Invasive Group A Streptococcal Infection Following Nasal Self-Packing With Facial Tissue: A Case Report
Takeo Mori, Sadako Yoshizawa, Naoki Onda, Yamato Mifune, Fumio Sugo, Katsuhito Kashiwagi, Takahiro Sato, Tadashi Maeda, Norihiko Takemoto, Yosuke Sasaki

TL;DR
A man with multiple myeloma developed a severe streptococcal infection after self-packing his nose with facial tissue, leading to septic shock.
Contribution
Highlights how nasal self-packing can lead to invasive group A streptococcal infection in immunocompromised individuals.
Findings
Nasal self-packing with facial tissue preceded the onset of invasive group A streptococcal infection.
The infection led to septic shock requiring norepinephrine infusion in an immunocompromised patient.
The causative strain was identified as emm49 through emm typing.
Abstract
Invasive group A streptococcal infection (iGAS) can develop rapidly in immunocompromised individuals. We describe the case of a 66-year-old man with multiple myeloma who was admitted for chemotherapy and subsequently developed iGAS. He had been performing nasal self-packing with facial tissue for nasal discharge and hemorrhage. During hospitalization, he developed erythema, pain, and swelling around the nose and experienced a sudden onset of septic shock characterized by profound hypotension requiring norepinephrine infusion. Streptococcus pyogenes was detected in blood cultures, and treatment with beta-lactam antibiotics and clindamycin led to rapid improvement. Follow-up testing revealed that emm typing identified the strain as emm49. This case highlights that in immunocompromised individuals, trivial self-care like nasal self-packing can precipitate severe infections such as iGAS and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
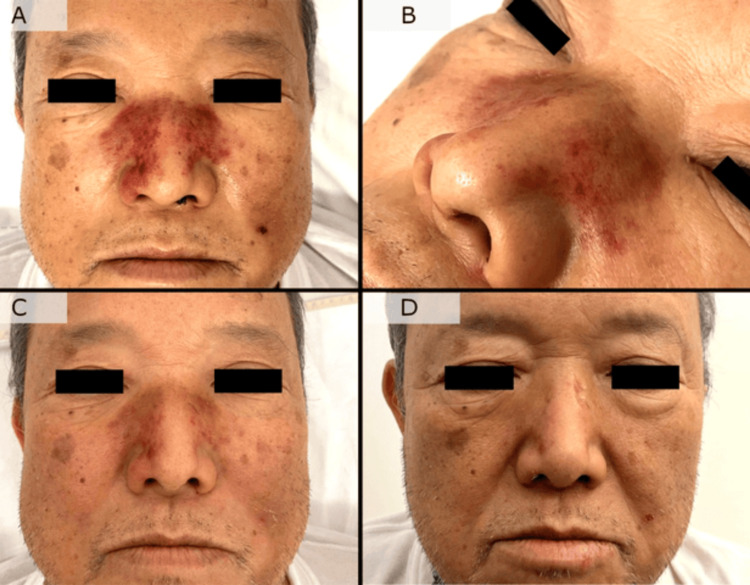 Figure 1
Figure 1| Laboratory parameter | Observed value | Reference range |
| WBC (/μL) | 3,200 | 3,300-8,600 |
| Basophil (%) | 0 | 0-2 |
| Eosinophil (%) | 0 | 1-9 |
| Lymphocyte (%) | 6 | 25-48 |
| Meta-myelocyte (%) | 1 | 0 |
| Segment cell (%) | 85 | 22-72 |
| Band cell (%) | 3 | 0-18 |
| Monocyte (%) | 5 | 2-12 |
| RBC (×104/μL) | 211 | 435-555 |
| Hb (g/dL) | 8.8 | 13.7-16.8 |
| Ht (%) | 25.9 | 40.7-50.1 |
| MCV (fL) | 122.7 | 83.6-98.2 |
| MCH (pg) | 41.7 | 27.5-33.2 |
| MCHC (%) | 34 | 31.7-35.3 |
| PLT (×104/μL) | 10.9 | 15.3-34.8 |
| Na (mEq/L) | 142 | 138-145 |
| K (mEq/L) | 3.6 | 3.6-4.8 |
| Cl (mEq/L) | 102 | 101-108 |
| UA (mg/dL) | 7.2 | 3.7-6.9 |
| UN (mg/dL) | 42 | 8-20 |
| Cr (mg/dL) | 1.86 | 0.65-1.07 |
| AST (IU/L) | 28 | 13-30 |
| ALT (IU/L) | 18 | 10-42 |
| LDH (IU/L) | 361 | 124-222 |
| γ-GTP (IU/L) | 52 | 13-64 |
| CK (IU/L) | 47 | 58-248 |
| Glucose (mg/dL) | 86 | 73-109 |
| HbA1c (%) | 5 | 4.9-6.0 |
| CRP (mg/dL) | 4.2 | 0.0-0.2 |
| PCT (ng/mL) | 301.56 | <0.05 |
| IgG (mg/dL) | 3,723 | 861-1,747 |
| IgA (mg/dL) | 12 | 93-393 |
| IgM (mg/dL) | <10 | 33-183 |
| PT (seconds) | 14.9 | 9.6-13.1 |
| PT-INR | 1.4 | 0.8-1.2 |
| PT% (%) | 58 | 70-130 |
| APTT (seconds) | 35.4 | 24.0-39.0 |
| Fibrinogen (mg/dL) | 364 | 200-400 |
| FDP (μg/mL) | 55.6 | <5 |
| D-dimer (μg/mL) | 34.1 | <1.0 |
| Laboratory parameter | Observed value | Reference range |
| Arterial blood gas analysis (nasal cannula at 2 L/minute O₂) | ||
| pH | 7.410 | 7.38-7.46 |
| PaO2 (mmHg) | 77.1 | 74-108 |
| PaCO2 (mmHg) | 31 | 32-46 |
| CHCO3- (mEq/L) | 19.3 | 22.5-26.9 |
| Lactate (mmol/L) | 1.5 | 0.5-1.6 |
