Atraumatic Tension Pneumocephalus in a Shunted Patient: A Case of Rapid Neurological Decline
Lily D Rundquist, Jomaris O Gomez-Rosado, Christopher Nunez, Aleksandr Dubrovskiy

TL;DR
This paper presents a case of a shunted patient who rapidly declined due to a rare condition called tension pneumocephalus, stressing the importance of early detection and treatment.
Contribution
The paper adds to the clinical literature by highlighting the rare but severe complication of tension pneumocephalus in VP shunt patients.
Findings
A 83-year-old VP shunt patient experienced acute neurological decline due to severe tension pneumocephalus.
Despite surgical intervention, the patient developed a subdural hematoma and poor neurological recovery.
The case underscores the need for prompt recognition and management of tension pneumocephalus in shunted patients.
Abstract
Pneumocephalus is a rare but potentially life-threatening condition caused by the presence of air within the intracranial cavity. It commonly arises from trauma, neurosurgical procedures, infections, malignancies, or spontaneous causes. In patients with ventriculoperitoneal (VP) shunts, pneumocephalus may result from complications such as altered cerebrospinal fluid dynamics or skull base defects leading to a vacuum-like effect. We report a case of an 83-year-old male with a history of VP shunt placement for normal pressure hydrocephalus who presented with acute neurological deterioration, including aphasia and quadriparesis. Imaging revealed severe frontal pneumocephalus with mass effect and midline shift. The patient underwent emergent burr hole evacuation and VP shunt removal. Despite surgical intervention, he developed a new sizable subdural hematoma, leading to further…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
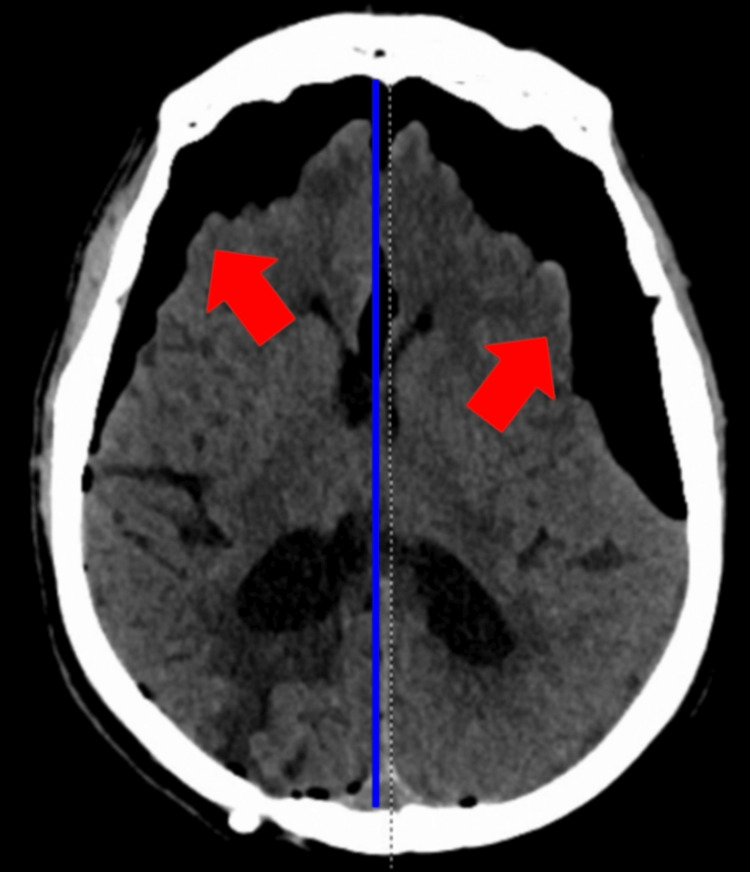 Figure 1
Figure 1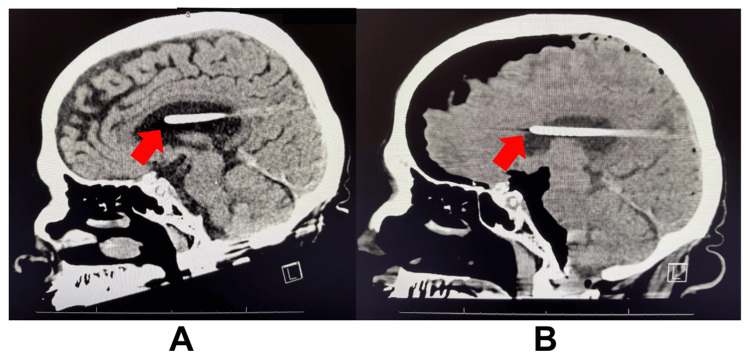 Figure 2
Figure 2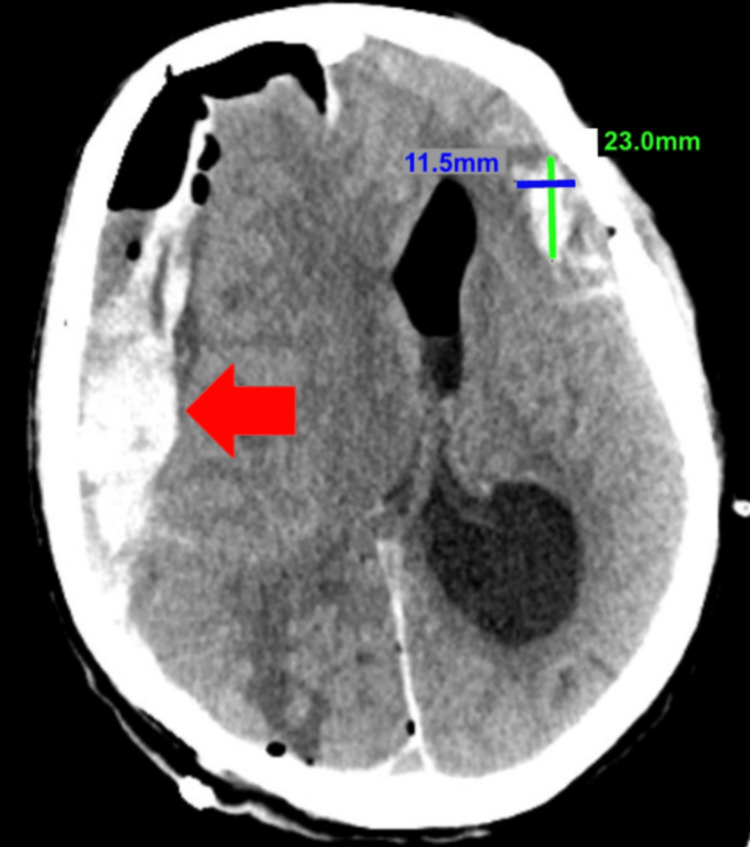 Figure 3
Figure 3| Stages of Patient Presentation | Clinical Status | Imaging/Findings | Interventions | Patient Outcome |
| Baseline | Alert, oriented, ambulatory with walker; required ADL assistance | Prior right VP shunt, left SDH evacuated 1 month prior | Routine care | Stable at baseline |
| Acute Presentation | Sudden inability to move, global aphasia, NIHSS 29 | Severe frontal pneumocephalus (L>R), 4 mm midline shift, right parietal encephalomalacia; VP shunt slightly anterior | Stroke alert called, BiPAP support | Rapid neurological deterioration |
| During Hospital Stay | Disoriented and eventually unresponsive | Same as in acute presentation | Left burr hole evacuation, VP shunt removal, intubation, antibiotics, ICU care | Partial resolution of pneumocephalus; continued poor neurological status |
