Autologous Fibroblast Cells in Platelet‐Rich Plasma Injection as a Novel Treatment for Inactive En Coup de Sabre Deformity
Sona Zare, Alireza Jafarzadeh, Maryam Nouri, Elaheh Lotfi, Solmaz Zare, Nastaran Kabiri Samani, Mohammad Ali Nilforoushzadeh

TL;DR
A new treatment using a patient's own fibroblast cells and platelet-rich plasma shows promise for improving skin appearance in a rare form of morphea.
Contribution
This case report introduces a novel combination of autologous fibroblast cell injection and PRP for treating inactive en coup de sabre morphea.
Findings
The treatment improved skin elasticity, hydration, and cosmetic appearance in a 40-year-old woman.
Ultrasound imaging showed increased dermal thickness and density after treatment.
Cutometric and colorimetric assessments confirmed enhanced skin viscoelastic properties and brightness.
Abstract
Morphea is a chronic autoimmune condition characterized by sclerosis and scar‐like changes in the skin and underlying tissues. En coup de sabre represents a rare and severe linear variant of morphea, primarily affecting the frontoparietal scalp and forehead, with a higher prevalence among children and women. The disease often leads to significant cosmetic and functional impairments, posing therapeutic challenges due to its unpredictable course and varying responses to conventional treatments. Current management strategies include topical steroids, calcineurin inhibitors, systemic therapies, such as methotrexate, and ultraviolet (UV) therapy. Additionally, interventions like fat grafting and hyaluronic acid injections have demonstrated some efficacy in restoring tissue volume and improving skin texture. This case report explores an innovative approach using autologous fibroblast cell…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2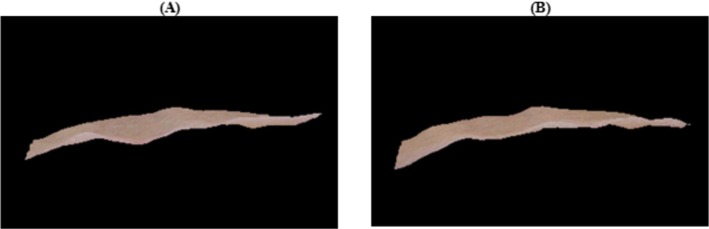 FIGURE 3
FIGURE 3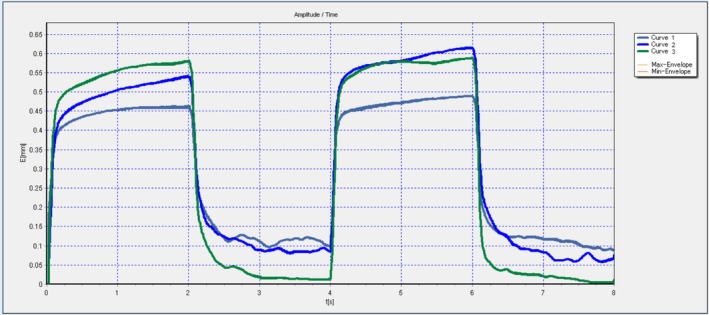 FIGURE 4
FIGURE 4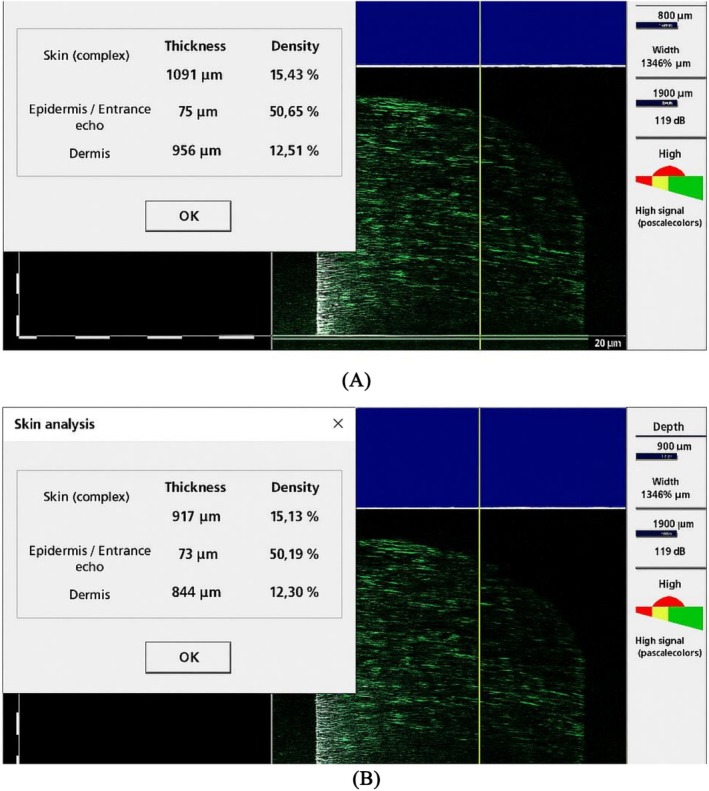 FIGURE 5
FIGURE 5| Outcome | Pre‐treatment | 3‐months follow up |
|---|---|---|
| Corneometer | 48 | 50 |
| Colorimeter | 11 | 16 |
| Mexameter | N/A | N/A |
| Melanin | 296.37 | 290.67 |
| Erythema | 419.33 | 422.00 |
| Cutometer | N/A | N/A |
| R2 | 0.7821 | 0.9759 |
| R5 | 0.4482 | 0.6936 |
| R7 | 0.3486 | 0.4863 |
| Outcome | Pre‐treatment | 3‐month follow‐up |
|---|---|---|
|
| ||
| Epidermis layer | 65 | 75 |
| Dermis layer | 844 | 956 |
| Complete thickness | 909 | 1031 |
|
| ||
| Epidermis layer | 39.8 | 50.98 |
| Dermis layer | 9.69 | 11.63 |
| Complete thickness | 11.91 | 14.54 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeriodontal Regeneration and Treatments · Dermatologic Treatments and Research · Mesenchymal stem cell research
Summary
