No-shows among children and adolescents in public oral health service: a retrospective register-based study from Finland
Shweta Goswami, Nora Hiivala, Inari Mensonen, Tuomo Maisala, Minna Kaila, Battsetseg Tseveenjav

TL;DR
This study analyzed dental appointment no-shows among children and adolescents in Finland's public oral health services from 2006 to 2020.
Contribution
The study reveals a decreasing trend in no-shows over 15 years and identifies a polarized group responsible for most missed appointments.
Findings
Dental no-shows decreased from 9.9% to 5.8% between 2006 and 2020.
Boys had more no-shows than girls, and adolescents had higher rates than children.
Only 5% of children and adolescents accounted for over 21% of all missed appointments.
Abstract
The aim of this study is to assess dental no-shows or missed scheduled dental appointments among children and adolescents in public oral health services in Helsinki, Finland, where under 18-year-olds receive subsidized oral health care. This retrospective register-based study focused under 18-year-olds in Helsinki who had dental no-shows, which was defined as any failure to arrive for a scheduled appointment without notifying, in the public oral health services from 2006 to 2020. The study utilized retrospectively collected data from the City of Helsinki’s electronic patient health information register systems, Effica (2006–2017) and Lifecare (2018–2020), which were in use during the respective periods. In the context of this study, children refer age group 0–9 years and adolescents 10–17 years. A total of 2,513,376 appointments were found from patient register; 92.6% (n = 2,326,878)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
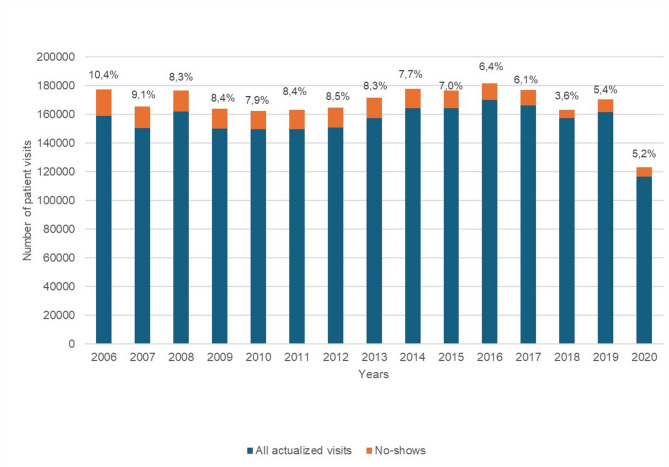 Figure 1
Figure 1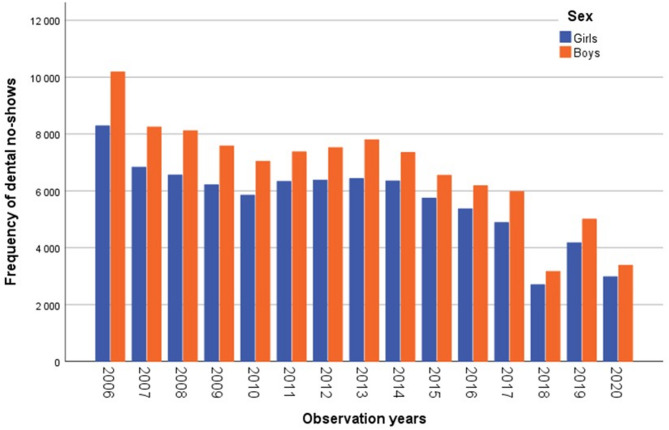 Figure 2
Figure 2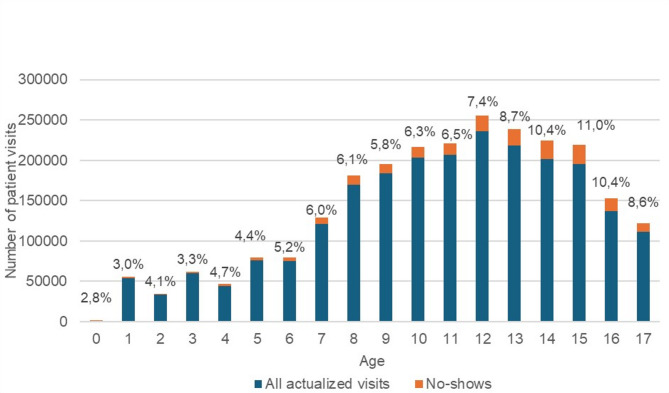 Figure 3
Figure 3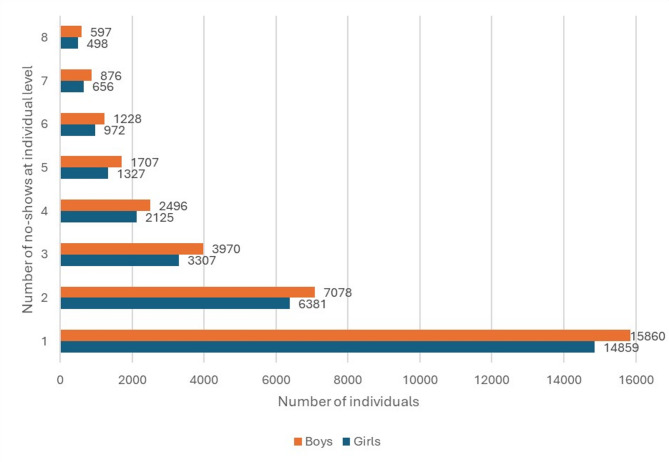 Figure 4
Figure 4- —University of Helsinki (including Helsinki University Central Hospital)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Anxiety and Anesthesia Techniques · Dental Research and COVID-19 · Dental Health and Care Utilization
Background
Oral health care services are crucial for sustaining oral health. When a patient does not attend a scheduled visit and does not cancel it, the visit is called a no-show [1]. In oral health care, no-shows can have detrimental effects such as elevated medical expenses, income loss, inefficient utilization of healthcare personnel, reduced productivity, disruption of patient care and impaired physician-patient rapport [2, 3]. Moreover, individuals who often miss their dental appointments are more likely to have untreated caries [4]. Regular dental visits enable prevention, and early detection and treatment of dental health issues [5]. A recent study from Finland showed that children from families on long-term social assistance had more no-shows and caries lesions than others [6].