| Final Outcome | Unresponsive, minimal improvement | Follow-up CT showed partial resolution of pneumocephalus and a new SDH | Right-sided craniotomy for new SDH; later hospice care, DNR | Compassionate extubation; patient deceased |
| Article | Mechanism of Pneumocephalus | Onset Timing Post-Shunt Placement | Location of Defect | Interventions | Key Notes/Outcome |
| Kim et al. (2009) - Otogenic Pneumocephalus Associated with a VP Shunt | Otogenic mechanism: Negative intracranial pressure via VP shunt + mastoid/skull base bony defect | 29-30 months post-shunt placement | Posterior fossa, mastoid | Mastoidectomy, Defect repair with muscle plug and bone dust | Patient had tinnitus; successful resolution |
| da Silva et al. (2021) - Intraventricular Pneumocephalus as a Complication of VP Shunt | Combination of shunt siphon effect + anatomical defect enabling air entry | Greater than 10 years post-shunt placement | Bony defect and meningocele (fistula) at the base of the skull | Bicoronal craniotomy; meningocele closure; frontal sinus cranialization; new VP shunt placed | Specifically discusses air entering the skull when nasal pressure is greater than intracranial pressure when the basal structures are connected to the paranasal sinuses via an opening |
| Pieri et al. (2011) - Delayed Otogenic Tension Pneumocephalus Complicating VP Shunt | Air entry via petrous apex/tegmen tympani defect + shunt effect | 12 months post-shunt placement | Petrous bone/temporal region | Temporarily raised shunt pressure; surgical defect repair | Emphasizes surgical correction of anatomical defect, complicated by aneurysmal subarachnoid hemorrhage |
| Monas et al. (2010) - Spontaneous Tension Pneumocephalus Resulting From a Scalp Fistula in a Patient With a Remotely Placed VP Shunt | Shunt negative pressure + skull defect (scalp fistula) | 4-5 years post-shunt | Frontal parietal region | Percutaneous decompression in the ED, scalp wound debridement and skin closure, broad-spectrum antibiotics | Skull defect due to infection eroding through the overlying tissue of an old burr hole |
| Verhaeghe et al. (2018) - Delayed Intraventricular Pneumocephalus Following Shunting for Normal-Pressure Hydrocephalus | Bone erosion + shunt negative pressure | 10 months post-shunt | Left temporal region/mastoid | Tegmen repair with flap | Delayed complication due to bone erosion secondary to long-standing intracranial pressure |
| Gkasdaris et al. (2024) - Spontaneous Intraventricular Tension Pneumocephalus | Chronic intracranial hypertension + thinness of bony area at the superior edge of the petrous pyramid | Multiple VP shunt placements; time frame not listed | Between left temporal bone and tegmen tympani; intraventricular | Middle cranial fossa surgery with repair of osteo-meningeal breach | Past medical history of tumor in the pineal region |
