Facial Pain as the Initial Presentation of Rhabdomyosarcoma: A Case Report
Najmeh Anbiaee, Atessa Pakfetrat, Shayan Yousefi, Nasrollah Saghravanian, Samaneh Salari

TL;DR
A rare case of rhabdomyosarcoma presented as persistent facial pain and was only diagnosed after advanced imaging revealed a tumor.
Contribution
Highlights rhabdomyosarcoma as a rare but critical differential diagnosis for unexplained facial pain.
Findings
Facial pain was the initial and misleading symptom of spindle cell/sclerosing rhabdomyosarcoma.
Advanced imaging was essential for identifying the tumor after initial evaluations failed.
The aggressive tumor led to poor outcomes despite chemotherapy.
Abstract
Spindle cell/sclerosing rhabdomyosarcoma (RMS) is an uncommon and aggressive neoplasm, especially in adults. This case details a 35‐year‐old male with a 4‐year history of persistent idiopathic facial pain (PIFP), first misdiagnosed owing to the lack of definitive clinical or radiologic evidence. Advanced imaging ultimately identified a malignant tumor in the infratemporal fossa, which was confirmed as rhabdomyosarcoma through histological examination. Owing to the tumor's inaccessibility, surgical removal was unfeasible, and despite chemotherapy, the cancer advanced, resulting in the patient's death. This example highlights the significance of prompt advanced imaging and interdisciplinary cooperation in detecting uncommon cancers that manifest as persistent pain. Given the diagnostic challenge, this case underscores the critical need to consider rhabdomyosarcoma in the differential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2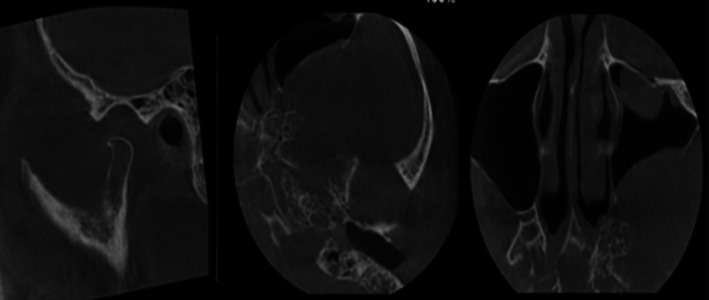 FIGURE 3
FIGURE 3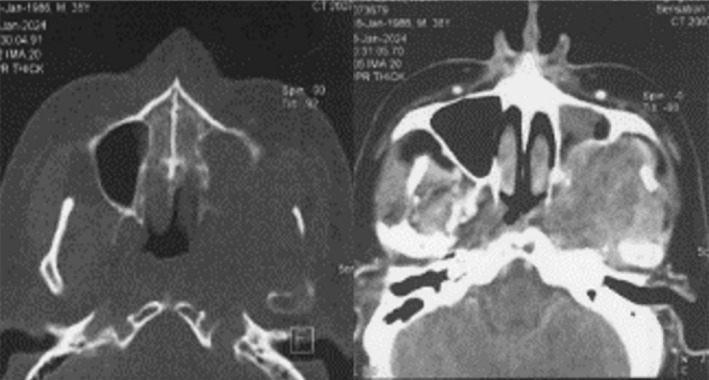 FIGURE 4
FIGURE 4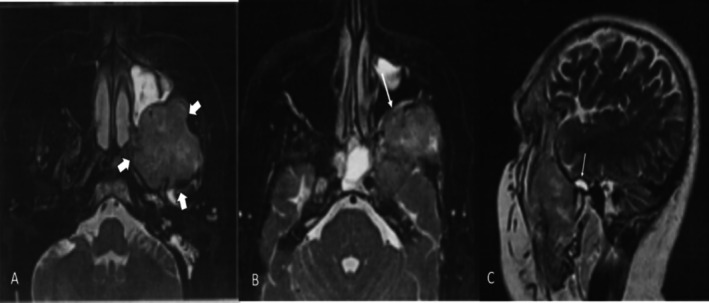 FIGURE 5
FIGURE 5 FIGURE 6
FIGURE 6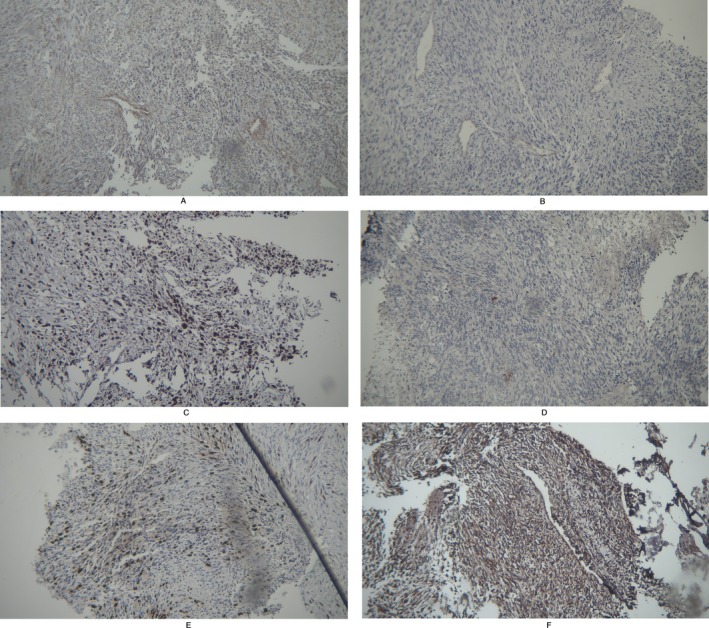 FIGURE 7
FIGURE 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Management of metastatic bone disease · Spinal Hematomas and Complications
Summary
- Facial pain as the initial symptom of rhabdomyosarcoma is rare and can lead to delayed diagnosis.
- Early recognition of persistent, unexplained facial pain as a potential warning sign is crucial for timely intervention and improved patient outcomes.
Introduction
1