Dental avoidance leads to poor oral health and later increased utilization of public oral health services [7–10]. A Swedish study of 16–19-year-olds indicated that 13.1% of 23,522 booked dental appointments were missed. Those skipping the visit had more oral health issues, required more invasive treatments, and had previously missed and cancelled dental appointments [11].
In Finland, children and adolescents have received free public oral health services, including orthodontics since 1972 [12]. Currently, around 47% of this population avail routine check-ups with a dentist or dental hygienist in the public oral health services [13]. The periodicity of oral health check-ups and examinations is dictated by Finnish Government Decree (338/2011) [14]. The Decree states that local authorities must provide at least once an examination of oral health status and need of treatment for each family expecting their first child, and an oral health examination for each child at the ages of one to two, three to four, and five to six years, carried out by dental hygienists or nurses, when needed by dentists. Likewise, schoolchildren in the 1 st, 5th and 8th grades must be examined. Specialist oral health examinations should be conducted as necessary. At the age of 17, youth receive an invitation to book dental appointments with dental hygienists. Children and adolescents at risk of oral diseases are provided with enhanced preventive oral health care [14].
The oral health of Finnish children and adolescents has improved since the 1970 s [15]. Between 2001 and 2013, approximately 40,000 children and adolescents visited the Finnish public oral health services annually, receiving a total of 2,488,805 treatment measures. However, the overall number of treatment measures has increased in the public oral health services [16]. Another study found that a significant proportion of low dental care user children and adolescents and orthodontic heavy users were caries free, while a small number in the heavy user group exhibited a significant number of caries [17].
Despite the free of charge provision of oral health services, it is not uncommon for dental appointments to be missed or cancelled among children and adolescents. It is therefore important to evaluate the rate at which dental appointments are missed in order to avoid potential negative outcomes in the future. The objective of this study was to assess the prevalence of dental no-shows among children and adolescents under 18 years of age and describe no-show trends between 2006 and 2020.
