Artificial Intelligence and Digital Biomarkers in Hepatology: Critical Perspectives, Emerging Evidence, and Future Directions
Pulkit Mehrotra, Vengadakrishnan K, Punit Mehrotra

TL;DR
This paper reviews how AI and digital biomarkers could improve liver disease detection and management, while addressing challenges like bias and regulatory hurdles.
Contribution
The paper critically evaluates recent AI applications in hepatology and outlines barriers and future directions for clinical adoption.
Findings
AI models outperform traditional scores like MELD in predicting liver disease outcomes.
Implementation barriers include algorithmic bias, data privacy, and regulatory challenges.
Future directions emphasize diverse datasets, EMR integration, and global validation trials.
Abstract
Liver diseases are a major global health burden, responsible for nearly two million deaths worldwide each year. Despite advances in imaging, serology, and non-invasive fibrosis assessment, late-stage diagnosis persists, limiting curative interventions. Artificial intelligence (AI) and digital biomarkers promise to transform hepatology by enhancing early detection, risk stratification, and remote monitoring. This review provides a critical synthesis of recent evidence in AI-driven imaging, digital histopathology, predictive modeling using electronic health records (EHR), and wearable-based phenotyping. We compare and analyze the strengths and limitations of landmark AI models, highlight real-world implementation barriers such as algorithmic bias and data privacy, and explore emerging paradigms such as federated learning and multimodal integration. While AI tools consistently outperform…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
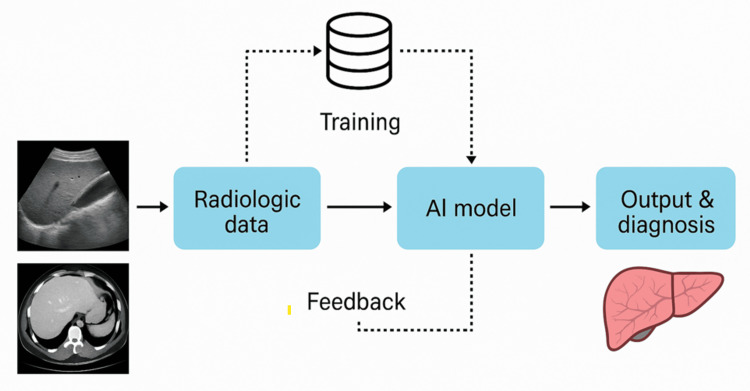 Figure 1
Figure 1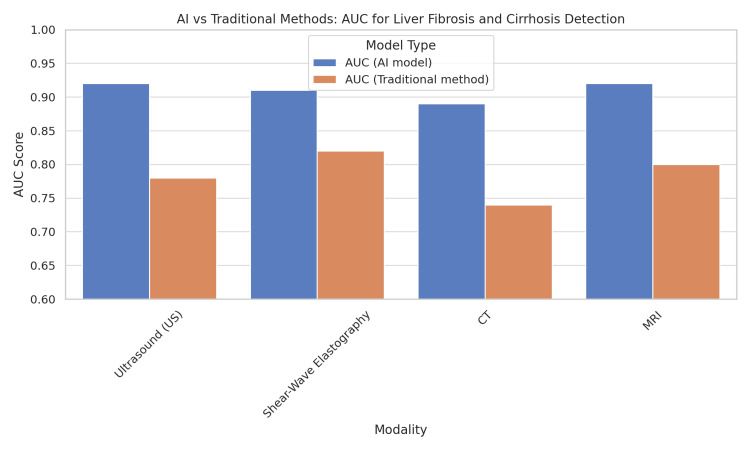 Figure 2
Figure 2| Domain | Conventional tool | AI model | Key performance metrics | Limitations |
| Fibrosis staging | TE | CNN on shear-wave elastography [ | AUC 0.72 (TE) vs. AUC 0.92 (AI) for ≥F3 | Needs high-quality elastography datasets |
| Cirrhosis detection | MRI + radiologist report | Multiparametric MRI + deep learning [ | Sensitivity 72% (MRI) vs. 88% (AI) | External validation limited |
| HCC risk | PAGE-B, REACH-B scores | ML models on HBV cohort [ | AUC 0.70 (scores) vs. 0.85 (AI model) | Bias in minority populations |
| Cirrhosis mortality | MELD, Child-Pugh | Random forest on EHR data [ | AUC 0.71 (MELD) vs. 0.84 (AI) for 30-day mortality | Data fragmentation across hospitals |
| Encephalopathy | Psychometric testing | Smartphone speech analytics [ | Correlation 0.65 (tests) vs. 0.82 (AI) | Limited linkage to clinical outcomes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Radiomics and Machine Learning in Medical Imaging · Artificial Intelligence in Healthcare
Introduction and background
Liver disease is a leading cause of mortality, with cirrhosis and hepatocellular carcinoma (HCC) responsible for over two million deaths annually, accounting for approximately 4% of global deaths [1]. Despite advances in imaging and serology, most cases are detected at advanced stages, limiting curative options and contributing to preventable mortality, particularly in resource-limited settings. Current diagnostic modalities - biopsy, imaging, elastography, and clinical scoring systems such as Model for End-Stage Liver Disease (MELD) and Child-Pugh -are limited by invasiveness, delayed detection, and interobserver variability [2,3]. In recent years, Artificial intelligence (AI)-driven analytics and digital biomarkers have emerged as