravenous (IV) norepinephrine (NE) infusion, IV hydrocortisone (HC) 50 mg every 8 h, and oral fludrocortisone 0.1 mg/day before being transferred to our intensive care unit (ICU).
On examination, body weight was 62 kg, and height was 152 cm. While receiving IV pressors and stress steroid, vital signs were: blood pressure 91/54 millimeters of mercury (mmHg), heart rate 83 beats per minute (bpm), respiratory rate 12 breaths per minute, temperature 99°F, and oxygen saturation 97% on room air. She was obtunded and sleepy, responding slowly to verbal stimuli and disoriented to time. Loss of the outer third of the eyebrows, periorbital edema, slurred and slow speech, dry thickened skin, and decreased deep tendon reflexes' responses were noted. The thyroid exam was unremarkable. Heart sounds were normal, and the lungs were clear to auscultation.
She reported chronic constipation and reduced functional capacity. She has four children, with last pregnancy 18 years ago, and complicated by postpartum hemorrhage that requires blood transfusion. On further questioning, she recalled being unable to lactate, with absence of menstrual cycles thereafter. She has not had medical evaluation before this presentation. Laboratory evaluation while on IV pressors and stress steroids revealed hypo-osmolar hyponatremia with low urine osmolality and sodium, as well as hyperlipidemia (Tables 1?–3). Pituitary hormone testing confirmed central hypothyroidism with undetectable free thyroxine (FT4) and normal TSH, low follicle-stimulating hormone (FSH) and luteinizing hormone (LH), estradiol, insulin-like growth factor-1 (IGF-1), and prolactin (PRL) (Table 4). Brain magnetic resonance imaging (MRI) performed for altered mental status evaluation showed a partial empty sella (Figure 1). Further testing revealed low-voltage complexes and prolonged QTc on electrocardiogram (ECG) (Figure 2), a small pericardial effusion, and normal ventricular function on transthoracic echocardiogram (TTE) (Figure 3).
IV thyroxine dose of 200 microgram (mcg) was started, followed by 75 mcg/day Empirical IV antibiotics were initiated until sepsis was excluded. Workup for anemia showed a normal iron profile, vitamin B12, and folate levels.
The patient improved significantly with IV thyroxine. She resumed bowel movements, became more interactive, and exhibited improved speech. Serum sodium normalized from 122 to 136 millimole per liter (mmol/L), and IV NE was discontinued after 2 days. Stress-dose steroids were gradually tapered to oral HC 20 mg in the morning and 10 mg in the afternoon. After 3 days, she was transitioned to oral thyroxine at 100 mcg/day (Figure 4). She was discharged on oral thyroxine and HC with endocrinology follow-up for further hormonal evaluation and long-term management.
3. Discussion
MC is a rare and lethal complication of Sheehan's syndrome [1]. Central hypothyroidism is less common than primary hypothyroidism, with an estimated prevalence of 1 in 20,000 to 1 in 80,000 [4]. A normal TSH level alone is insufficient to exclude thyroid disorders, as failure to assess FT4 can delay or miss the diagnosis of central hypothyroidism. Our case has panhypopituitarism secondary to Sheehan's syndrome with an 18-year delay in diagnosis and management. Clinical features of myxedema were noted with normal TSH which raises the possibility of central hypothyroidism. Subsequent hormonal evaluation confirmed the diagnosis with an undetectable free T4 and inappropriately normal TSH. Further workup revealed panhypopituitarism including central hypogonadism (low FSH, LH, and undetectable estradiol associated with secondary amenorrhea), low IGF-1, and low PRL levels.
We concluded that MC was due to prolonged untreated central hypothyroidism after exclusion of septic and circulatory causes. Our case exhibited other features of hypothyroidism, including a small pericardial effusion, low QTc voltage, normocytic normochromic anemia, and hyperlipidemia, which may also be attributed to deficiencies in other pituitary hormones. Neutrophilia, lymphopenia, and eosinopenia could be due to steroid therapy. Although hypoglycemia and bradycardia may have been masked by IV pressors and stress steroid, the hypotension, hypothermia, and hyponatremia only improved following IV thyroxine administration. The duration of panhypopituitarism prior to presentation is unclear; however, the history of postpartum hemorrhage, failure of lactation, and secondary amenorrhea strongly suggests long-standing hypopituitarism due to pituitary apoplexy.