Rhabdomyosarcoma (RMS) is a malignant tumor of mesenchymal cells that develop into skeletal muscle. It is the most common soft tissue sarcoma in children and presents a treatment challenge due to its aggressiveness and variety [1, 2, 3]. It is the third most prevalent pediatric extracranial solid tumor, with approximately 250 cases diagnosed annually in the United States [4, 5]. It often occurs in the head and neck, genitourinary tract, and extremities. Also, it can occur in the orbit of the eye [4, 6, 7, 8]. The median age of adult patients with Rhabdomyosarcoma varies, with studies reporting median ages ranging from 28 to 59 years [7, 9, 10].
Genetic and histological factors separate Rhabdomyosarcoma into subgroups. The main subtypes include embryonal, alveolar, spindle cell/sclerosing, and pleomorphic rhabdomyosarcoma. Each subtype differs morphologically and molecularly [11, 12]. Biopsies and molecular analysis are needed for accurate diagnosis. MYOD1 and myogenin immunohistochemistry is often used to confirm the rhabdomyoblastic phenotype [11, 13].
Surgery, chemotherapy, and radiation are usually used. Even with advancements, metastatic and recurrent rhabdomyosarcoma patients have a terrible prognosis, especially high‐risk patients [5, 13, 14]. Survival rates are significantly worse for adults compared to children with similar tumors [15].
This report highlights the diagnostic challenge of persistent idiopathic facial pain (PIFP) when standard evaluations fail to identify a cause. A patient with a four‐year history of persistent idiopathic facial pain, worsening after dental procedures, was initially diagnosed with a nonneoplastic condition. However, a malignant tumor in the infratemporal region was later discovered through advanced imaging. The tumor's aggressive nature, including sinus wall erosion, underscores the need for a multidisciplinary approach. This case emphasizes the importance of comprehensive imaging and collaboration between specialties for early diagnosis and improved outcomes.
Case Presentation
2
A 35‐year‐old male patient presented to the Department of Oral Medicine on December 20, 2023, with complaints of severe, persistent pain localized to the left side of his face (Figure 1). The patient reported that the pain had persisted for approximately 4 years, though it significantly worsened 2 months prior when he sought treatment from a general dentist. During this period, the patient underwent root canal therapy on the left maxillary canine and extraction of the first left premolar, followed by curettage of the extraction site. Unfortunately, the interventions did not provide any relief, and the pain progressively intensified postextraction.