- This case report highlights the promising results of combining autologous fibroblast cells with platelet‐rich plasma (PRP) injections as a novel, minimally invasive treatment for inactive‐phase en coup de sabre morphea, showing improvements in skin elasticity, thickness, and overall appearance, warranting further investigation in larger studies.
Introduction
1
Morphea, or localized scleroderma, is a rare autoimmune condition primarily affecting the skin and soft tissue, predominantly seen in women [1]. It follows a relapsing–remitting course characterized by alternating phases of inflammation—manifesting as pain, pruritus, erythema, and edema—and fibrosis, marked by dense collagen deposition and yellow‐to‐white plaques. If left untreated, morphea can lead to permanent atrophy and lasting deformity [2].
The pathophysiology of morphea is multifactorial, with immune and fibrotic abnormalities playing central roles. Genetic predisposition, vascular aberrations, trauma, and other environmental triggers are also considered contributing factors [3, 4].
Conventional treatments for active, isolated lesions typically include topical steroids, calcineurin inhibitors, and UV therapy. For more severe or refractory cases, systemic therapies such as methotrexate or mycophenolate mofetil are commonly employed [5].
In recent years, alternative therapies have gained attention. Dermal fat grafting and hyaluronic acid injections have shown effectiveness in improving scalp deformities and addressing inactive scars [6, 7, 8]. Additionally, PRP has emerged as a potential therapeutic option, with reported positive outcomes likely attributed to its high concentration of growth factors that promote tissue remodeling and regeneration [9, 10].
Autologous fibroblast injections have also been explored in dermatology for various applications due to their regenerative properties. In this article, we present a case of a female patient with en coup de sabre morphea successfully treated with a novel combination therapy involving autologous PRP and fibroblast injections.
Case History/Examination
2
A 40‐year‐old woman presented to our dermatology clinic with a two‐year history of a progressive linear depression on her forehead. While she did not report any pain, itching, or discomfort, her primary concern was the cosmetic appearance of the affected area, which she felt had worsened over time.
On physical examination, a well‐defined linear vertical skin depression, approximately 7 cm in length, was observed on the right medial side of her forehead, consistent with an en coup de sabre pattern (Figure 1). The lesion exhibited skin atrophy and mild hypopigmentation, with no signs of erythema, induration, or active inflammation. There was no evidence of associated neurological or ophthalmic abnormalities upon thorough evaluation.