Methods
Study design and setting
This retrospective register-based study was based on electronic health information systems, Effica (2006–2017) and Lifecare (2018–2020), which encompasses dental care information of all the patients treated in the public oral healthcare department of City of Helsinki. Dental appointments for children and adolescents under 18-year-olds, are booked by public health centres for check-up examinations and treatment visits as well. All these visits are registered in the health information system, also in case the individual misses the appointment without cancelling. An automatic phone message service (SMS) reminder system was introduced in 2007 to prevent no-shows.
Data extraction
In this study, a no-show refers to missing scheduled appointment without cancelling, i.e. cancellation with pre-notification was not considered a no-show. The scheduled visits were categorized into two according to treatment codes made by dentists, dental hygienists or dental nurses. The scheduled appointments were then recoded based on later events into (1) actualized visit: if any examination or treatment code was identifiable in the records, and (2) no-show (missed appointment): if the code was 900, specific and official code for missed appointment. In this study, children referred 0–9-years-olds and adolescents 10–17-years-olds, respectively. These codes are provided by the Finnish National Institute for Health and Welfare.
Statistics
The statistical analyses were carried out using the SPSS 28.0 software (SPSS Inc., Chicago, IL, USA). Descriptive statistics were reported. Correlations between variables individual’s age and sex, observation years of the study and frequency of no-shows were calculated using Pearson’s correlation test (r). The data analyzed was then graphed using Microsoft Excel 365.
Results
The periodicity and oral health examinations in Helsinki, according to public information provided by the City of Helsinki in 2024 [18], are depicted in Table 1. Expecting family or first-time parents as well as all age groups of children and adolescents shown in Table 1 receive invitation letters for booking their oral health examination.Table 1.Periodicity and oral health check-ups in Helsinki, FinlandOral health check-ups carried out byExpecting Family or First Time ParentsDental Nurse or Remote Appointments1-year-oldsDental Nurse or Remote Appointments3-year-oldsDental Nurse5-year-oldsDental Nurse or Dental Hygienist 1 st grade schoolchildren(about 7-year-olds)Dental Hygienist3rd grade schoolchildren(about 9-year-olds)Dentist5th grade schoolchildren(about 11-year-olds)Dental Hygienist8th grade schoolchildren(about 14-year-olds)Dentist17-year-oldsDental Hygienist
A total of 2,513,376 dental appointments were scheduled for patients aged 0–17 years from 2006 to 2020 (Fig. 1). Of these, 92.6% (n = 2,326,878) were actualized visits and 7.4% (n = 186,498) were no-shows.
Fig. 1. Dental actualized visits and no-shows among children and adolescents in Helsinki health centers, by years from 2006–2020
The frequency of dental no-shows declined among boys and girls from 2006 to 2020. There was total 186,497 no-shows – 85,054 among girls and 101,443 among boys. The boys accounted for 54.4% of all no-shows and surpassed the number of no-shows among girls each year. The no-shows increased between 2011 and 2013 (girls: 6,329 to 6,430; boys: 7,370 to 7,796), followed by a steady decline up to 2017. In 2020, the frequency of no-shows decreased by 64% among girls and 67% among boys compared to 2006. A significant sex difference (p = 0.002) in no-show rates was observed within the study period. Figure 2 shows frequency of dental no-shows by sex.
Fig. 2. Frequency of dental no-shows by individuals’ sex and observation years in Helsinki health centers from 2006–2020
The prevalence of no-shows was 5.2% and 8.6% among children and adolescents respectively. The non-utilization of dental health care has shown an upward trend from childhood through adolescence. The number of no-shows peaked at 14–15 years of age, where no-shows accounted for 10.7% and 11.0%, respectively (Fig. 3).
Fig. 3. Dental actualized visits and no-shows among children and adolescents in Helsinki health centers, by their age during 2006–2020 (n = 2,513,376).1
A positive correlation was found between age and the frequency of no-shows (r = 0.872, p < 0.001). However, an inverse association was seen between the number of years and frequency of no-shows (r = −0.884, p < 0.001). Among those with one or more no-shows, 53% were boys and 47% girls.