| Alalawi et al. (2025) - Atypical Presentation of Pneumocephalus Post-VP Shunt in a Patient with a History of Endoscopic Endonasal Skull Base Approach: A Case Report | Siphon effect from VP shunt/excessive negative intracranial pressure + postoperative skull base defect | 3 days post-shunt | Right petrous apex/middle cranial fossa with brainstem compression | Endoscopic skull base defect repair, fat graft, excessive irrigation | Large extra-axial tumor in the right middle cranial fossa → tumor removal → acute hydrocephalus due to meningitis → VP shunt → pneumocephalus |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Surgical Oncology · Infectious Diseases and Tuberculosis · Spinal Dysraphism and Malformations
Introduction
Pneumocephalus, the presence of air within the intracranial cavity, is a rare but potentially life-threatening condition that can lead to significant neurological defects [1]. It is most commonly associated with head trauma, neurosurgical interventions such as ventriculoperitoneal (VP) shunt placement, infections, malignancy, or spontaneous causes [1,2]. Pneumocephalus is classified into two categories: simple pneumocephalus and tension pneumocephalus. Simple pneumocephalus is often asymptomatic, following a procedure such as a craniotomy or burr hole placement. They are benign and self-limiting [3,4]. Tension pneumocephalus occurs when intracranial air accumulates under pressure, causing brain compression and mass effect [4,5]. This leads to increased intracranial pressure (ICP) with symptoms such as headache, altered mental status, nausea, vomiting, neurological deficits, and, in severe cases, death [5]. In patients with VP shunts, pneumocephalus can arise due to altered cerebrospinal fluid (CSF) flow or skull base defects, which create a vacuum for air trapping [6,7]. Limited data exist on the prevalence of this complication; however, prior studies have documented cases in patients with longstanding VP shunts, often presenting with symptoms of shunt dysfunction and elevated ICP [6,8].
Here, we report a case of severe tension pneumocephalus in an elderly patient with a history of VP shunt placement, leading to rapid neurological deterioration and necessitating emergent neurosurgical intervention. This case highlights the unique interplay between VP shunts and cranial defects, demonstrating how shunt-induced negative pressure can exacerbate air entry and accelerate neurological decline, an uncommon but significant teaching point for medical professionals.