| Urinalysis | ||
| pH | 5 | 4.5-7.5 |
| Protein | + | - |
| Sugar | - | - |
| Acetone | - | - |
| Nitrite | - | - |
| Sediment WBC (/HPF) | 5-9 | 0-4 |
| Sediment RBC (/HPF) | 10-19 | 0-4 |
| Antibiotics | MIC (μg/mL) |
| Penicillin G | ≦0.06 |
| Ampicillin | ≦0.25 |
| Sulbactam/ampicillin | ≦0.25 |
| Cefotiam | ≦0.5 |
| Ceftizoxime | ≦0.25 |
| Cefpirome | ≦0.5 |
| Cefditoren-pivoxil | ≦0.12 |
| Imipenem | ≦0.12 |
| Meropenem | ≦0.12 |
| Clarithromycin | ≦0.12 |
| Minocycline | ≦0.25 |
| Vancomycin | ≦0.5 |
| Teicoplanin | ≦0.5 |
| Tosufloxacin | ≦0.5 |
| Levofloxacin | 1 |
| Clindamycin | ≦0.12 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Otolaryngology and Infectious Diseases · Ear Surgery and Otitis Media
Introduction
Streptococcus pyogenes is a well-known causative pathogen of skin and soft tissue infections, such as erysipelas and cellulitis, and in some cases, it can lead to severe conditions, including necrotizing fasciitis and toxic shock syndrome (TSS) [1]. In particular, invasive group A streptococcal infections (iGAS) and streptococcal toxic shock syndrome (STSS), which are triggered by toxins produced by the bacterium, are known for their rapid progression and high mortality rates [1].
TSS has been reported to occur in women as a result of using menstrual products such as tampons [2]. Regardless of gender, there have been some reports of TSS caused by S. pyogenes and Staphylococcus aureus following nasal sinus surgery or nasal packing for epistaxis [3-5]. We report a case of iGAS in a patient with a history of multiple myeloma, who developed the infection after performing nasal self-packing with facial tissue for nasal discharge and hemorrhage. This case suggests that, particularly in immunocompromised patients, inserting facial tissue into the nasal cavity may serve as a potential risk factor for iGAS. We report this case to highlight important considerations for similar future cases.
Informed written consent was obtained from the patient for the open-access publication of this case report.
Case presentation
A 66-year-old male patient presented to our hospital with complaints of back pain. Two months prior to the onset of disease, he experienced movement-related back pain, nasal discharge, and hemorrhage. He had been performing nasal self-packing with facial tissue once a day. One month prior to onset, he was referred to our hospital for further evaluation of his back pain. He had a medical history of hypertension, dyslipidemia, gastroesophageal reflux disease, and idiopathic contact dermatitis. His regular medications included nifedipine, azilsartan, bisoprolol, vonoprazan, sodium picosulfate, and a combination tablet of tramadol and acetaminophen. He had a smoking history of two packs per day for 46 years, but no history of alcohol consumption or overseas travel.
Following his initial visit to our hospital, laboratory testing and computed tomography revealed anemia, protein-albumin dissociation, and multiple osteolytic lesions. Based on these findings, he was subsequently diagnosed with stage III multiple myeloma according to the Revised International Staging System, identified as IgG-producing type. He was admitted for treatment seven days prior to disease onset. Three days before onset, he received chemotherapy with bortezomib, lenalidomide, and dexamethasone. During this time, he also continued nasal self-packing with facial tissue.