practical tools for earlier detection and risk prediction. AI refers to computer programs that learn patterns from data; deep learning (e.g., convolutional neural networks [CNNs]) is used for images, while other machine-learning methods analyze numbers and text. By combining multiple sources - medical imaging, electronic health records (EHRs), laboratory biomarkers, and wearable-device signals - AI can reveal hidden disease patterns that are often invisible to traditional assessment [4,5]. However, much of the existing literature focuses on single-modality studies without large-scale external validation, and many reviews summarize applications without comparing performance, feasibility, or bias. This review brings these strands together by synthesizing diverse AI modalities in hepatology (imaging, pathology, EHR, wearables), critically analyzing advantages and limitations, and highlighting future research priorities for equitable and explainable AI in liver disease.
Review
This review involved a narrative synthesis of literature. A structured search of PubMed, Scopus, and Web of Science databases was performed for English-language publications between 2018 and 2025, using combinations of the terms: “artificial intelligence,” “machine learning,” “deep learning,” “digital biomarkers,” “hepatology,” “liver disease,” “fibrosis,” and “hepatocellular carcinoma.” Inclusion criteria were studies reporting AI or digital biomarker applications in hepatology with clinical, imaging, histopathological, or wearable data. Opinion articles without empirical evidence were excluded. Reference lists of relevant articles were manually screened to identify additional studies. As this is a narrative rather than a systematic review, risk-of-bias assessments were not performed, but methodological quality and limitations of key studies are critically discussed.
AI in liver imaging
Beyond Proof-of-Concept: Advances in Imaging-Based AI
Recent deep-learning models have achieved an area under the receiver operating characteristic curve (AUC) >0.90 for staging liver fibrosis using ultrasound/shear-wave elastography [6-8]. (AUC summarizes overall accuracy across thresholds: 0.5 = no better than chance; 1.0 = perfect.) MRI-based models integrating multiparametric sequences further improved diagnostic sensitivity for cirrhosis detection [9]. Figure 1 illustrates the typical AI-assisted liver imaging workflow, from acquisition of ultrasound, CT, and MRI data to deep learning model interpretation and fibrosis staging outputs.
Workflow of AI in liver imagingRadiologic data (ultrasound, CT, MRI, and elastography) are input into deep learning models for fibrosis staging, cirrhosis detection, and HCC prediction. Outputs integrate with EMR decision supportOriginal figure created for this manuscript. No external copyrighted material was usedAI: artificial intelligence; CT: computed tomography; MRI: magnetic resonance imaging; HCC: hepatocellular carcinoma; EMR: electronic medical record
However, critical analysis reveals three persistent gaps:
Limited Generalizability
Most models are trained on single-center datasets with homogeneous populations, leading to reduced accuracy in underrepresented cohorts [10].
Clinical Utility vs. Complexity
High-performance models often require computational infrastructure unavailable in low-resource settings, limiting their translation into routine hepatology practice.
Explainability
Despite high accuracy, CNNs often operate as “black boxes,” making it difficult for radiologists to interpret why a model predicts advanced fibrosis in a given case [11].