Case presentation
An 83-year-old male with a past medical history of hypertension, hyperlipidemia, diabetes mellitus, depression, normal pressure hydrocephalus status post right VP shunt placed five years ago, and left subdural hematoma (SDH) evacuated one month prior, presented to the Emergency Department via Emergency Medical Services (EMS) as a stroke alert. The family reported he was at baseline when he suddenly became unable to move, exhibiting a blank stare, global aphasia, and inability to follow commands, prompting an Emergency Services (911) call. Baseline function included ambulation with a walker and self-feeding, with assistance needed for other activities of daily living. The family reported no recent trauma, fever, chest pain, or shortness of breath (SOB).
On arrival, he was hemodynamically unstable (BP 167/101 mmHg, HR 53-68 bpm) and on BiPAP with mild respiratory alkalosis (pH 7.43, pCO2 36, pO2 112). The exam revealed disorientation, minimal responsiveness, partial gaze palsy, complete facial paralysis, global aphasia, 0/5 strength, severe sensory loss in all extremities, and an NIHSS Stroke Scale (NIHSS) score of 29. He was normocephalic, atraumatic, with a well-healed left parietal craniotomy scar and no signs of infection or trauma. A chronic heart murmur was noted, with chronicity based on notes from previous hospital admissions. The patient was breathing comfortably on BiPAP, the abdomen was soft, non-distended, and non-tender.
Emergent non-contrast computed tomography (CT) of the brain showed severe frontal pneumocephalus (L>R) with mass effect, a 4 mm rightward midline shift, and right parietal encephalomalacia (Figure 1). The VP shunt appeared slightly anterior compared to prior imaging (Figure 2). The patient was intubated for airway compromise, started on broad-spectrum antibiotics, and neurosurgery was consulted. A VP shunt imaging series was ordered to assess the function and placement of the device, which proved unremarkable. The pneumocephalus was visualized, and the VP shunt catheter had no evidence of fractures.
Non-contrast CT brain before neurosurgical intervention, depicting severe frontal pneumocephalus (left greater than right), with air extension in the skull and right parietal encephalomalacia, indicated by the red arrows. There is also a 4 mm rightward midline shift, with the midline depicted by the dashed line and the shifted midline depicted by the blue line.
Non-contrast CT brain depicting the shift in VP shunt. Picture A shows the VP shunt inside the lateral ventricle from imaging during a prior admission. Picture B shows the VP shunt shifted slightly anterior compared to the position in picture A. The anterior tip of the VP shunts is indicated by the arrows.
The neurosurgical team performed an emergent left-sided burr hole evacuation and VP shunt removal via a right posterior occipital incision. The procedure aimed to relieve ICP by allowing air drainage and reducing mass effect. Although a bilateral procedure was initially considered, intraoperative findings suggested adequate decompression with left-sided intervention alone. Postoperatively, he remained in the intensive care unit on mechanical ventilation.
Despite intervention, his neurological status remained poor. Follow-up CT brain revealed a new right-sided SDH (Figure 3). Neurosurgery discussed the poor prognosis with the patient’s family, who initially opted for maximal medical and surgical management. The patient subsequently underwent a right-sided craniotomy. Post-operatively, he remained unresponsive, with questionable seizure activity. Given the lack of improvement and poor prognosis, the family declined further interventions, and he was transitioned to a do-not-resuscitate status and hospice care, with compassionate extubation performed. Table 1 summarizes the patient’s clinical course from baseline through interventions and outcomes.
Non-contrast CT brain post-procedure depicting the partial resolution of intracranial air and a new right-sided SDH depicted by the arrow. There is also a small bleed on the left side, measuring 23.0 mm by 11.5 mm.SDH: Subdural hematoma
Discussion
This case highlights the potential development of tension pneumocephalus secondary to micro-openings at a healing burr hole site. This led to air trapping that was rapidly exacerbated by the VP shunt, resulting in acute clinical deterioration. Atraumatic pneumocephalus is a rare and life-threatening complication that warrants prompt recognition and intervention. This case is particularly unique due to its mechanism and rapid progression, offering valuable insight into an uncommon but serious postoperative risk that should be considered in patients with VP shunts and recent cranial procedures.
