The needs of parents and their network to influence physical activity and motor development among children 0-to-4-years old: a mixed-methods study protocol
Mary-ann R. Wagijo, Teatske M. Altenburg, Annick Ledebt, Floor Bartels, Robert K. van der Kaap, Katja Bel, Sanne Voorwinden, Corina van Doodewaard, Dave H. H. van Kann, Jessica S. Gubbels, Marleen H. M. de Moor

TL;DR
This study explores how parents and their networks can support physical activity and motor development in young children through a mixed-methods approach.
Contribution
The study introduces a systemic approach to understanding parental needs and environmental factors influencing early childhood physical activity.
Findings
Parents' perceived needs, obstacles, and opportunities will be analyzed to inform intervention strategies.
Longitudinal data will reveal patterns in daily activities and environmental influences on motor development.
Qualitative insights will highlight the role of the family network in supporting physical activity.
Abstract
Promoting physical activity and motor development in early childhood is important for physical and mental health outcomes later in life. However, knowledge on how to influence physical activity and motor development in early life focusing on families and their context in daily life is currently lacking. This study therefore aims to take a systemic approach to investigate the support needs, obstacles and opportunities as perceived by parents and their network to influence physical activity and motor development of young children aged 0 to 4 years. This study employs a longitudinal design over a two-month period per family, with mixed methods data collection. Data are collected in 36 families with a child aged 0 to 4 years and a total of 72 network contacts (2 per family). The study is part of the larger Active System for an Active Start project. Extensive qualitative and quantitative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
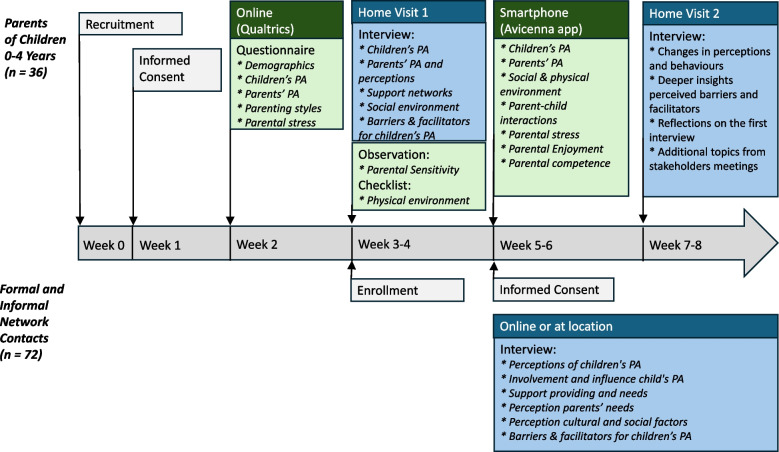 Figure 1
Figure 1- —https://doi.org/10.13039/501100001826ZonMw
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChildren's Physical and Motor Development · Green IT and Sustainability · Innovative Approaches in Technology and Social Development
Background
Early childhood represents a critical period for establishing healthy movement behaviours [1]. Physical activity (PA) in the early years (0 to 4 years) is associated with numerous health benefits, including improved motor skill development, cognitive development, healthy body weight, cardiometabolic, bone and skeletal health and psychological well-being [2–8]. Insufficient PA during early childhood contributes to delayed achievement of motor milestones [9–11], which can be difficult to catch up later in life [9–11].
However, already in infancy a large majority of children (0 to 1 years) do not meet the 24-hour movement guidelines as set by the World Health Organization (WHO)^7^, a trend which continues during toddlerhood and beyond [12–14]. The Dutch PA guidelines recommend for 0 to 1 year old children to be active multiple times a day, with at least 30 minutes of daily PA. For 1- to 4-year-old children the recommendation is to be active for at least 180 minutes per day, including bouts of moderate-to-vigorous PA. It is further recommended that children from both age groups are not ‘secured’ (e.g., strapped in a chair, car seat or bouncer) for longer than 60 minutes at a time, and that they do not sit still for long periods of time [15]. However, most children in the Netherlands between 0 to 4 years do not meet these guidelines [15], since they spend 76–85% of their wake time in sedentary behaviour and only 3–12% engaged in moderate-to-vigorous PA [16, 17].