Clinical photograph of the patient.
The patient was referred to an ear, nose, and throat (ENT) specialist, who performed a full assessment but did not identify any abnormalities. After continued pain, the patient was referred to the Department of Oral Medicine for further evaluation.
Upon presentation, the patient exhibited no limitation in mouth opening, and a thorough intraoral and extraoral examination revealed no abnormal findings. However, the patient complained of significant discomfort upon palpation of the ridge, cheek, and tongue, specifically reporting burning sensations. Additionally, he described episodes of severe pain lasting 2–3 h daily, which radiated to the ear, temple, and eye. These episodes were accompanied by sensitivity to light and sound, dizziness, nausea, vomiting, and a persistent salty taste in the mouth. The patient noted that the pain initially began following a period of significant emotional stress and became exacerbated after the dental extractions. Given the complexity of his symptoms, a provisional diagnosis of persistent idiopathic facial pain (PIFP) was made, and the patient was referred to a neurologist for further management. The patient was prescribed carbamazepine, trifluoperazine, and gabapentin, but no significant improvement was observed after 2 weeks.
Methods
3
Consequently, the patient was referred to a neurosurgeon for additional evaluation. The OPG images showed fullness of the left maxillary sinus and increased joint space (Figure 2). The CBCT scans revealed an enlarged temporomandibular joint (TMJ) space and the presence of a solid lesion within the temporomandibular space (Figure 3). This lesion had displaced the posterior wall of the left maxillary sinus anteriorly and caused erosion of the sinus wall. Based on these findings, the differential diagnosis included angiofibroma, lymphoma, malignant nerve sheath tumor, squamous cell carcinoma (SCC), and malignant nasopharyngeal carcinoma.
Panoramic radiograph illustrating maxillary sinus opacification and TMJ space widening.
CBCT imaging demonstrating a solid lesion with posterior maxillary sinus wall erosion.
The patient initially underwent a CT scan (Figure 4). Subsequently, an ultrasound‐guided evaluation was considered to examine the salivary glands, thyroid, and neck. However, due to the absence of detectable lesions, performing a biopsy under ultrasound guidance was not feasible. Given this limitation, an MRI was conducted for further assessment. The MRI revealed a heterogeneous solid mass in the left infratemporal fossa, which had eroded and displaced the posterior wall of the maxillary sinus.
Spiral CT scans revealing the extent of the infratemporal mass and associated bone destruction.
MRI T2 axial and sagittal views showed a medium‐signal, heterogeneous mass occupying the left infratemporal fossa. The lesion caused inflammation, mucositis, and exudate formation within the left maxillary sinus, as well as the temporomandibular joint space. Hyperintense areas within the mass suggested internal hemorrhage or exudate. Moreover, the mass had destructively invaded the posterior wall of the maxillary sinus and penetrated the submucosal layers of the sinus wall (Figure 5).
Representative Magnetic Resonance Imaging (MRI) scan of the patient illustrating the radiological appearance of the lesion.
We reviewed the patient's CBCT, MRI, and CT scans, which confirmed the presence of a mass. The patient was initially referred for biopsy; however, due to accessibility limitations, surgical intervention and biopsy by an oral and maxillofacial surgeon were not feasible. Consequently, the patient was referred for ultrasound‐guided biopsy, but this approach was also deemed impractical. Ultimately, an open surgical biopsy was performed, and the pathological report was as follows.
Histopathological examination of the tumor revealed a malignant neoplasm with a spindle cell morphology, characterized by elongated tumor cells with hyperchromatic nuclei and moderate eosinophilic cytoplasm arranged in intersecting fascicles. The presence of pleomorphic cells and areas of increased mitotic activity suggested an aggressive neoplasm. Immunohistochemical analysis was performed to further characterize the lesion (Figure 6).
Histopathological section of the tumor stained with Hematoxylin and Eosin (H&E) for routine microscopic examination.
