Comparison of the Efficacy of Continuous Saline Infusion to Prevent Catheter Occlusion: A Systematic Review and Meta-Analysis
Shunsuke Kondo, Yusuke Hirao, Shunsuke Yasuo, Yasushi Tsujimoto

TL;DR
This study compares continuous saline infusion to standard care for preventing catheter blockage in critically ill patients, finding it may reduce occlusion risk but with low certainty.
Contribution
The study provides a meta-analysis of continuous saline infusion's efficacy in preventing catheter occlusion in high-risk patients.
Findings
Continuous saline infusion reduced occlusion risk by 49% compared to standard care, with low certainty.
No significant difference in catheter-related bloodstream infections between groups.
Adverse events were rare and mainly involved leakage at the catheter site.
Abstract
Central venous catheters (CVCs) are essential in managing critically ill patients but are frequently complicated by occlusion, which can necessitate catheter replacement and increase the risk of complications such as catheter-related bloodstream infection (CRBSI). Continuous saline infusion devices have emerged as a potential intervention to maintain catheter patency, as continuous fluid administration is the common measure of fluid administration, though a persistently high occlusion rate remains in the high-risk population. This systematic review and meta-analysis assessed the efficacy of continuous saline infusion versus standard of care, including intermittent flushing and catheter lock, in preventing catheter occlusion. We searched MEDLINE, Embase, Cochrane CENTRAL, ClinicalTrials.gov, and the WHO International Clinical Trials Registry Platform (ICTRP) up to February 11th, 2025.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
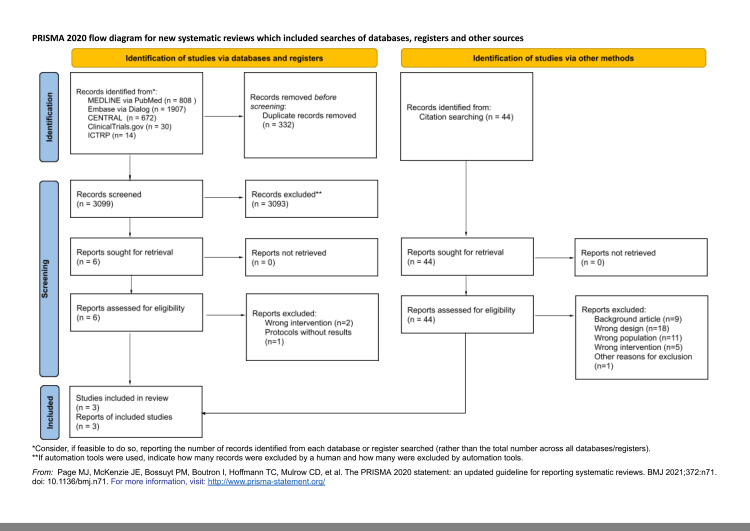 Figure 1
Figure 1 Figure 2
Figure 2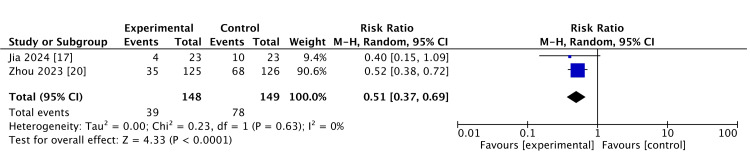 Figure 3
Figure 3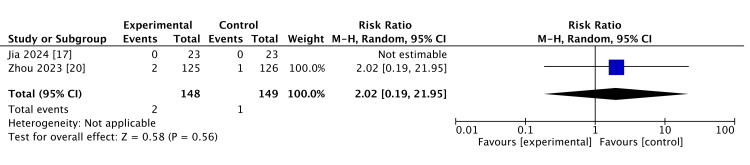 Figure 4
Figure 4| Study/country | N | Follow-up duration (days) | Population | Site of catheter (n) | Percent female | The main reason for ICU admission | Standard of care |
| RCTs | |||||||
| Zhou et al. (2024) [ | 251 | 7 | Patients aged 14 to 80 years admitted to the hospital, who had a new centrally inserted central catheter placed within 24 hours, and the catheter was placed via the internal jugular or subclavian vein | Subclavian vein: 24. Internal jugular vein: 227 | 36.7% | Not reported | 10 mL of saline was used to flush and positive pressure locking |
| Jia et al. (2024) [ | 46 | 7 | Patients aged 14 to 80 years admitted to ICUs who had a new centrally inserted central catheter placed within 24 hours, and the catheter was placed via the internal jugular or subclavian vein | Subclavian vein: 4. Internal jugular vein: 42 | 58.7% | Pneumonia = 10; abdominal pain = 6; acidosis = 5; pancreatitis/cholecystitis = 9; digestive tract perforation = 3; multiple site damage = 4; other reasons = 9 | 10 mL of saline was used to flush and positive pressure locking every 6 hours |
| Li et al. (2024) [ | Aim for 250 | - | Patients aged 14 to 80 years admitted to ICUs who had a new centrally inserted central catheter placed within 24 hours, and the catheter was placed via the internal jugular or subclavian vein | - | - | - | 10 mL of saline was used to flush and positive pressure locking every 6 hours |
| Outcomes | Anticipated absolute effects risk with the intermittent manual injection of the solution* | Anticipated absolute effects risk with the continuous catheter flushing technique* | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments |
| Catheter occlusion rate | 523 per 1,000 | 267 per 1,000 (194 to 361) | RR: 0.51 (0.37 to 0.69) | 297 (2 RCTs) | ⨁⨁◯◯ Lowa,b | Continuous catheter flushing technique may reduce the catheter occlusion rate. |