Different studies and reviews have associated a variety of parental, family system and environmental factors with PA and motor development in children aged 0 to 4 year olds [8, 13, 18–25], which aligns with socio-ecological models of PA [26]. For both PA and motor development, child gender, parental age, family socioeconomic status, education of the parents and family composition have been identified as relevant determinants [25, 27, 28]. Boys seem to be more active compared to girls, having older parents is negatively associated with PA levels and a higher socio-economic status, high education, presence of both parents and having sibling(s) are positively associated with higher PA levels and motor development [21–23, 25, 27, 28].
Parents have great impact on fostering PA and motor development in children from 0 to 4 years old [18, 19]. A quantitative literature review conducted by Hesketh et al. (2017), explored determinants of change in PA in children from 0 to 6 years old and found that maternal role modelling, for example maternal PA, is positively associated with changes in PA levels of children [13]. Parental PA levels have an impact on children's PA, as parents act as role models, positively or negatively influencing their child’s behaviour [19, 20, 22]. Also higher involvement, awareness and co-participation of parents in PA and motor development are associated with positive outcomes [19, 21, 22]. In a study analysing both maternal sports participation and perceived exercise benefits/barriers, only the perceived benefits and barriers were directly associated with children's fitness and motor coordination. Maternal sports participation showed no direct relationship [29]. Furthermore, parents’ perceptions on PA, (work) schedule, health status and preferences of their child are important factors influencing children’s PA and motor development as well [22, 30–32].
The physical and social environments of young children also play a role in their PA and motor development. Physical environmental factors that are positively associated with PA in the early years include the availability of open spaces, playground equipment, and a variety of portable play materials [24]. People within the social environment of the child, such as parents, siblings, and peers, may influence the PA levels and motor development of a child through interactions with the child [33]. In addition, different motor development aspects (for example fine versus gross motor skills) are favoured or impaired, depending on the social cultural context in which a child is raised [27].
Despite the identified determinants, there are still gaps in our knowledge regarding the PA and motor development of 0 to 4 years old children. Firstly, most studies, including intervention studies, are limited to the daycare setting [34, 35]. In the Netherlands, 29% of the children under the age of 4 years does not attend daycare centres [36]. Focusing primarily on the daycare setting limits the reach of children who do not attend daycare as well as of infants in their first months of life, before attending daycare [37]. The home environment of young children is an important setting, but few studies focussed on 0-to-4-year-olds at home. The few studies on home environments reveal an association between developmental stimulation, toys, organization, mother interaction and children nearby in the home environment with PA in infants [38, 39]. Secondly, research on the perception of parents on PA and their needs in daily life to effectively promote PA among 0-to-4-year-old children is still lacking. Research focussing on the context of parents and children is important to develop effective interventions to promote PA in daily life including their home environment. Thirdly, in the social environment of parents and children, different network contacts (such as professionals, e.g., the general practitioner or physiotherapist, and friends or family, e.g., grandparents) can significantly influence health-related behaviours [40–42]. Research on older children (3 to 14 years old) showed that grandparental influence appears to play a significant role in promoting PA [40]. However, similar studies have not yet been conducted among younger children, even though these network contacts are likely also involved in their development as well. Therefore, identifying the perception and needs of network contacts, can provide valuable information to design interventions to influence PA and motor development, while taking the complete context of parents and children into account. In addition, little is known about the view of male caretakers, as they participate less in scientific studies directed at PA-related upbringing of children [20, 43].
This study takes a systemic approach to examine how parents and their informal and formal family networks perceive and support physical activity and motor development in children aged 0 to 4. Specifically, the study aims to address the following research questions:
- What are the support needs of parents regarding the PA and motor development of their children aged 0 to 4 years and what obstacles and opportunities do they experience in relation to themselves, their child, and the social and physical environment of the family?
- What daily activities do parents engage in to influence PA and motor development in their young children?
- How do members of the families’ formal and informal networks perceive the support needs of parents in promoting PA and motor development in young children, and what obstacles and opportunities do they encounter to promote PA and to support parents and children?