Baseline clinical presentation of en coup de sabre morphea. (A) Right‐sided view showing a distinct linear depression along the patient's forehead, characteristic of en coup de sabre morphea. (B) Frontal view highlighting the extent and location of the atrophic lesion prior to treatment.
Comparison of baseline and 3‐month post‐treatment clinical images. (A, B) Straight‐on frontal views at baseline and 3 months post‐treatment demonstrating visible improvement in skin volume, texture, and contour. (C, D) Right‐side profile views showing notable filling of the linear depression and enhanced skin smoothness following autologous fibroblast‐PRP therapy.
The patient had no history of trauma, autoimmune disorders, or previous medical or cosmetic treatments for her condition. Additionally, no family history of similar dermatological conditions was reported.
Methods
3
A biopsy was taken from the lesion, and histopathological analysis confirmed the diagnosis of en coup de sabre, revealing marked dermal fibrosis, epidermal atrophy, and absence of inflammatory cell infiltration.
To address the patient's cosmetic concerns, a novel autologous fibroblast–PRP therapy was initiated. Following informed consent, a punch biopsy was performed to harvest a small section of superficial dermis from the retroauricular region (posterior to the patient's ear), a site chosen for its minimal sun exposure and higher fibroblast viability. Prior to biopsy, 2% lidocaine was administered intradermally for local anesthesia.
The epidermis was first separated from the dermis by incubation in Dispase II solution (2.4 U/mL; Sigma‐Aldrich, USA) at 4°C overnight. Subsequently, the dermal tissue was enzymatically digested using Collagenase Type I (1 mg/mL; Sigma‐Aldrich, USA) in Dulbecco's Modified Eagle Medium (DMEM; Gibco, USA) at 37°C for 3–4 h to dissociate the dermal fibroblasts. After digestion, the solution was filtered through a 70‐μm cell strainer to obtain a single‐cell suspension. The cells were centrifuged at 1500 rpm for 5 min, resuspended in DMEM supplemented with 10% fetal bovine serum (FBS; Gibco, USA) and 1% penicillin–streptomycin, and cultured in a humidified incubator at 37°C with 5% CO₂.
Fibroblasts at passage 2 were harvested and suspended in freshly prepared platelet‐rich plasma (PRP) solution prior to injection.
Simultaneously, PRP was prepared using a commercially available kit from Pars Fundamental Bio Structure Company, Tehran, Iran. The patient's whole blood was collected and transferred into sterile PRP preparation tubes. The tubes were centrifuged at 1500 Revolutions Per Minute (RPM) for 8 min, and the plasma layer was carefully transferred to a plain tube. A second centrifugation was then performed at 3800 rpm for 8 min. Following centrifugation, the upper two‐thirds of the plasma was discarded, and the remaining plasma was mixed with the platelet pellet at the bottom to create the PRP concentrate.
The cultured autologous fibroblasts were suspended in the freshly prepared PRP under sterile conditions. A total of 5 mL of the fibroblast‐PRP solution was injected subcutaneously into the lesion using a grid‐like injection pattern to ensure even distribution. This procedure was repeated at 1‐month intervals for a total of three sessions to enhance cellular response and tissue remodeling.
Conclusion and Results
4
Epidermal hydration, as assessed through corneometry, did not show significant improvement following the treatment. Similarly, Mexametry results, which measure skin pigmentation and erythema, indicated no considerable differences between the pre‐ and post‐treatment evaluations. These findings suggest that while the intervention may not have directly impacted surface hydration or pigmentation, it did have notable effects on the deeper structural and mechanical properties of the skin (see Table 1, Figures 1, 2, 3).
Three‐dimensional imaging of the affected area. Baseline (A) and 3‐month follow‐up (B) 3D reconstructions illustrating volumetric improvements, softening of the lesion margins, and enhanced skin surface uniformity after treatment.
In contrast, cutometry assessments, which measure the viscoelastic properties of the skin, demonstrated substantial improvements across all three key parameters: R2 (overall elasticity), R5 (net elasticity), and R7 (skin resilience). These enhancements indicate improved skin firmness, elasticity, and the ability to return to its original state after deformation, reflecting a positive impact on the dermal extracellular matrix and collagen architecture (see Figure 4).