| Catheter-related bloodstream infection (CRBSI) | 0 per 1,000 | 10 per 1,000 (0 to 247) | RR: 3.02 (0.12 to 73.52) | 297 (2 RCTs) | ⨁⨁◯◯ Lowa,b | CRBSI may not be affected by continuous catheter flushing. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Diagnosis and Treatment of Venous Diseases · Vascular Procedures and Complications
Introduction and background
Central venous catheters (CVCs) are widely used, especially for critically ill or perioperative patients [1]. They help measure hemodynamic variables that non-invasive methods cannot accurately assess and allow the safe delivery of blood products, medications, and nutrition when peripheral vein catheters are unsuitable. In the critically ill setting, CVCs are the route of vasopressors or nutrition, which cannot be delivered via a peripheral vein catheter [2]. Another common use of CVCs is for hemodialysis vascular access. In the ICU setting, bolus fluid administration is the common measure to deliver fluid to patients with CVC [3]. Even in the sepsis population, bolus fluid administration is mainly used to give IV fluid, as around 8.6% receive bolus fluid administration [4].
CVC occlusion is a frequent problem that often requires catheter removal or exchange. It increases the risk of CVC-related complications, such as catheter-related bloodstream infections (CRBSIs) and increased healthcare costs [5,6]. Current guidelines recommend intermittent normal saline flushing to prevent catheter occlusion, as multiple systematic reviews and meta-analyses, including recent Cochrane reviews and large randomized trials, demonstrated that intermittent heparin flushing has similar efficacy with no significant rate of catheter occlusion [7-9]. Normal saline intermittent flushing is generally recommended due to its lower cost and avoidance of heparin-associated risks, such as heparin-induced thrombocytopenia [10]. The National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) and the American Society of Clinical Oncology both recommend routine saline flushing as standard practice [11,12]. Despite the effort, a previous study reported that CVCs experience occlusion rates of approximately 4.95% within one week [13]. Catheter occlusion happens more frequently in ICUs because of the severity of the patients, non-standardized care, and the more frequent urgent catheter placement compared to the general wards, and the occlusion rate goes up to 33% in 10 weeks [14]. Also, catheter-related thrombosis is a more frequently reported complication, with one study noting a prevalence of 56% in ICU patients and approximately 14% to 18% in the general population [15,16].
Recently, continuous infusion devices have been developed as a novel approach to maintain catheter patency and prevent occlusion. These devices, utilizing continuous infusion technology, are used to deliver flushing fluid into the CVCs at a precise and steady rate of 2 mL per hour [17]. While a recent study demonstrated that heparin locking may be more effective than 0.9% sodium chloride locking for preventing occlusion in CVCs [18], evidence remains limited regarding optimal strategies for maintaining catheter patency and preventing occlusion [19]. In this context, continuous infusion devices have attracted attention, and several randomized controlled trials have evaluated their effectiveness, and both studies showed favorable outcomes [17,20]. However, no systematic review or meta-analysis has evaluated the efficacy of continuous infusion for catheter maintenance. We conducted a systematic review to evaluate the effectiveness of continuous infusion to prevent catheter occlusion.
Review
Methods
We followed a pre-specified protocol [21]. The difference between the protocol and this review is provided in Supplement 1. We adhered to the Cochrane handbook [22], Grading of Recommendations Assessment, Development, and Evaluation (GRADE) informative statement [23], and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [24] when preparing this protocol and reporting the present study.