All no-shows (186,498) between 2006 and 2020 belonged to 67,284 children and adolescents. Of all, 45.7% (n = 30,719) of the children and adolescents had one missed appointment and 49.3% (n = 33,218) had two to eight missed appointments, accounting for 115,087 of the total no-shows. Fig. 4 shows children and adolescents (n = 63,037) with 1 to 8 no-shows; cumulative frequencies accounting 95% of all no-shows. In each scale group (Fig. 4), no-shows differed by sex (p > 0.05). Of all children and adolescents, 5% (n = 3,347) had 9 to 40 no-shows, which accounted 21.8% (n = 40,692) of all missed appointments, revealed a strong polarization of the phenomenon.
Fig. 4. Distribution of 1–8 dental no-shows among children and adolescents at individual level, separately by sex (n = 145,806), in Helsinki health centers during 2006–2020
Discussion
The findings of this study indicate that there is a significant positive and inverse correlation with age and observation years (p < 0.001) in the prevalence of dental no-shows among children and adolescents, emphasizing the credibility and robustness of these associations.
Dental no-shows were more frequent in adolescents and among boys than in children and among girls, respectively. The present decreasing trend from 2006 to 2020 differed from our previous study, which showed an increasing trend of no-shows among children and adolescents in specialized care from 2009 to 2023 [19]. This could be related to the centralization of dental general anesthesia patients in specialized care, increasing numbers of both actualized visits and no-shows [19]. According to the present and previous results [20], no-shows are more frequent among adolescents than among children.
Although free dental services are accessible among children and adolescents in Helsinki health centers, there is still a noticeable disparity in their utilization. Failing to attend scheduled visits may negatively impact the patient’s health as a result of the delay in diagnosis or treatment [1]. Of children who missed more than 10% of their dental appointments, 74% had untreated caries [4]. Missed dental appointments can lead to poorer oral health as well as exacerbated emergent dental needs [4, 21]. Children who miss their scheduled dental appointments should be classified as high-risk patients and provided with personalized treatment plans [9].
In this study, the prevalence of dental no-shows among children was 5.2%. According to a study, 15% of children who had missed at least one appointment in the previous two years had increased enamel disturbances, caries experience, and caries activity as well as longer treatment duration [9]. Children who had one or more missed dental appointments, had behavior management issues, dental anxiety, and parents who avoided dental care were more likely to have caries experience at the age of 5 years [22]. Previous research has documented the prevalence of missed dental appointments among the pediatric population ranging from 6.7% to 52% [23–27].
Among adolescents, the dental no-show rate was found to be 8.6% in this study. The findings of previous studies showed the prevalence of dental avoidance (irregular, delayed, cancelled, and no-show) has been estimated to reach 20% among adolescents in Scandinavia including Norway and Sweden where oral health care services are free of charge among children and adolescents [7, 11, 28]. Dental care during adolescence is crucial for multiple reasons, such as the emergence of permanent teeth, which leads to an increased risk of tooth decay on more surfaces, as well as a higher likelihood of early periodontal disease [29, 30]. Hence, adolescents are more susceptible to oral diseases during a crucial developmental stage while they are forming oral hygiene routines [31]. The prevalence of dental no-shows was found to be lower among individuals aged 16 and 17 compared to the uptrend pattern observed in 0–15 years old in this study. This could be attributed to the fact that the number of actualized visits was also lower among them. According to the information retrieved from the City of Helsinki, about 43% of 17-year-olds did not schedule an appointment despite receiving an invitation letter.
The results of the present study have found adolescents had a higher dental no-show rate than children. This finding is in accordance with previous studies [7, 32, 33]. By contrast, some studies report that dental no-shows tend to be higher in children than adolescents [20, 34]. This might be related to the different sociodemographic and other related characteristics [20, 34]. The disparity in the utilization of dental services is influenced by individual, social, cultural, and economic determinants [35].