Methods
Study design
This study employs a longitudinal design over a two-month period per family, with a mixed methods data collection (see Fig. 1 for an overview of the different research methods and timeline). It is part of the Active System for an Active Start (ASAS) consortium that started in April 2024 and lasts until August 2027. This consortium is a multidisciplinary collaboration between different universities, universities of applied sciences, institutes of secondary vocational education and health-related organizations. The aim is to investigate how PA and motor development among 0-to-4-year-olds can be influenced by employing a systems approach. Data collection of this specific study takes place between September 2024 and November 2025 in three regions geographically spread over the Netherlands: West, North-East and South-East. Ethical approval was granted by the Ethics Committee of Erasmus University Rotterdam (Application number: ETH2324-0902).Fig.1overview of the different research methods and timeline of the study
Participants
The study aims to include 36 families (12 families per region) and 72 network contacts (two per family: one contact from their informal network such as a grandparent and one from their formal network such as a daycare professional). To ensure diversity in socioeconomic status of the families, parental gender, ethnicity and achieved motor milestones of the child (walking independently vs. not walking independently), various recruitment strategies were applied. To enhance such a variety in background characteristics, mid-study recruitment evaluations are conducted. Eligibility criteria for parents are: providing care at least 50% of the time for a 0-to-4-year-old child that is born >34 weeks with a birth weight >2500 gram and being proficient in spoken and written Dutch. Eligibility criteria for the network contacts are proficiency in spoken Dutch. Parents can receive a total financial compensation of €45, which they receive stepwise to enhance retention of the parents during the study [44, 45]. Network contacts do not receive financial compensation.
Recruitment
Recruitment takes place between September 2024 and July 2025 using multiple strategies. In each region, researchers from three universities of applied sciences recruit 12 parents. In the West region, two researchers are involved, in the North-East region three researchers, and in the South-East region also three researchers. A post-doc researcher monitors the overall data collection of the study. Parents will be recruited through social media and local organizations, for example: youth healthcare, community centres, swim schools, playgrounds, and daycare centres. Whenever possible, the researcher will ask employees at these organizations who are already in contact with parents, if they can attend meetings or gatherings to recruit parents in person. When recruiting in person, parents receive an information flyer and verbal information from the researcher. If they are interested in participation, their email address is registered to send them an elaborate information letter as soon as possible. With consent of the parents, their phone number is also registered to enable contact follow-up. If potentially interested parents do not contact the researcher themselves within a week after receiving verbal and/or written information, the researcher will contact them to ask if they are willing to participate or not. If employees from the organizations know parents who are eligible, they can contact the researcher by email or phone to provide the parents’ email address and telephone number (with the parents’ consent to do so). In addition, a digital flyer is posted online on social media (LinkedIn, Instagram and Facebook) and is will be send to the above-mentioned local organizations, with the request to add it in a digital newsletter or other communications with parents. Furthermore, a recruitment poster is designed to hang at local organizations. The digital flyers and posters contain a QR code that parents can scan to register themselves and the researcher will contact them afterwards. To increase trust between parents and researchers, the researcher who collects the parent’s data will be the contact person during the whole process unless this is impossible for practical reasons.
At the end of the first home visit, parents will be asked to identify individuals in their formal networks (e.g., daycare staff, physiotherapists, general practitioners, municipal health employees) and informal networks (e.g., family, friends, neighbours) who are involved in their child’s PA and motor development; examples of networks are provided if needed. One individual form the formal network and one from the informal network will be contacted by the researchers for an interview online or at a location of their choice. Network contacts receive an information letter by email and are contacted after one week to ask if they consent to participate. They will be asked to provide a written informed consent either through email or in person at the start of the interview.
Data collection procedures
After agreeing to participate, one regional researcher schedules a first home visit with the parent. Parents receive an email confirmation and an online link to a general questionnaire, which they are requested to complete before home visit 1. Home visit 1 includes an interview, a 15-minute observation of parenting behaviour during interaction with their child, a checklist about the physical environment and support to install the Avicenna app on parents’ smartphones for the brief momentary assessments using the Experience Sampling Method (ESM). ESM data collection starts after home visit 1and continues for 14 days. If for any reason, it is not possible to conduct the observation during home visit 1, the observation will take place during home visit 2.
Studies suggest that people’s attitudes and behaviours can shift over time as they reflect on experiences or face new situations and the process of reflection can be more accurately captured with adequate time between data points [46]. Therefore, we chose to schedule the second home visit with the parents after approximately two months. This time frame enhances the chances of capturing both short-term and long-term behavioural or situational changes, increasing the robustness of the data collected, and obtaining a more balanced and complete view of the parents’ experiences and attitudes over time. In addition, the time between the interviews provides the opportunity to identify topics that need to be addressed during home visit 2, based on home visit 1, the network interviews and input gathered from meetings with stakeholders that are part of the broader ASAS study.