A month prior to this admission, the VP shunt was placed at a high setting performance of 2.5 (140 mm Hg drainage pressure) to aid the evacuation of the left SDH. A higher shunt pressure setting was chosen to minimize CSF drainage and prevent overdrainage, which can lead to negative pressure in the subarachnoid space and subsequent expansion of the SDH due to tearing of bridging veins or brain shifting. Despite these precautions, the patient required surgical evacuation of the hematoma through a left burr hole. On follow-up visits, a well-healed surgical scar on the left parietal scalp was noted; no skin breakdown or signs of infection. The patient was progressively improving and returned to his domiciliary environment.
Tension pneumocephalus is a known complication of cranial trauma and acute VP shunt placement [2]. However, this patient had no recent head trauma, and the VP shunt was placed over five years ago. This prompted the question of how an acute and atraumatic tension pneumocephalus could develop with such rapid onset and neurological deterioration.
The literature supports that micro-openings in the previous left parietal burr hole surgical scar allowed small amounts of air to enter the intracranial space. The negative pressure from the VP shunt created a vacuum, which facilitated the rapid introduction of air into the brain cavity. This led to the quick expansion and entrapment of air, hence a tension pneumocephalus [9]. The literature also indicates that the combination of a VP shunt and a cranial defect or fistula may provide a route for air to enter the cranial cavity [9,10]. We believe the negative pressure from the VP shunt caused the acute presentation of this tension pneumocephalus and rapid neurological deterioration in the patient. Table 2 below summarizes seven case studies to highlight the similarities and differences between cases of atraumatic pneumocephalus in patients with VP shunts.
The patient's presentation and subsequent imaging findings highlight the importance of careful monitoring and timely intervention in patients with VP shunts who are experiencing neurological deterioration. Adjusting the shunt pressure settings to prevent overdrainage and regular follow-up imaging can help mitigate the risk of complications such as SDH expansion and pneumocephalus. This case underscores the need for a multidisciplinary approach, involving neurosurgery, critical care, and infectious disease specialists, to optimize patient outcomes in complex cases involving VP shunts.
Conclusions
Tension pneumocephalus is a rare but serious complication. Patients with VP shunts who underwent additional cranial procedures appeared to be at higher risk due to potential micro-openings. This case illustrates how a healing cranial defect, combined with shunt-induced negative pressure, can rapidly lead to life-threatening neurological decline. Early recognition and timely neurosurgical intervention are crucial. This case reinforces the need for vigilance in patients with VP shunts who develop new neurological decline, emphasizing the importance of considering pneumocephalus in the differential diagnosis even in the absence of trauma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spontaneous pneumocephalus: a case report with a literature review J Emerg Med Chen J Wang S Huang CY Wu YH Hsieh CC 51752165202310.1016/j.jemermed.2023.06.01337838493 · doi ↗ · pubmed ↗
- 2Pneumocephalus In: Stat Pearls [Internet] Das JM Munakomi S Bajaj J Treasure Island, FL Stat Pearls Publishing LLC 2024 https://www.ncbi.nlm.nih.gov/books/NBK 535412/
- 3Chapter 5 - Pneumocephalus Complications in Neuroanesthesia Prabhakar H Bithal P 3539 Academic Press 2016
- 4What should an intensivist know about pneumocephalus and tension pneumocephalus?Acute Crit Care Wankhade BS Beniamein MM Alrais ZF Mathew JI Alrais GZ 2442483820233554524210.4266/acc.2021.01102 PMC 10265419 · doi ↗ · pubmed ↗
- 5Tension pneumocephalus Braz J Anesthesiol Khanna S Trombetta C Ruetzler K Argalious M 8348357320233751758610.1016/j.bjane.2023.07.005PMC 10625142 · doi ↗ · pubmed ↗
- 6Intraventricular pneumocephalus as a complication of ventriculoperitoneal shunt Cureus da Silva AJ Malta Doria AL 013202110.7759/cureus.18392 PMC 855592034725626 · doi ↗ · pubmed ↗
- 7Otogenic pneumocephalus associated with a ventriculoperitoneal shunt Clin Exp Otorhinolaryngol Kim YH Lee WI Park MN Choi HS Kim NH Han SJ 203206220092007269610.3342/ceo.2009.2.4.203PMC 2804097 · doi ↗ · pubmed ↗
- 8Incidence and perioperative management of tension pneumocephalus following craniofacial resection J Neurosurg Anesthesiol Yates H Hamill M Borel CO Toung TJ 152061994829825910.1097/00008506-199401000-00002 · doi ↗ · pubmed ↗