Bedside Removal of a Retained Plastibell Ring Using Handheld Electrocautery in the Emergency Department
Benjamin H Press, Elizabeth Chu, Emily S Blum

TL;DR
A 15-day-old baby had a Plastibell ring removed using handheld electrocautery at the bedside when other methods failed, showing it could be a viable alternative.
Contribution
Introduces handheld electrocautery as a feasible alternative for removing a retained Plastibell ring in resource-limited settings.
Findings
The plastic ring was successfully melted and removed using electrocautery without sedation or injury.
Post-removal examination showed normal perfusion and no urethral damage.
Follow-up at five months showed normal healing and cosmesis.
Abstract
We report a 15-day-old infant with a proximally migrated Plastibell and marked glans edema. Ligature release with gentle manipulation was unsuccessful; scissor division was judged unsafe, and a ring cutter was unavailable. A handheld, battery-powered fine-tip cautery was used at the bedside to melt and divide the plastic ring with tissue protection and local analgesia, permitting removal without sedation. Postremoval examination showed preserved perfusion without urethral injury, and five-month follow-up demonstrated normal healing and cosmesis. This case suggests that handheld cautery may be a feasible and resource-conscious alternative when mechanical methods are unsuitable or unavailable. Careful patient selection and thermal safety measures are essential, and further experience is needed to define their role.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2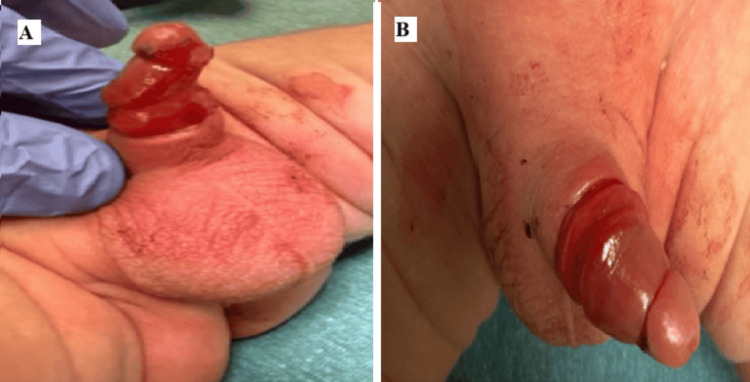 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenital Health and Disease · Urological Disorders and Treatments · Female Genital Mutilation/Cutting Issues
Introduction
The Plastibell device is widely used for neonatal circumcision because it is simple to apply and generally well tolerated. The ring is designed to detach spontaneously within several days; contemporary series report typical separation around one week, which helps define when a device should be considered “retained” [1]. Retained or proximally migrated rings are a recognized complication that can lead to edema and urinary obstruction. In the event of delayed presentations, retained rings can cause penile incarceration or tissue injury, underscoring the need for timely and effective bedside management [2,3].
Multiple strategies for removal have been described, including release of the ligature with gentle manipulation, lubrication, or osmotic reduction to decrease edema, and mechanical division of the plastic ring using scissors or dedicated ring-cutting instruments; emergency department case reports provide step-by-step guidance for ring-cutter removal when simple measures fail [4,5]. Real-world cohort data also show that retained ring is among the most common Plastibell complications and that event rates are higher in infants than neonates, which explains the practical need for reliable bedside options [6].
We report a 15-day-old infant with a retained, proximally migrated Plastibell ring and marked edema in whom scissor division was deemed unsafe, and a ring cutter was unavailable. A handheld, battery-powered fine-tip cautery device was used to melt and divide the plastic ring at the bedside, permitting atraumatic removal without sedation. Based on our literature review, published bedside divisions of retained Plastibell rings predominantly use mechanical tools; we did not identify prior reports describing handheld cautery as the primary method of plastic ring division [4-6]. Because ring devices remain common, strategies for managing ring-specific complications remain clinically relevant [7].