Measurement instruments
Questionnaire
The questionnaire (see Table 1 and Supplementary Information) consists of closed-ended questions and optional open-ended responses, collecting the following demographic information: parental gender, age, marital status, ethnicity, education, and employment; household composition (e.g., questions about partner and other children); and child’s age and gender. Collecting demographic data enables researchers to assess and monitor diversity in the sample and allows subgroup analyses [53]. If the participating parent or their partner is not the biological parent of the child, additional questions about the ethnic background of the biological parent are asked. For all other questions about the partner, they refer to the partner they form a household with.Table 1. Overview of study outcomes collected in the questionnaires of the studyGeneral QuestionnaireESM QuestionnaireStudy ConstructMeasurement InstrumentStudy Construct****Measurement InstrumentBackground CharacteristicsGender parentSelf-developed (1 item)Age parentSelf-developed (1 item)Country of birth parent and their biological parentsSelf-developed (3 items)Family compositionSelf-developed (5 items)Education parent and partnerSelf-developed (2 items)Household income & workSelf-developed (3 items)Age childSelf-developed (1 item)Sex childSelf-developed (1 item)Child VariablesPhysical Activity & Screen timeMovement Behavior Questionnaire- Baby (12 items) or Movement Behavior Questionnaire -Child (18 items) [47]Momentary Activities1 item – Adapted from Dunton 2012 [48]Organized sport activitiesSelf-developed (1 item)Daycare during the weekSelf-developed (1 item)Parent VariablesPhysical ActivityInternational Physical Activity Questionnaire-Short Form (7 items) [49]Momentary Involvement of parent in activitySelf-developed (1 item)Parenting Styles (Authoritative, Authoritarian & Permissive)Parenting styles & dimensions questionnaireShort Version (32 items) [50]Momentary Feelings of Enjoyment while involved in activity with childSelf-developed (1 item)Parenting StressNijmeegse Ouderlijke Stress Index Short Form (Dutch Short version of the Parenting Stress Index) (33 Items) [51]Momentary Perceived Parental Stress while involved in activity with child1 item – Adapted from ESM repositoryMomentary Feelings of Competence while involved in activity with child4 items – Adapted from de Moor et al. 2023 [52]Physical EnvironmentMomentary physical location3 items - Adapted from Hager 2017 [39]Social EnvironmentMomentary presence of other people1 item – Adapted from Hager 2017^39^See Supplementary Information for exact phrasing of all question(s) and answer options
Additional sections of the questionnaire assess the children’s participation in organized sports and daycare arrangements, movement behaviours using the validated Movement Behaviour Questionnaire (MBQ-B for children who cannot yet walk, MBQ-C for children who can walk) [47], and parental PA via an instrument developed by the Flemish Institute Healthy Living questionnaire (the Vlaams Instituut voor Gezondheidsbevordering en Ziektepreventie (VIGEZ)), based on the short version of the IPAQ [49]. Parenting styles are assessed using the Parenting Styles and Dimensions Questionnaire [50], and parenting stress using the abbreviated Dutch version of the Parenting Stress Index (the Nijmeegse Ouderlijke Stress Index (NOSI)) [51, 54].