Eligibility Criteria
Types of studies: We included randomized controlled trials (RCTs), randomized crossover trials, and cluster RCTs that assess the efficacy of continuous flushing as compared to manual injection of saline. We did not apply language or country restrictions. We included all papers, including published, unpublished articles, abstracts of conferences [23], and letters.
We excluded non-randomized studies of interventions, such as quasi-experimental studies or observational studies. We did not exclude studies based on the observation period or publication year.
Study participants: Adult patients older than 16 years with a CVC, temporary hemodialysis catheter, or a peripheral insertion central catheter placement within 24 hours, regardless of the insertion site, were included.
The exclusion criteria were patients who must use alternative fluids for catheter locking; patients who need to use drugs that are incompatible with normal saline, such as lorazepam; patients who need to use drugs that cannot tolerate the cessation of infusion for catheter flushing. Patients receiving 24 hours of continuous infusion of the medications who do not require a lock to prevent obstruction were also excluded.
Intervention and Control
The intervention group used continuous normal saline infusion with a pre-filled elastic bag or syringe pump, which delivers fluid at a constant rate over 24 hours. The control group received standard care, which includes manual pulsatile normal saline flush or heparin solution flush at least every 24 hours with positive pressure lock or citrate lock. If medication is given through that catheter, the catheter is locked with positive pressure normal saline or heparin solution at the end of the infusion without routine additional positive pressure lock every 24 hours.
Outcomes
The primary outcomes of interest were catheter occlusion, which is defined by the Catheter Injection and Aspiration (CINAS) classification [25], incidence rate of CRBSI, and catheter-related thrombosis. Secondary outcomes of this study were CVC removal without a pre-specified plan and all adverse events.
Search Strategy
We searched the following databases: MEDLINE (PubMed), the Cochrane Central Register of Controlled Trials (Cochrane Library), and Embase (Dialog). The search strategies are listed in Appendix B. We also searched the US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) and the WHO International Clinical Trials Registry Platform (ICTRP), listed in Appendix B. Also, we checked the reference lists of studies, including the reference lists of eligible studies and articles citing eligible studies. The search was conducted in February 2025. We asked the authors of original studies for unpublished or additional data.
Data Collection and Analysis
Selection of the studies: Two reviewers (SK and YH) performed independent data extraction of the included studies using a standardized data collection form. Any disagreements were resolved by discussion, and if this failed, a third reviewer acted as an arbiter (SY).
Assessment of risks of bias in included studies: Two reviewers (SK and YH) evaluated the risk of bias independently using the Risk of Bias 2 tool [26]. Disagreements between the two reviewers were discussed, and if this failed, a third reviewer (SY) acted as an arbiter, if necessary.
Data synthesis: Meta-analysis was performed using Review Manager software (RevMan 5.4.1, Cochrane Collaboration, London, UK). We used a random-effects model for meta-analysis. We pooled the relative risk ratios (RRs) and the 95% confidence intervals (CIs) for the following binary variables: number of occlusions of the catheter. We pooled the mean differences and the 95% CIs for the following continuous variables: catheter occlusion rate. If several different scales have been used in the included studies, we pooled the effect estimates using standard mean differences (SMDs). We summarized adverse events based on the definition by the original article, but we did not perform a meta-analysis. We performed the intention-to-treat (ITT) analysis for all dichotomous data as much as possible. For continuous data, we did not impute missing data based on the recommendation by the Cochrane handbook [22]. We performed a meta-analysis of the available data in the original study. When original studies only report standard error or p-value, we calculated the standard deviation based on the method by Altman and Bland [27]. If we do not know these values when we contact the authors, the standard deviation was calculated by confidence interval and t-value based on the method mentioned in the Cochrane handbook [22], or a validated method [28,29].
We evaluated the statistical heterogeneity by visual inspection of the forest plots and calculating the I2 statistic (I2 values of 0% to 40%: might not be important; 30% to 60%: may represent moderate heterogeneity; 50% to 90%: may represent substantial heterogeneity; 75% to 100%: considerable heterogeneity). When there is substantial heterogeneity (I2 > 50%), we assessed the reason for the heterogeneity. Cochran's chi^2^ test (Q-test) was performed for the I2 statistic, and a p-value less than 0.10 was defined as statistically significant.
We searched the clinical trial registry system (ClinicalTrials.gov and ICTRP) and performed an extensive literature search for unpublished trials. To assess outcome reporting bias, we compared the outcomes defined in trial protocols with the outcomes reported in the publications.