Case presentation
A 15-day-old male infant, born at term and previously healthy, presented to the pediatric emergency department with a retained Plastibell circumcision device. The procedure had been performed on the second day of life. There was no bleeding or urinary retention. Before the urologic consultation, an attempt was made to manually remove the device by cutting the string to release the ligature, but the device did not separate. Initial examination demonstrated that the Plastibell device had migrated over the glans (Figure 1).
Initial examination demonstrating a malpositioned, retained Plastibell device (arrow) associated with marked glans edemaImage courtesy: Used with permission from the patient's mother
There was some discoloration to the corona of the penis that was tucked under the Plastibell ring. There was significant edema of the glans, most notably in the glans distal to the ring. Removal with scissors was deemed unsafe given the deep embedding and risk of iatrogenic injury. A ring cutter was considered but not immediately available, and its bulk would have posed a challenge given the significant edema and small operative field. The decision was made to attempt removal using a handheld battery-operated cautery device (Bovie Disposable High Temperature Fine Tip Cautery, MFI Medical, San Diego, CA) (Figure 2).
Portable electrocautery device used for removal of the Plastibell deviceImage courtesy: Reused with permission from the owner (https://mfimedical.com/products/bovie-disposable-high-temperature-fine-tip-cautery)
With appropriate analgesia and tissue protection using a wet gauze barrier, the cautery device was used to carefully melt through the plastic ring. Cautery was used in brief (less than three seconds) intermittent activations with several seconds of cooling between bursts to limit heat conduction. After careful application of electrocautery for a total of five minutes, the device was successfully divided and removed in one piece. The patient tolerated the procedure well without sedation or complications. Postremoval examination revealed significant glans edema but no signs of vascular compromise, tissue necrosis, or urethral injury (Figure 3).
Examination immediately following removal of the Plastibell device. (A) Lateral view. (B) Dorsal viewSignificant distal glans edema is present following removal, but without vascular compromise, necrosis, or urethral injuryImage courtesy: Used with permission from the patient's mother
The area was cleaned and treated with Bacitracin ointment. The family received thorough discharge instructions and was advised to follow up with their primary care provider. The patient was discharged in stable condition. Five months following removal of the device, the glans has healed normally, and there are no parental concerns with cosmesis.
Discussion
This report describes the successful bedside division of a retained Plastibell ring using a handheld fine-tip cautery device after conventional mechanical approaches were judged unsafe or unavailable. The existing literature predominantly details mechanical strategies, including ligature release through manipulation, scissor division, and the use of orthopedic or umbilical-cord ring cutters [4,5]. Within this context, our experience adds a resource-conscious option when edema, tissue entrapment, or equipment limitations preclude previously described methods. To our knowledge, this is the first reported case describing the use of handheld electrocautery for the removal of a retained Plastibell device. A review of the available literature revealed no prior similar cases.
Technique selection should be individualized. Each technique carries distinct benefits, risks, and resource requirements. Scissors are ubiquitous but may confer a higher risk of iatrogenic laceration when the ring is deeply embedded or visualization is compromised by circumferential edema. Ring cutters provide focused mechanical force and are well documented in stepwise emergency department guidance and small case series [4,5]; however, they are not uniformly stocked and can be cumbersome in a confined field. Operative removal maximizes visualization and tissue protection at the cost of anesthesia exposure and operating room resources. By contrast, handheld fine-tip cautery allows incremental thermoplastic weakening of the ring and precise division with minimal traction, potentially facilitating removal without sedation in selected presentations. Although we did not identify prior reports describing handheld cautery as the primary bedside method to divide a retained Plastibell ring, electrocautery is used in related contexts to cut or segment non-tissue foreign bodies (e.g., endobronchial electrocautery snares for impacted airway objects) when mechanical techniques are impractical, supporting the plausibility of a controlled, device-directed thermal approach [8,9].
Timely identification and triage of delayed ring separation are also important. Most Plastibell devices separate within approximately one week, and systems that prompt reassessment beyond this interval can expedite intervention and reduce complication risk [1,10]. Proximal migration with incarceration or evidence of tissue compromise (e.g., dusky glans, bleeding from the meatus, or obstructive symptoms) should prompt urgent evaluation and, when indicated, operative removal to mitigate the well-described risks of fistula formation and partial glans necrosis [2,3].