Home visit 1
The first home visit includes a semi-structured interview, a checklist of the physical environment and an observation of parenting behaviour during interaction with their child and lasts approximately 1–1.5 hours in total (see Table 2 and Supplementary Information). The interview starts with journey mapping their week planning and further covers the following topics: parental perceptions of children's PA and activities, their own past and current PA levels, their social and physical environment, and barriers and facilitators of promoting their children’s PA. These topics are based on socio-ecological models of PA and previous empirical research, emphasizing the influence of individual, social, and environmental factors on behaviour [22, 26]. Three pilot home visits were conducted before recruitment (without parent-child observation, because the researchers were still in training for this). Based on these pilot visits, question phrasing was refined and additional topics were included in the interview protocol, such as sibling influence and financial considerations for organized PA.Table 2. Overview of Study Topics Collected in the Interviews of the StudyHome Interview 1 ParentHome Interview 2 ParentInterview Formal Network****Interview Informal NetworkChild (Physical) ActivitiesOrganized activitiesAvailability toys for childRole in PA of childRole in PA of childPhysical activities the child likesJourney map (Visited places)Toys and activities directed at stimulating PA childParent Physical ActivityParents’ PA in childhoodCurrent parents’ PAPerceptionsPerception parent on character childScreen time childPerception physical activity young childrenPerception physical activity young childrenThoughts about PA childrenPerception own involvement PA childPerception own involvement PA childImportance PA childrenImportance PA childrenImportance PA childrenActivities the child is not able to do yet, but the parents would like them to doInfluence own upbringing and culture on PA childInfluence own upbringing and culture on PA childInfluence own upbringing and culture on PA childConcerns of parents about PA childrenConcerns of parents about PA childrenDescription of own role in stimulating PA of their childChallenges and BarriersConcerns about PA or motor development childContact with professionalsProviding support generalProviding support generalSupport in their environmentSources of information about PA and motor developmentProviding support PAProviding support PAImpact professional and private life on stimulating PA childSupport family, friends and partnerNeeds of parents to stimulate PANeeds of parents to stimulate PAOwn needs to stimulate PA childrenOwn needs to stimulate PA childrenPhysical EnvironmentJourney map (weekly activities)Safety neighbourhoodCharacteristics residence and surroundingSocial EnvironmentPeople involved in physical activities of the childPeople involved in physical activities of the childPeople involved in physical activities of the childImpact of siblings on PA of childPerception of partner on PA of childOtherFinancial contribution for PA childWork related activities involving PA children.Tips and tricks for parentsTips and tricks for parents
The researcher completes a physical environment checklist (see supplementary info 2. Home visit protocol 1 – Parents Guardians) assessing features of the home and neighbourhood environment related to PA and motor development, such as play equipment and outdoor space. Evaluating the home and neighbourhood environment is essential as research suggests that indoor and outdoor play spaces significantly impact children's movement behaviours [55–57].
To assess parenting behaviour in interaction with their child, we employed the OK! [58], which is a structured method to assess parental sensitivity efficiently in real-time in parent-child observations. Parental sensitivity is a construct that stems from attachment theory [59, 60] and is defined as the extent to which a parent correctly interprets and adequately and promptly responds to a child’s signals [61]. Previous research suggests that parental sensitivity is related to the development of young children’s explorative and play behaviours [62]). Researchers complete the OK! App e-learning [58] before the start of data collection to ensure consistent and reliable scoring. The e-learning training includes a user’s self-administered reliability test. In case reliability is insufficient, a second test is taken. If the second test is failed, further use of the OK! app is proscribed, and the researcher would be assigned other tasks. Researchers evaluate parental sensitivity based on predefined criteria in the app yielding a score ranging between 1 (Very strongly insensitive parental behaviour) and 7 (Very strongly sensitive parental behaviour). The observation lasts 15 minutes and utilizes age-appropriate boxes with toys to standardize play interactions. Studies using the OK! observation method have established that a 15-minute timeframe is sufficient for capturing parental sensitivity reliably [58].
Experience Sampling Method (ESM)
Daily physical activities of parents and their young children are assessed using ESM via the Avicenna app installed on the phones of parents. ESM is a valid method for studying daily and momentary fluctuations in behaviours, feelings, cognitions, interactions and environments [63, 64]. Parents receive four notifications per day over 14 days to complete very brief questionnaires of 10 items each (approximately 1-2 minutes to complete per notification). The notifications are sent out randomly within four fixed time frames during the day: between 8 and 11 AM, between 11 AM and 2 PM, between 2 and 5 PM and between 5 and 8 PM. Parents are asked to complete the questionnaires within an hour after the notification. Questions address current physical activities, social and physical environments (adapted from Hager et al. and Dunton et al. [39, 48]), parent-child interactions, parental stress, parental enjoyment, and parental competence while interacting with the child (adapted from de Moor 2023 et al. [52]) (see Table 1 and Supplementary Information). The researchers follow up on adherence by checking response rates in the Avicenna Research portal and contact the parents if responses are not received after two days. They remind the parents about the Avicenna app and ask if they need any assistance. A pilot ESM study with eight parents conducted in Spring 2024 (unpublished results) confirmed its feasibility and acceptability. Based on feedback about the answering options and clarity of questions, from the parents through interviews after the pilot, a few items in the ESM survey were adjusted, for example phrased in a different way or an option added in the answers, and the questionnaire was finalized.