The tumor exhibited focal weak positivity for smooth muscle actin (SMA), supporting a mesenchymal origin and indicating partial myogenic differentiation. CD31 was negative, effectively ruling out a vascular endothelial neoplasm. The proliferation index, assessed using Ki‐67, was significantly elevated, suggesting a high mitotic rate and rapid tumor growth. The absence of S100 and SOX10 expression excluded neural and melanocytic differentiation, making diagnoses such as malignant peripheral nerve sheath tumor (MPNST) and melanoma unlikely. Strong positivity for myogenin (MYO) confirmed skeletal muscle differentiation, a key diagnostic feature of rhabdomyosarcoma. Additionally, vimentin showed diffuse positivity, further supporting the mesenchymal nature of the tumor.
Outcome and Follow‐Up
4
Based on the imaging findings, the patient was diagnosed with a malignant tumor, and chemotherapy was initiated, which resulted in a marked reduction in the patient's pain. However, despite the initial improvement in symptoms, the disease proved to be aggressive, and the patient ultimately succumbed to the malignancy. Given the histopathological and immunohistochemical findings, in conjunction with the radiologic and clinical presentation, the diagnosis of spindle cell/sclerosing rhabdomyosarcoma was strongly favored. The tumor's aggressive nature, including its infiltrative growth pattern and high proliferative index, underscores the necessity of a multidisciplinary therapeutic approach involving surgery, chemotherapy, and radiation therapy to improve patient outcomes (Figure 7).
Immunohistochemical staining of the tumor tissue: (A) Smooth Muscle Actin (SMA – Mild positive), (B) CD‐31 (negative), (C) Ki‐67 (positive), (D) S100 (negative), (E) Myogenin (positive), and (F) SOX10 (negative).
Discussion
5
This case presents an unusual and diagnostically challenging instance of spindle cell/sclerosing rhabdomyosarcoma (RMS) in the infratemporal fossa of an adult patient. Rhabdomyosarcoma is a rare cancer arising in skeletal muscle that typically impacts children and young adults [4, 5, 16]. Most cases occurred in pediatric patients (44.4%), predominantly in the para‐meningeal region (57.7%), with the alveolar subtype being the most common (43.2%) [17]. Also, the occurrence of rhabdomyosarcoma in the infratemporal fossa is exceedingly rare, as this deep anatomical area contains intricate neurovascular pathways, complicating diagnosis and treatment. Schwannomas and meningiomas were the most common tumors identified in the infratemporal fossa. The most frequent presenting symptoms included facial hypoesthesia and auricular or preauricular pain [18]. A case series showed that head and neck rhabdomyosarcoma affects the neck, maxillary sinus, nasal cavity, cheek, and infratemporal fossa. Lymph node involvement was common, and distant metastases were observed in some cases, particularly in alveolar and pleomorphic subtypes. Prognosis was generally poor in metastatic cases, while spindle cell/sclerotic rhabdomyosarcoma showed better survival [19].
A major challenge in this case was the atypical presentation of symptoms. The patient presented with facial pain, which initially led to an incorrect diagnosis of persistent idiopathic facial pain (PIFP). The chronic pain, exacerbated after dental extractions, delayed the identification of the underlying malignancy. Persistent Idiopathic Facial Pain (PIFP) is a chronic, daily facial pain without a clear neurological cause. Unlike trigeminal neuralgia, it is persistent, unilateral, and lacks autonomic symptoms. Its cause is unclear, requiring multidisciplinary diagnosis and management [20, 21, 22]. Facial pain is often attributed to neuropathic or musculoskeletal disorders, and malignancies in the infratemporal fossa can remain undetected due to the region's deep location and the lack of overt clinical signs.
The diagnostic intricacy was exacerbated by unremarkable results in initial imaging and discussions with many specialists, including dentists, otolaryngologists, and neurologists. Notwithstanding the advancement of symptoms, the exact nature of the disease remained ambiguous until sophisticated imaging (CBCT, MRI, and CT) was conducted, uncovering a solid tumor with aggressive characteristics, including erosion of the sinus wall.
This example highlights the necessity of evaluating malignancy in cases of persistent, unexplained face pain, particularly when conventional therapies are ineffective. Due to the tumor's aggressive and infiltrative characteristics, a multidisciplinary strategy was needed for diagnosis and treatment.