On the day of onset, erythema with pain appeared around his nose, and a few hours later, he developed fever and shock. His vital signs were as follows: body temperature at 40.1°C, blood pressure at 68/47 mmHg, heart rate at 106 bpm, percutaneous oxygen saturation at 95% (room air), and respiratory rate at 24 breaths per minute, indicating shock and tachypnea. Physical examination revealed erythema and purpura with warmth, swelling, and tenderness over the nasal dorsum and alae (Figure 1). There were blood clots in the left nasal cavity. Bilateral tonsillar enlargement and erythema were observed, with white exudate on the left tonsil. No significant abnormalities were found in heart sounds, lung sounds, the abdomen, or the extremities.
Clinical course of nasal erythema and swellingOn the day of onset, physical examination revealed erythema and purpura with warmth, swelling, and tenderness over the nasal dorsum and alae (A). An enlarged view of the macroscopic photograph (B). On the second day after onset, the erythema and swelling persisted but showed slight improvement (C). On the fourth day after onset, local findings had disappeared (D)
Laboratory findings showed leukopenia, anemia, and thrombocytopenia, along with an elevated inflammatory response (C-reactive protein: 4.2 mg/dL). His renal function had deteriorated from 0.82 to 1.86 mg/dL the previous day. Procalcitonin was markedly elevated at 301.56 ng/mL. Immunoglobulin levels showed an increased IgG of 3,723 mg/dL, while IgA and IgM were suppressed. Other blood and urine test results are shown in Tables 1, 2. A chest X-ray showed pulmonary congestion and cardiac dilatation. Computed tomography revealed mucosal thickening and fluid retention in the maxillary and ethmoid sinuses and a fracture in the left nasal bone. Although differential diagnoses such as urinary tract infection, catheter-related bloodstream infection, and other causes of shock, including anaphylaxis, were considered, the combination of his clinical history and local nasal findings strongly suggested bacterial infection of the nasal cavity with septic shock. Blood cultures were performed, and treatment with meropenem and norepinephrine was initiated.
The next day, Gram-positive streptococci were detected in blood cultures. Matrix-assisted laser desorption/ionization (MALDI) time-of-flight mass spectrometry using MALDI Biotyper (Bruker Daltonics GmbH, Bremen, Germany) from the blood identified it as S. pyogenes. Because STSS was highly considered, clindamycin was added to the meropenem regimen. The treatment course was favorable, with local symptoms showing a tendency to resolve and become slightly less prominent by the second day of treatment, allowing discontinuation of norepinephrine. By the fourth day, local findings had disappeared (Figure 1).
The final identification of the bacteria was S. pyogenes, and the same pathogen was also isolated from the pharyngeal mucosa and the nasal cavity. emm gene analysis identified the strain harbors emm49. The results of antimicrobial susceptibility are shown in Table 3. Based on final identification and antimicrobial susceptibility results, the antibiotic regimen was changed to intravenous ampicillin and clindamycin. Once the patient recovered from shock and vital signs stabilized, administration of clindamycin was discontinued. The patient underwent 11 days of intravenous therapy and was discharged for personal reasons. Because of concerns about a relapse due to the short duration of therapy for bacteremia, he was given one week of oral amoxicillin. After a total of 18 days of treatment, there is no recurrence.
Discussion
Patients with multiple myeloma are known to have an increased risk of infections due to impaired production of normal immunoglobulins [6]. In particular, secretory IgA has a role in mucosal infection defense, and IgG3 is involved in the initial immune response to the M protein of S. pyogenes [7,8]. This risk is particularly high in advanced cases and during the early stages of diagnosis [9]. Previous reports suggested that the incidence of infectious diseases can be up to seven times higher in these patients [10]. In 2023, a case of toxic shock-like syndrome caused by Streptococcus agalactiae of unknown entry site was reported in a patient with treatment-resistant multiple myeloma [11]. As in previous reports, the present case was observed at both the initial diagnosis stage and an advanced disease state, suggesting a possible association. Although this case did not meet the criteria for STSS as defined by the Centers for Disease Control and Prevention, the patient presented with rapidly developing shock, along with vital signs, respiratory failure, renal impairment, and disseminated intravascular coagulation, suggesting a case very close to STSS.
As seen in this patient, long-term retention of foreign bodies in the nasal cavity can stimulate local bacterial growth. A previous study reported the detection of Klebsiella spp., Proteus mirabilis, S. aureus, Streptococcus pneumoniae, and Haemophilus influenzae from packing materials used after hemorrhage and sinus surgery [12,13]. Cases of infective endocarditis and spondylitis caused by S. aureus following nasal septum surgery have also been reported [14]. Additionally, cases of TSS caused by S. pyogenes and S. aureus have been reported after nasal or sinus surgery, suggesting that nasal packing may be a risk factor for TSS [3-5]. In the present case, it is presumed that the enclosed environment created by facial tissue in the nasal cavity facilitated the colonization and local proliferation of S. pyogenes. A previous study involving 350 healthy volunteers aged 18 years or older in Poland reported a pharyngeal carriage rate of S. pyogenes of 4.9%, highlighting that, even among healthy adults, asymptomatic colonization can occur [15].