Rating the certainty of evidence: Two reviewers (SK and YH) evaluated the certainty of evidence based on the GRADE approach [30]. Disagreements between the two reviewers were discussed, and if this failed, a third reviewer (SY) acted as an arbiter, if necessary.
A summary of findings table was made for the following outcomes based on the Cochrane handbook [22]: catheter occlusion, CRBSI, catheter-related thrombosis, and unexpected catheter removal.
Results
A total of 3,099 records were identified from the electronic database search, and 44 records were identified from the citation search. We retrieved full texts of six reports from the electronic database and 44 reports from citation searches for full assessment. Of these six full-text articles, we included three studies in our review, and one of them is an ongoing study, which is shown in Figure 1. The references of the excluded studies and the reasons for exclusion are summarized in Appendix C.
PRISMA (2020) flow diagram for a new systematic review, which included searches of databases, registers, and other sources.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 1 shows the characteristics of the three included studies. All the included studies assessed the impact of the continuous normal saline infusion. Among the three studies, one study was not published, and the data were not available [31]. We found that the study participants were from the general population in one study [20], and one study included only critically ill patients [17]. Comparison of both studies was intermittent normal saline flushing. As only two studies were available, we performed a meta-analysis using these studies.
Primary Outcomes
We summarize the risk of bias in the outcomes of catheter occlusion rate and incidence rate of CRBSI in Figure 2. Both of the studies had an overall high risk of bias [17,20].
Summary of risk of bias.References: Jia et al. [17]; Zhou et al. [20].
Catheter occlusion rate: Both studies were included in the meta-analysis. Continuous catheter flushing technique may reduce catheter occlusion rate (RR: 0.51, 95% CI: 0.37 to 0.69, I2 = 0%; two studies, 279 participants, low certainty of evidence). This is shown in Figure 3.
Catheter occlusion rate.
Incidence rate of CRBSI: Two studies reported CRBSI as an outcome measure. One study reported that there was no CRBSI in either the intervention or control groups. CRBSI may not be affected by continuous catheter flushing (RR: 3.02, 95% CI: 0.19 to 21.95; heterogenicity not applicable; two studies, 279 participants). This is shown in Figure 4.
Incidence rate of catheter-related bloodstream infections (CRBSIs).
Incidence rate of catheter-related thrombosis: Only one study reported this outcome. They reported no events in both intervention and control groups during the study period.
Secondary Outcomes
One study did not report catheter-related thrombosis and catheter removal without a pre-specified plan, although it was planned to measure in the protocol [20]. We sent emails twice to authors asking for the detailed outcome data of the incidence of catheter-related thrombosis and CVC removal without a pre-specified plan, but they did not respond, so no additional data are available. CVC removal without a pre-specified plan was reported in one study. They reported no events in both intervention and control groups during the study period. All adverse events were reported as qualitative synthesis and reported in the summary of findings table (Table 2 and Appendix A).
Discussion
This systematic review found that the continuous catheter flushing technique may improve the catheter occlusion rate in patients who have CVCs placed within 24 hours compared to intermittent fluid administration, with low certainty of evidence. Our study also showed that the incidence rate of CRBSI may not be increased by using continuous catheter flushing. Only one study reported on the other clinically important outcomes, such as incidence of catheter-related thrombosis or catheter removal according to a pre-specified plan, but no events were observed. The main adverse event noted was leakage, and the incidence rate was low.
Continuous saline flushing demonstrates comparable effectiveness to other established interventions in preventing catheter occlusion. One meta-analysis reported that the intermittent heparin flushing was associated with a reduced risk of catheter occlusion by approximately 30-40% compared to intermittent saline flushing in patients with newly placed CVCs during the first 30 days [9]. Standardization of care for CVCs, which demonstrated improvement in occlusion rate in a previous systematic review [32], showed a 69% reduction without heterogenicity of the studies. Our study showed that catheter occlusion with the continuous flushing technique may reduce occlusion (RR: 0.51), though the overall number of catheter occlusions is lower in both intervention and comparison groups compared to the previous studies [15,16]. Also, CVCs made using new materials could prevent further occlusive events, though there is no available report focusing on the acute setting, as one report showed improvement in the long-term catheter placement [33]. Clinicians can apply continuous normal saline flushing with the standardized nursing education or new material CVCs, and this intervention may provide additional benefits in reducing the catheter occlusion rate. Patients who cannot receive heparin may also benefit from this intervention.