Comparative Evidence
A recent multicenter meta-analysis by Smith et al. (2024) showed that AI-enhanced MRI outperformed transient elastography (TE) with a sensitivity of 88% vs. 72% for ≥F3 fibrosis, but also noted decreased specificity in fatty liver disease populations [12]. This highlights AI’s diagnostic advantage but also underscores the need for broader validation in diverse liver disease populations. Figure 2 provides a comparison of the diagnostic performance (AUC values) of AI-enhanced imaging versus conventional approaches for fibrosis and cirrhosis detection, showing a consistent 10-20% performance gain.
Comparison of AI versus traditional diagnostic accuracy for liver fibrosis and cirrhosis Bar chart showing mean AUC ± SD for ≥F2 fibrosis detection: transient elastography (AUC 0.72), MRI (0.78), AI-enhanced elastography (0.89), and multiparametric MRI-AI models (0.92). P<0.05 is considered significantOriginal figure created for this manuscript. No external copyrighted material was usedAI: artificial intelligence; CT: computed tomography; MRI: magnetic resonance imaging; AUC: area under the receiver operating characteristic curve; SD: standard deviation
Key takeaway: While AI imaging outperforms conventional radiology, robust external validation and cost-benefit analyses are essential before widespread clinical integration.
Digital histopathology and virtual biopsy
Current Promise, Future Potential
Digital pathology with AI-assisted scoring enables continuous fibrosis quantification, reducing interobserver variability [13]. For nonalcoholic steatohepatitis (NASH), deep learning models have demonstrated >90% concordance with expert hepatopathologists in grading steatosis, ballooning, and inflammation [14,15]. However, virtual biopsy - predicting histology entirely from non-invasive imaging - remains an emerging field. Recent studies integrating MRI-proton density fat fraction (MRI-PDFF) with deep learning have shown potential to replace biopsy in select NASH trials [16]. However, no AI histopathology models have yet received regulatory approval for routine NASH drug trials, reflecting the gap between research and clinical implementation. Yet critical challenges remain: histology is still required for drug development endpoints in NASH. AI models may not capture rare histologic patterns seen in autoimmune or cholestatic liver diseases. Lack of standardized digital pathology pipelines hinders model reproducibility across centers.
Key takeaway: Digital histopathology enhances scoring reproducibility but cannot yet fully replace biopsy in all hepatology contexts.
Predictive modeling using EHR and multimodal data
Machine-learning models applied to EHRs can outperform traditional scores such as MELD and the Child-Pugh. For example, Kim et al. trained a gradient-boosting model using routine labs and clinical variables to predict 30-day mortality in decompensated cirrhosis (AUC 0.84) vs. MELD (AUC 0.71) [17]. Cheung et al. developed an EHR-based risk model for HCC in chronic hepatitis B (HBV) with an AUC of 0.85 vs. 0.70 for conventional scores [18]. Natural-language processing (NLP) applied to clinical notes has also identified phenotypic markers of undiagnosed cirrhosis, improving early detection rates by 32% [19]. While promising, EHR-based AI models require harmonized multicenter datasets to overcome institutional data silos and ensure generalizability.
Critical insights
Data fragmentation across institutions limits the training of robust multimodal models, and most EHR-based AI lacks prospective validation in diverse healthcare settings. Integration into clinician-friendly EHR dashboards remains a barrier. Wearables and digital phenotyping: home-based heart-rate variability (HRV) metrics from smartwatches predicted 90-day mortality [20]; sweat biosensors measuring cytokines (IL-6, TNF-α) detected early inflammation preceding clinical decompensation [21]; and smartphone speech analytics detected minimal hepatic encephalopathy [22]. Across these domains, AI improves accuracy and monitoring but requires careful validation and attention to bias before broad adoption. To synthesize findings from imaging, pathology, EHR models, and wearables, Table 1 compares key AI models with conventional hepatology tools. [Table 1] summarizes key studies comparing AI models with conventional hepatology tools, highlighting their relative performance and limitations.