The isolated S. pyogenes strain was identified as emm49. The emm gene encodes the M protein of S. pyogenes, which is an important virulence factor involved in cell adhesion, resistance to phagocytosis, and inhibition of complement system activation [16]. The emm49 strain has been increasingly reported in recent years in the United States, the United Kingdom, Canada, and Spain [17-19]. In an analysis of strains obtained from 526 STSS patients in Japan between 2019 and 2021, emm49 accounted for 8.4% of the total, making it the fourth most common type following emm1, emm89, and emm81 [20]. Its proportion increased from 3.4% in 2019 to 13.5% in 2022 [20]. It has also been shown that the emm49 strains carrying a mutation in the scpA gene, which encodes the C5a peptidase protein involved in promoting local infections such as skin and soft tissue infections, are spread in Arizona [21,22]. Also, in our case, inflammation of the skin and soft tissue around the nose was observed. While the M1UK strain has drawn attention in cases of severe S. pyogenes infections, considering epidemiological data, it is also important to recognize the potential threat of the emm49 strains [23].
This case highlights that the presence of a foreign body in the nasal cavity, such as facial tissue, particularly in immunocompromised patients, may serve as a trigger for severe bacteremia. Recognizing this risk emphasizes the importance of infection prevention education for immunocompromised patients. Additionally, with the increasing prevalence of highly virulent S. pyogenes strains, there is a concern that similar cases may become more frequent in the future.
Conclusions
This case represents a rare clinical course of iGAS in a patient with multiple myeloma, and nasal self-packing with facial tissue was considered a possible trigger. The presence of a foreign body in the nasal cavity may have facilitated local bacterial colonization and proliferation and led to systemic infection. The isolated S. pyogenes strain was identified as emm49, a genotype that has been increasing in prevalence in recent years and is suggested to be associated with pathogenicity. Beyond its rarity, this case highlights key lessons for clinical practice: even seemingly trivial self-care behaviors can carry serious risks in immunocompromised individuals, and clinicians should maintain vigilance for iGAS when unusual local findings are present. Awareness of these risks may help reduce the likelihood of similar severe infections in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Invasive group A streptococcal infections: lessons learned from the 2022-23 upsurge Lancet Infect Dis Flamant A Demirjian A Lamagni T 147330999202510.1016/S 1473-3099(25)00343-340651487 · doi ↗ · pubmed ↗
- 2Clinical and molecular epidemiology of Staphylococcal toxic shock syndrome in the United Kingdom Emerg Infect Dis Sharma H Smith D Turner CE 2582662420182935015910.3201/eid 2402.170606 PMC 5782905 · doi ↗ · pubmed ↗
- 3Streptococcal toxic shock syndrome (STSS) secondary to monoarticular septic arthritis leading to multiorgan failure in a patient without underlying comorbidities: emphasizing early diagnosis and management strategies. [Online ahead of print]Infect Disord Drug Targets Chady A Brandon C Michelle S Fahad O Asad O 202510.2174/011871526532674024121808031939886786 · doi ↗ · pubmed ↗
- 4Toxic shock syndrome following submucous resection and rhinoplasty JAMA Thomas SW Baird IM Frazier RD 240224032471982 https://jamanetwork.com/journals/jama/fullarticle/3721747069900 · pubmed ↗
- 5Phlegmonous gastritis and group A streptococcal toxic shock syndrome in a patient following functional endoscopic sinus surgery Surg Infect (Larchmt) Paik DC Larson JD Johnson SA Sahm K Shweiki E Fulda GJ 5455491120102057566610.1089/sur.2009.064 · doi ↗ · pubmed ↗
- 6Antibody deficiency in paraproteinemia Acta Med Scand Dammacco F Clausen J 7557681791966438027210.1111/j.0954-6820.1966.tb 05500.x · doi ↗ · pubmed ↗
- 7Physiology of Ig A and Ig A deficiency J Clin Immunol Cunningham-Rundles C 3033092120011172000310.1023/a:1012241117984 · doi ↗ · pubmed ↗
- 8Immunoglobulin G subclass concentrations and infections in children and adolescents with severe asthma Pediatr Allergy Immunol de Moraes Lui C Oliveira LC Diogo CL Kirschfink M Grumach AS 1952021320021214464210.1034/j.1399-3038.2002.00058.x · doi ↗ · pubmed ↗