This case underscores the importance of early advanced imaging and multidisciplinary collaboration in diagnosing rare malignancies like infratemporal fossa rhabdomyosarcoma. Persistent, unexplained facial pain warrants thorough investigation, as delayed diagnosis can lead to poor outcomes. Given the tumor's aggressive nature and complex location, surgical options were limited, making chemotherapy and radiotherapy the primary treatments. The poor prognosis of adult‐onset rhabdomyosarcoma highlights the need for heightened clinical suspicion, prompt imaging, and coordinated specialist care to improve early detection and management.
This case underscores the diagnostic difficulties associated with spindle cell/sclerosing rhabdomyosarcoma (RMS) in an adult patient exhibiting persistent idiopathic facial pain (PIFP). The atypical symptoms and postponed diagnosis underscore the necessity of thorough imaging and interdisciplinary cooperation in intricate cases. The tumor's aggressive characteristics and profound anatomical positioning hindered diagnosis and restricted therapy alternatives. This example highlights the imperative for prompt advanced imaging and increased clinical vigilance in individuals experiencing unexplained face pain. Future innovations in targeted therapy and precision medicine may enhance survival rates for adult‐onset rhabdomyosarcoma.
Author Contributions
Najmeh Anbiaee: conceptualization, investigation, visualization. Atessa Pakfetrat: supervision, writing – original draft, writing – review and editing. Shayan Yousefi: writing – original draft. Nasrollah Saghravanian: conceptualization, investigation, supervision, visualization. Samaneh Salari: conceptualization, investigation, visualization.
Consent
Written informed consent was obtained from the patient for the publication of this case report, including all related clinical details and images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. F. Shern , M. E. Yohe , and J. Khan , “Pediatric Rhabdomyosarcoma,” Critical Reviews in Oncogenesis 20, no. 3–4 (2015): 227–243.26349418 10.1615/critrevoncog.2015013800 PMC 5486973 · doi ↗ · pubmed ↗
- 2L. H. Wexler and L. J. Helman , “Pediatric Soft Tissue Sarcomas,” CA: A Cancer Journal for Clinicians 44, no. 4 (1994): 211–247.8019928 10.3322/canjclin.44.4.211 · doi ↗ · pubmed ↗
- 3W. Lawrence, Jr. and J. P. Neifeld , “Soft Tissue Sarcomas,” Current Problems in Surgery 26, no. 11 (1989): 753–827.2686945 10.1016/0011-3840(89)90036-1 · doi ↗ · pubmed ↗
- 4R. Dagher and L. Helman , “Rhabdomyosarcoma: An Overview,” Oncologist 4, no. 1 (1999): 34–44.10337369 · pubmed ↗
- 5A. Zarrabi , D. Perrin , M. Kavoosi , et al., “Rhabdomyosarcoma: Current Therapy, Challenges, and Future Approaches to Treatment Strategies,” Cancers (Basel) 15, no. 21 (2023): 5269.37958442 10.3390/cancers 15215269 PMC 10650215 · doi ↗ · pubmed ↗
- 6J. A. Shields and C. L. Shields , “Rhabdomyosarcoma: Review for the Ophthalmologist,” Survey of Ophthalmology 48, no. 1 (2003): 39–57.12559326 10.1016/s 0039-6257(02)00415-0 · doi ↗ · pubmed ↗
- 7N. Stock , F. Chibon , M. B. Binh , et al., “Adult‐Type Rhabdomyosarcoma: Analysis of 57 Cases With Clinicopathologic Description, Identification of 3 Morphologic Patterns and Prognosis,” American Journal of Surgical Pathology 33, no. 12 (2009): 1850–1859.19898221 10.1097/PAS.0b 013e 3181 be 6209 · doi ↗ · pubmed ↗
- 8R. V. Lloyd , S. I. Hajdu , and W. H. Knapper , “Embryonal Rhabdomyosarcoma in Adults,” Cancer 51, no. 3 (1983): 557–565.6821833 10.1002/1097-0142(19830201)51:3<557::aid-cncr 2820510333>3.0.co;2-e · doi ↗ · pubmed ↗