Informal and formal network interviews
The interviews with parents' formal and informal network contacts (1 each per family) take approximately 45–60 minutes. The interviews are semi-structured and cover the family networks’ perceptions of children's PA and motor development, their involvement and influence regarding PA and motor development of the children, their perception on the influence of PA while they were growing up, their provision of support to parents, the cultural and social impact on PA of children, their perception on support needed by parents, and of barriers and facilitators to influence children’s PA and motor development themselves and through parents.
Home visit 2
Approximately two months after home visit 1, a second home visit is scheduled with the parents that lasts approximately 45-60 minutes. This home visit includes a second semi-structured interview that aims to explore possible changes in parental perceptions and behaviours, gain deeper insights into the perceived obstacles and opportunities mentioned by parents in the first interview, and assess reflections on the first interview. To this end, the researcher conducting the interview prepares by reading through and reflecting on the transcript from the first interview before the second interview. Furthermore, new topics are added based on the meetings with stakeholders as part of the broader ASAS study, including trust in PA and health professionals, perception on screen time behaviour, needs for support and equipment availability.
Data processing and analyses
Processing and analyses of interview data
All interviews are transcribed automatically with Amberscript. All generated transcripts are checked manually by the researchers for errors and corrected if needed, to transcribe the interviews at verbatim. After transcription, the interviews will be thematically coded in Atlas.ti [65], using collaborative coding [66]. In each region, one or two researchers will be assigned with the task of coding and participate in a weekly coding meeting where results of the coding process are discussed and aligned over the different regions. In brief, coding will be conducted in three steps: open, axial and selective coding. The identified themes based on the coding will reflect the support needs, obstacles and opportunities of parents and their network to influence PA and motor development of their 0-to-4-year-old children. Twenty percent of the interviews will be independently coded by two other researchers who will not participate in data collection (MRW and FB) and the codebook will be checked by two ASAS consortium members (TMA and JSG). Inter-rater reliability will be computed to assess consistency across coders. Thereafter, the remaining interviews will be double checked on a sample basis. Finally, the interviews will be analyzed with the framework method to identify important patterns, themes and associations [67, 68].
To answer the first research question, about the experienced needs, obstacles and opportunities of parents regarding the PA and motor development of their children aged 0–4 years in relation to themselves, their child, and the social and physical environment of the family, we will examine the interview data of the parents. Themes occurring from the interview data will be thematically presented together with quotes from specific parents to illustrate the themes.
To examine the third research question, about how the families’ formal and informal networks perceive the needs of parents in promoting PA and motor development in young children, and what obstacles and opportunities they encounter, interview data from the network contacts will be analysed and presented using the same procedures as described for the interview data of the parents.
Processing quantitative data
Survey data will be downloaded from Qualtrics and ESM data from Avicenna and saved in SPSS format. Observation data will be manually entered into SPSS. Next, these data will be checked for missings and errors (e.g., implausible values for age) and imputed or corrected where appropriate. Summed scores will be computed for questionnaires where appropriate. Last, all quantitative data derived from the interviews, survey, ESM and observations will be merged into one file in SPSS. For all analysis IBM SPSS Statistics, version 28.0 will be used.
Analyses of quantitative data
Descriptive analyses will be conducted to examine the distributions of the study variables (means, standard deviations, range, tests of normality for continuous variables, and frequencies for categorical variables) and the associations among study variables (by computing Pearson correlations and conducting t-tests, analysis of variance and chi-square tests depending on the measurement levels of the relevant variables) in the total study population. Furthermore, we will explore differences in distributions and associations by subgroups (i.e., region, gender parent, socio-economic status, age and motor milestones children).
The second research question, about the daily activities that parents engage in with their young children to promote their PA and motor development, will be answered by analysing the ESM data in combination with survey and observation data. Multilevel regression modelling and/or dynamic structural equation modelling will be employed to examine the interrelationships between PA of the children, parental stress, cognitions and emotions, and parent-child interactions across time and as a function of the social and environmental environment they find themselves in from moment to moment and from day to day [69–71].
Discussion
This study aims to provide a comprehensive understanding of the perceived support needs, obstacles and opportunities of parents and their network contacts to influence of PA and motor development in young children using a systemic approach.