The causes of central hypothyroidism include structural lesions, trauma, surgery, hemorrhage, ischemia, irradiation, inflammation, infiltration, or genetic disorders of the pituitary gland and/or hypothalamus [2]. More recently, immune checkpoint inhibitors, particularly cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitors, have been recognized as an emerging cause of hypophysitis [5]. Sheehan's syndrome results from postpartum hemorrhage leading to pituitary infraction. While its incidence has declined due to advances in obstetric care, cases with a remote history of postpartum hemorrhage may still be diagnosed years later through a detailed history, often after presenting with central hormone deficiencies [1], as seen in our case. Hyponatremia is frequently associated with hypothyroidism, particularly MC and AI. It is often attributed to a syndrome of inappropriate antidiuretic hormone secretion (SIADH)-like state, thought to result from impaired renal perfusion and reduced free water excretion, which improves with hormonal replacement therapy [6].Our patient presented with hypo-osmolar hyponatremia, but low urine osmolality and specific gravity were inconsistent with SIADH. Additionally, low urine sodium could be due to dehydration. It is noteworthy that urinary evaluation was performed, while the patient was receiving IV pressors and stress steroid. Serum sodium improved to 136 mmol/L with IV isotonic saline and IV thyroxine.
Diagnosing MC is challenging and requires a high index of clinical suspicion. A scoring system has been proposed, where a score >60 strongly suggests MC [7]. Retrospectively, our patient had a score of 65. Early recognition and treatment of MC are critical to improve the survival rates. The American Thyroid Association (ATA) recommends administering stress-dose steroids before initiating IV thyroxine therapy, with a loading dose of 200–400 mcg IV thyroxine, followed by a weight-based maintenance dose of 1.6 mcg/kg/day orally or 75% of the calculated dose if given IV [8]. Routine triiodothyronine (T3) therapy is not recommended due to its higher potency and risk of cardiac ischemia. However, T3 can be added to levothyroxine in cases of persistent hypothyroid symptoms or in patients with malabsorption syndromes affecting levothyroxine uptake [9].
The goal of CH treatment is to maintain FT4 levels in the upper half of the normal reference range. A persistently unsuppressed TSH may indicate undertreatment [2]. When initiating hormone replacement therapy, interactions between thyroxine and other hormones should be considered. Estrogen therapy increases thyroid-binding globulin (TBG), requiring a higher thyroxine dose. Testosterone replacement reduces TBG, potentially lowering thyroxine requirements and higher doses of thyroxine are needed with growth hormone replacement [2].
4. Conclusion
Central hypothyroidism can be overlooked when relying solely on TSH screening without measuring FT4. Sheehan's syndrome is now rare; however, it should be considered during history taking for central endocrine disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ono Y. Ono S. Yasunaga H. Matsui H. Fushimi K. Tanaka Y. Clinical Characteristics and Outcomes of Myxedema Coma: Analysis of a National Inpatient Database in Japan Journal of Epidemiology 201727311712210.1016/j.je.2016.04.0022-s 2.0-8501704777328142035 PMC 5350620 · doi ↗ · pubmed ↗
- 2Persani L. Central Hypothyroidism: Pathogenic, Diagnostic, and Therapeutic Challenges The Journal of Clinical Endocrinology & Metabolism 20129793068307810.1210/jc.2012-16162-s 2.0-8486614994722851492 · doi ↗ · pubmed ↗
- 3Kwaku M. P. Burman K. D. Myxedema Coma Journal of Intensive Care Medicine 200722422423110.1177/08850666073013612-s 2.0-3444765111017712058 · doi ↗ · pubmed ↗
- 4Price A. Weetman A. P. Screening for Central Hypothyroidism is Unjustified BMJ: British Medical Journal 2001322728910.1136/bmj.322.7289.798798 PMC 111997011303532 · doi ↗ · pubmed ↗
- 5Kwon H. Roh E. Ahn C. H. Immune Checkpoint Inhibitors and Endocrine Disorders: A Position Statement From the Korean Endocrine Society Endocrinology and Metabolism 202237683985010.3803/En M.2022.162736604955 PMC 9816514 · doi ↗ · pubmed ↗
- 6Pantalone K. M. Hatipoglu B. A. Hyponatremia and the Thyroid: Causality or Association? Journal of Clinical Medicine 2015413236 PMID: 26237016; PMCID: PMC 447023710.3390/jcm 4010032 PMC 447023726237016 · doi ↗ · pubmed ↗
- 7Popoveniuc G. Chandra T. Sud A. A Diagnostic Scoring System for Myxedema Coma Endocrine Practice 201420880881710.4158/EP 13460.OR 2-s 2.0-8490655461324518183 · doi ↗ · pubmed ↗
- 8Jonklaas J. Bianco A. C. Bauer A. J. Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement Thyroid 2014241216701751 PMID: 25266247; PMCID: PMC 426740910.1089/thy.2014.00282-s 2.0-8491858326025266247 PMC 4267409 · doi ↗ · pubmed ↗