Thermal safety is paramount. Although the cautery was directed exclusively at the plastic ring in our case, any technique employing heat risks collateral thermal injury if energy is not meticulously confined. Recommended safeguards include interposing wet gauze or a thin metallic barrier between ring and tissue, using brief intermittent activations, avoiding continuous traction near the corona, and employing suction for smoke management. Contemporary reports of postcircumcision penile ischemia further justify a cautious approach and a low threshold for escalation when there is concern for vascular compromise [11].
Beyond technique selection, clear parent-facing education is essential; contemporary summaries of normal and abnormal post-Plastibell features provide practical visuals to reduce unnecessary returns while flagging true complications [12].
This report has limitations. It reflects a single case with an uncomplicated course; thus, external validity and generalizability are necessarily limited. Procedural success likely depends on operator familiarity with handheld cautery and adherence to thermal-protection measures. Comparative effectiveness vs. mechanical techniques cannot be inferred from this experience alone and warrants confirmation in additional cases or case series.
In summary, handheld fine-tip cautery may be considered as a selective bedside option for retained Plastibell rings when mechanical division is unsafe or unavailable, provided that rigorous thermal-safety precautions are observed and institutional protocols support its use. Further reports are needed to delineate indications, standardize procedural safeguards, and compare outcomes with established mechanical approaches [4-6].
Conclusions
Retained Plastibell rings, though uncommon, can cause significant morbidity if not addressed promptly. This case shows that handheld fine-tip cautery may be a feasible bedside option for removal when mechanical methods are unsafe or unavailable. Use should be limited to carefully selected cases with strict tissue protection and operator familiarity, with a low threshold for operative escalation. Further reports are needed to define indications and compare outcomes with established mechanical approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Circumcision with the Plastibell technique: a descriptive case series Cureus Ahmed N Jan ZU Yasin MD Aurangzeb M 014202210.7759/cureus.30601 PMC 967998836420227 · doi ↗ · pubmed ↗
- 2Penile injuries from proximal migration of the Plastibell circumcision ring J Pediatr Urol Bode CO Ikhisemojie S Ademuyiwa AO 232762010 https://www.sciencedirect.com/science/article/abs/pii/S 14775131090035561957072210.1016/j.jpurol.2009.05.011 · doi ↗ · pubmed ↗
- 3Proximal migration of Plastibell circumcision: two case reports and review of the literature Ann Pediatr Surg Ahmad AM Ahmed SE Mostafa NA Nafisah TI 4182022 https://link.springer.com/article/10.1186/s 43159-021-00138-z
- 4Infant with swollen penis and apparent dysuria Clin Exp Emerg Med Fanny SA Chumpitazi CE 136138720203263570510.15441/ceem.18.086PMC 7348680 · doi ↗ · pubmed ↗
- 5Management of Plastibell circumcision ring migration and glans penis incarceration J Pediatr Surg Case Rep Smith AW Hebra A Mansfield JM Streck CJ 18618812013 https://www.sciencedirect.com/science/article/pii/S 2213576613000547
- 6Plastibell circumcision: comparison between neonates and infants Urol Ann Bawazir OA Alsaiari WRS 347351122020 https://journals.lww.com/urol/fulltext/2020/12040/Plastibell_circumcision__Comparison_between.9.aspx 3377633110.4103/UA.UA_146_19PMC 7992528 · doi ↗ · pubmed ↗
- 7Evaluating safety of ring versus clamp devices in neonatal circumcision: a meta-analysis J Pediatr Surg Ahmad I Tang J Khondker A 1616065920243898706210.1016/j.jpedsurg.2024.06.015 · doi ↗ · pubmed ↗
- 8Utilization of endobronchial electrocautery for removal of an impacted airway foreign body Monaldi Arch Chest Dis Nongpiur VN Mittal S Madan K Mohan A Hadda V 90312020 https://www.monaldi-archives.org/macd/article/view/138310.4081/monaldi.2020.138332735107 · doi ↗ · pubmed ↗