This study has several strengths. First, the study employs a systematic approach focussing on parents, the family system and their social and physical environment and includes not only the perspective of parents but also that of two important persons from their formal and informal network. Second, the study employs a mixed-methods approach combining various types of qualitative and quantitative data. While the sample size is relatively small for a quantitative study with 36 parents and 72 network contacts and a larger sample could enhance generalizability, the in-depth data acquired by integrating multiple data collection methods (interviews, questionnaires, observations and ESM and network interviews) necessitates a more focused participant sample to ensure feasibility. In addition, the methodological triangulation —where key interview topics overlap with constructs assessed via observations, ESM and/or a questionnaire— enhances the validity and reliability of the findings. Third, the study leverages established collaborations with community partners who maintain direct contact with the populations of interest, facilitating translating research findings into practice.
Despite its strengths, the study also comes with some limitations. Selection bias poses a potential risk due to the intensive nature of the study and the various aspects of the data collection process. Some individuals may refrain from participating, because they might consider the research as time consuming. As a result, participating parents may be more intrinsically motivated and particularly interested in the topic. This self-selection could lead to a less heterogenous study population. However, despite intensive data collection the burden on parents is minimized as much as possible. This is achieved by, for example, combining different methods within a single home visit, eliminating travel time, and scheduling visits at a time convenient for the parent. In addition, researchers conduct observations instead of asking parents to self-report, whenever possible. The use of ESM also allows for brief, in-the-moment data collection, which is perceived as less demanding than other more intensive data collection methods such as keeping diaries [64, 70]. Furthermore, financial reimbursement is offered to increase participation rates. To increase the heterogeneity of the population, participants with various demographic backgrounds are recruited actively in addition to solely passive recruitment methods, such as online calls for participation and flyers. Recruiting participants from lower socio-economic backgrounds, ethnic minorities, and male caregivers remains a known challenge [43, 72]. Recruitment efforts emphasize face-to-face engagement, with follow-up occurring shortly after initial contact to maintain participant’s interest. Scheduling of the first interview at short notice is prioritized to minimize dropout.
Due to data collection by multiple researchers collecting data, the study has a risk of interview bias. This was reduced by discussing and reviewing the interview protocols with all the researchers before data collection, pilot testing in every region with presence of the postdoc researcher in every region and weekly meetings to discuss the interviews and possible obstacles. Response bias is inherent to the study’s data collection methods and is addressed through using different question formats and neutral language.
The combined results of this study will generate in-depth insights into the needs of parents and their network to support physical activity and motor development of their young children. Ultimately, the results of this study are expected to yield important insights that will guide the development and implementation of intervention strategies. The final aim, which will be part of activities of the broader ASAS consortium, is to successfully build communities of practice in the Netherlands to anchor these research findings in practice to effectively support parents and their social network to stimulate PA and motor development among their 0-4 years old child(ren) in daily life.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wijtzes AI, Kooijman MN, Kiefte-de Jong JC, de Vries SI, Henrichs J, Jansen W, et al. Correlates of physical activity in 2-year-old toddlers: the generation R study. J Pediatr. 2013;163(3):791-9.e 1-2.10.1016/j.jpeds.2013.02.02923523279 · doi ↗ · pubmed ↗
- 2Milieu Rv Ve. Erkende interventies - Bewegen en sport - 0-4 jarigen [Available from: https://www.loketgezondleven.nl/interventies-zoeken-overzicht?atabase=ey Jz Z Wxl Y 3Rl ZF 9ma Wx 0ZX Jz Ijpbey I 5Yzhi Nj Jl Yy 0y OTE 2LTQ 2ZD Ut YWY 5Yy 1h N 2Jj Nz E 4NTI 2ZT Mi Olt 7In Zhb H Vl Ijoi OW Jj Mj A 0ZW Ut YW Uz Zi 00NT Zj L Tkx N Tct M Tlj ZG My OT Jh Mm Mw In 1df Sx 7Ijlj OGI 2MWU 1L Tk 5OT Ut N Ddk My 05ZW Vh L Tg 5Mm Uy Zjg 3Nj A 3MCI 6W 3sib G Fi Z Wwi Oi JCYWJ 5J 3Ms IG Ry ZX Vt ZX Mg ZW 4gc GV 1d G Vycy Ao MC 00I Gph YX Ip Iiwidm Fsd W Ui Oi I 5Ym E 2MDY 4NC 02Ym Rl LT Qw Nj Yt Ym Nk Ni 1m Nm Fh NG Jl Ym E 1NG Mif V 19XX 0=.
- 3CBS. Kinderopvang in Nederland 2024 [Available from: https://dashboards.cbs.nl/v 5/SZW_Kinderopvang/.