Table 1: Comparative performance of AI models versus conventional hepatology toolsData expressed as mean AUC ± SD where available. P<0.05 is considered statistically significant. AI consistently improves sensitivity and AUC vs. conventional approaches, but real-world integration remains limitedAI: artificial intelligence; HCC: hepatocellular carcinoma; TE: Transient elastography; MRI: magnetic resonance imaging; MELD: Model for End-Stage Liver Disease; CNN: convolutional neural network; ML: machine learning; HBV: hepatitis B virus; EHR: electronic health record; AUC: area under the receiver operating characteristic curve; SD: standard deviation
Ethical considerations and barriers to adoption
Algorithmic Bias
Studies show lower AI model accuracy in women and ethnic minorities due to underrepresentation in training datasets [23]. For example, an AI liver fibrosis model trained on predominantly male viral hepatitis cohorts showed reduced accuracy in female patients with NASH, highlighting population bias concerns.
Explainability and Trust
Lack of interpretability hinders clinician confidence and regulatory approval. Emerging explainability tools like SHAP and LIME may help clinicians understand AI decision pathways, improving trust and adoption.
Privacy and Security
Wearable and cloud-integrated systems must comply with strict HIPAA/GDPR data regulations [24]. Similarly, a 2025 multicenter prospective validation demonstrated deep learning models achieving high sensitivity for early hepatocellular carcinoma detection, further highlighting AI’s potential for liver cancer surveillance [25]. Recent international studies have successfully used federated learning to harmonize liver fibrosis staging models across diverse cohorts without compromising data privacy [26].
Emerging solutions include: Federated learning to train AI models without centralizing patient data; Explainable AI (XAI) frameworks for interpretable decision-making; Independent regulatory sandboxes to test AI tools under controlled conditions before scaling.
Future research priorities
Multimodal Integration
Combining imaging, lab biomarkers, genomics, and wearables for holistic disease profiling. Developing prospective randomized trials to test AI-assisted surveillance pathways against standard hepatology care is essential to establish real-world benefit.
Federated Data Collaboratives
Global consortia ensuring diverse, representative datasets for equitable AI.
Prospective Clinical Trials
Evaluating AI-assisted care pathways vs. standard hepatology practice for real-world impact. Explainable and Patient-Centered AI: Co-developing models with patient advocates and hepatologists for transparent deployment.
Conclusions
AI and digital biomarkers hold great promise for earlier detection and improved management of liver diseases. However, they are complementary to, not replacements for, conventional scoring systems at present. For successful clinical adoption, external validation, equitable datasets, and integration into EMR workflows are essential. The future of the field of hepatology will depend on collaborative efforts between clinicians, data scientists, regulators, and patients to ensure safe, ethical, and meaningful use of AI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burden of liver diseases in the world J Hepatol Asrani SK Devarbhavi H Eaton J Kamath PS 1511717020193026628210.1016/j.jhep.2018.09.014 · doi ↗ · pubmed ↗
- 2The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 Lancet Gastroenterol Hepatol GBD 2017 Cirrhosis Collaborators 245266520203198151910.1016/S 2468-1253(19)30349-8PMC 7026710 · doi ↗ · pubmed ↗
- 3Liver biopsy Hepatology Rockey DC Caldwell SH Goodman ZD Nelson RC Smith AD 101710444920091924301410.1002/hep.22742 · doi ↗ · pubmed ↗
- 4A guide to deep learning in healthcare Nat Med Esteva A Robicquet A Ramsundar B 24292520193061733510.1038/s 41591-018-0316-z · doi ↗ · pubmed ↗
- 5The digital transformation of hepatology: the patient is logged in Hepatology Wu T Simonetto DA Halamka JD Shah VH 1131113375202210.1002/hep.32329 PMC 953118535028960 · doi ↗ · pubmed ↗
- 6Deep learning with ultrasonography: automated classification of liver fibrosis using a deep convolutional neural network Eur Radiol Lee JH Joo I Kim KW Shin J Han JK Choi BI 126412733020203147808710.1007/s 00330-019-06407-1 · doi ↗ · pubmed ↗
- 7Contemporary use of elastography in liver fibrosis and portal hypertension Clin Physiol Funct Imaging Thiele M Kjaergaard M Thielsen P Krag A 2352423720172645918410.1111/cpf.12297 · doi ↗ · pubmed ↗
- 8Deep learning radiomics of shear-wave elastography significantly improved diagnostic performance for assessing liver fibrosis in chronic hepatitis B: a multicenter study Gut Wang K Lu X Zhou H 7297416820192973060210.1136/gutjnl-2018-316204 PMC 6580779 · doi ↗ · pubmed ↗