A recent review has suggested various factors for non-utilization of dental services including predisposing (age, gender, ethnicity, parent’s level of education), enabling (family income, dental insurance) and treatment need factors (oral clinical status) [20]. Those belonging to racially and ethnically varied origins face a greater likelihood of having unmet dental health needs, as well as those with intricate medical conditions [36, 37]. Therefore, it is important to understand the specific patient characteristics that are connected with this behavior in order to establish focused intervention programmes [38]. The role of parents in children’s oral health is crucial. Parents can have a direct impact on the prevention of oral and other diseases of their children by teaching them healthy behaviors.
The declining trend of no-shows during the observation years of this study may partly reflect the effectiveness of various measures implemented by oral health care system to minimize the magnitude of missed appointment, such as sending SMS-reminder message to caretakers of children and to adolescents themselves.
This study also showed strong polarization identified as 5% of all children and adolescents had 21.8% of all missed appointments. This phenomenon of no-shows is also seen in the previous study of children and adolescents in specialized care [19], where almost 6% of them had nearly 19% of the no-shows. Identifying the factors of polarization may reveal why some children and adolescents missed more dental appointments than others and aid in the development of interventions to alleviate the burden of dental no-shows and associated adversities.
The significant association between dental anxiety and avoidance of dental visits is widely recognized [8, 11, 39]. Previously, dental anxiety, pain experiences, poor oral health status, and a family history of avoidance have been linked to avoidance of dental visits [28]. In the present study, the dental no-show prevalence in the age groups six, 12 and 15 were 5.2%, 7.4% and 11% respectively. . Previously, high dental fear has been reported among 12- and 15‐year‐old children as compared to the younger ones [40]. Caries-affected children between six and twelve years were more likely to report dental fear than their caries-free counterparts [40].
Missed dental appointments waste publicly funded capacity and may increase treatment costs when preventive care is not taken. No-shows disrupt patients, providers and clinical procedures that leads to further difficulty in scheduling appointments. The delay of preventive care and primary treatment may accelerate disease progression, leading to more complex and costly procedures [41].
Strength and limitation of the study
Since the data were collected from the public health sector, which provides dental services to all children and adolescents, the findings can be considered generalizable. In addition, this study for the first time explored no-shows among children and adolescents and identified the polarization of the no-show phenomenon. The present results should be applied by improved understanding of which patients are more likely to miss their appointments and the underlying reasons for their absences, in order to effectively help resolve individual barriers [42].
A limitation of this study is that the data originates from patient heath records, meaning any documentation errors remain uncorrected, as is common in register-based study. In this study, we did not relate numbers of no-shows with total dental visits or with emergency visits of the individuals.
Conclusion
The 15-year trend analysis showed a reduction in yearly dental no-show prevalence among children and adolescents, in general. However, there is a positive correlation between age and the frequency of no-shows. There was a strong polarization of the no-show phenomenon, only 5% of the children and adolescents accounting more than one fifth of all missed appointments. This polarized group needs to be characterized, so that potential underlying causes can be studied.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hiilamo A, Keski-Säntti M, Mannevaara M, Kallio J, Harjunmaa U, Koskenvuo K. Toimeentulotukea Saaneiden Perheiden Lapsilla on Ilmoittamattomia poisjääntejä hammashoidosta Ja Hammaskariesvaurioita Muita useammin – rekisteritutkimus Vuonna 1997 syntyneistä Espoolaisista. 2023. https://ideas.repec.org/p/osf/socarx/ktfw 9.html .
- 2Finnish Institute for Health and Welfare, Finland - THL. Suun ja hampaiden sairauksien hoidon laaturekisteri – tulosraportti. 2023. https://repo.thl.fi/sites/laaturekisterit/suun_terveyden_rekisteri/nqrodh.html#jump_leader 2 .
- 3Finlex. Government Decree 338. /2011. Maternity and child health clinic services, school and student health services and preventive oral health services for children and youth. 2011. https://www.finlex.fi/en/laki/kaannokset/2011/en 20110338.pdf .
- 4City of Helsinki. Health and social services. Dent Care. 2024. https://www.hel.fi/en/health-and-social-services/health-care/dental-care .