Although the possible downside of the continuous normal saline flushing is CRBSI, our study shows that it may not increase the rate of these complications. The rate of CRBSI is reported to be around 4.4% in the previous study [34], or 3.5 per 1000 catheter-days in high-income countries, as reported by the International Society for Infectious Diseases [35]. In contrast, we did not observe CRBSI in the control groups of the included study. We found more incidence of CRBSI in continuous normal saline flushing groups, but the absolute difference was modest.
Our review also highlights the need for future investigation to confirm the potential use of continuous saline infusion, as many of the outcomes in this review left uncertainty. The incidence rate of catheter-related thrombosis in our study was zero, whereas previous studies reported the incidence rate as 56% in ICU patients and 14% to 18% in the general population [15,16]. We therefore rated the certainty of evidence on this outcome as very low. CVC removal without a pre-specified plan was also not reported in one study and reported as zero in the other study. The adverse event rate in our study was higher compared to the previous studies, as 2-4 per 1000 insertions [5]. Studies included in our review counted minor adverse events such as leakage, which might increase the rate. One study with an expected sample size of 250 is ongoing, but larger RCTs measuring clearly defined important outcomes are needed to confirm our findings [31].
Our study has several limitations. First, we were able to find only two articles with results and one additional protocol. This device is new, and there are not many published studies yet. Second, we cannot perform the subgroup analysis or sensitivity analysis because the data are limited, and the author did not respond to our inquiry. Third, we could not obtain unpublished data on catheter-related thrombosis and catheter removal, though we had contacted the original investigators.
Despite these limitations, this study first summarized the efficacy of the continuous normal saline flushing compared to the intermittent catheter flushing technique.
Our study has several strengths. We followed the standard methods such as the Cochrane handbook and GRADE approach [22,30], and we did a comprehensive search, including unpublished protocols.
Conclusions
In conclusion, clinicians may consider using continuous saline infusion devices for patients at high risk of catheter occlusion. However, our review also highlights several uncertainties that warrant attention when applying this intervention. Well-designed RCTs with larger sample sizes are needed to provide more definitive conclusions regarding the efficacy of this intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Insertion site of central venous catheter among hospitalized adult patients: a systematic review and network meta-analysis Front Med (Lausanne) Sakuraya M Okano H Yoshihiro S Niida S Kimura K 960135920223610631610.3389/fmed.2022.960135 PMC 9464814 · doi ↗ · pubmed ↗
- 2Medical-grade honey does not reduce skin colonization at central venous catheter-insertion sites of critically ill patients: a randomized controlled trial Crit Care Kwakman PH Müller MC Binnekade JM van den Akker JP de Borgie CA Schultz MJ Zaat SA 016201210.1186/cc 11849 PMC 368231823111148 · doi ↗ · pubmed ↗
- 3Fluids in the ICU: which is the right one?Nephrol Dial Transplant Mayerhöfer T Shaw AD Wiedermann CJ Joannidis M 160316123820233617096210.1093/ndt/gfac 279PMC 10310506 · doi ↗ · pubmed ↗
- 4Fluid boluses and infusions in the early phase of resuscitation from septic shock and sepsis-induced hypotension: a retrospective report and outcome analysis from a tertiary hospital Ann Intensive Care Messina A Albini M Samuelli N 1231420243914795710.1186/s 13613-024-01347-6PMC 11327232 · doi ↗ · pubmed ↗
- 5Complication rates of central venous catheters: a systematic review and meta-analysis JAMA Intern Med Teja B Bosch NA Diep C 47448218420243843697610.1001/jamainternmed.2023.8232 PMC 12285596 · doi ↗ · pubmed ↗
- 6Risk factors of catheter-associated bloodstream infection: systematic review and meta-analysis P Lo S One Lafuente Cabrero E Terradas Robledo R Civit Cuñado A 018202310.1371/journal.pone.0282290 PMC 1003584036952393 · doi ↗ · pubmed ↗
- 7Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 update Infect Control Hosp Epidemiol Buetti N Marschall J Drees M 5535694320223543713310.1017/ice.2022.87PMC 9096710 · doi ↗ · pubmed ↗
- 8Heparin versus 0.9% sodium chloride locking for prevention of occlusion in central venous catheters in adults Cochrane Database Syst Rev López-Briz E Ruiz Garcia V Cabello JB Bort-MartíS Carbonell Sanchis R Burls A 07201810.1002/14651858.CD 008462.pub 3PMC 651329830058070 · doi ↗ · pubmed ↗