Cutometry assessment of skin elasticity. Graphical representation of skin elasticity parameters (R2, R5, R7) pre‐treatment and post‐treatment. Substantial increases in all parameters reflect improved skin firmness, elasticity, and mechanical resilience after therapy.
Skin brightness, evaluated using colorimetry, demonstrated a measurable increase after the injections. This improvement suggests enhanced skin quality and light reflectivity, likely resulting from structural changes in the dermis and improved tissue hydration at a deeper level.
Furthermore, ultrasound imaging was employed to objectively evaluate the thickness and density of the epidermal and dermal layers of the treated skin. The results indicated considerable enhancements in both parameters, with increased skin thickness and improved dermal density noted in comparison to baseline measurements (Table 2, Figure 5). These findings are indicative of effective tissue remodeling and the deposition of new extracellular matrix components facilitated by fibroblasts and PRP growth factors.
Sonographic evaluation of skin thickness and density. (A) Baseline ultrasound showing reduced dermal and epidermal thickness and lower density. (B) Post‐treatment ultrasound at 3 months demonstrating increased thickness and echogenicity, indicating tissue remodeling and regeneration.
Collectively, these objective measurements—cutometry, colorimetry, and ultrasound imaging—corroborate the visible clinical improvements observed in the patient, providing quantitative evidence for the efficacy of the treatment.
Discussion
5
Untreated morphea can result in irreversible structural and cosmetic damage, making effective intervention crucial to mitigate its long‐term consequences. In this case report, we described a novel therapeutic approach combining intralesional PRP and autologous fibroblast injections in a patient with inactive‐phase en coup de sabre morphea. The outcomes demonstrated promising improvements in both skin texture and elasticity, suggesting this treatment modality as a potential therapeutic option.
While the precise mechanism underlying the observed improvements remains unclear, existing evidence highlights the role of autoimmunity and fibroblast dysregulation in the pathogenesis of morphea. Studies have shown that lymphocytic infiltration and elevated cytokine levels play a critical role in disease progression [11]. Elevated Th2 lymphocyte activity leads to increased secretion of interleukin‐4 (IL‐4) and transforming growth factor‐beta (TGF‐β), both of which stimulate fibroblast activation and excessive collagen deposition [12]. Additional cytokines, including IL‐13, IL‐12, and interferon‐gamma, further contribute to fibrotic changes [13].
Another proposed mechanism suggests that vascular endothelial damage in the early stages of morphea triggers cytokine release, which in turn recruits lymphocytes. These lymphocytes release additional cytokines, perpetuating the fibrotic response [14].
PRP, which is rich in growth factors and bioactive proteins, has been widely studied for its ability to enhance tissue repair and regeneration [15]. On the other hand, fibroblasts, derived from mesenchymal cells, are essential for maintaining the extracellular matrix (ECM) and facilitating wound healing [16]. Their regenerative potential has been successfully applied across various dermatological conditions, including scar healing, alopecia treatment, and skin repair in amputee stump sites [17].
Furthermore, fibroblasts have demonstrated immunomodulatory properties, including the ability to inhibit T‐cell activity and aggregation. In an experimental study by Jalili et al., fibroblast injections in alopecia areata mouse models, an autoimmune T‐cell‐mediated disorder, resulted in reduced CD4+ and CD8+ lymphocyte infiltration and lower levels of pro‐inflammatory cytokines [18].
The combined use of autologous fibroblasts and PRP in our study was based on the complementary mechanisms of action of these two therapies. PRP, rich in growth factors such as platelet‐derived growth factor (PDGF), transforming growth factor‐beta (TGF‐β), and vascular endothelial growth factor (VEGF), primarily stimulates tissue remodeling, angiogenesis, and collagen synthesis. On the other hand, autologous fibroblasts contribute directly by producing extracellular matrix components and exhibiting immunomodulatory effects that can counteract the fibrotic process characteristic of morphea [10].
While PRP alone has been previously used to promote tissue regeneration in various dermatological disorders, its effects are often transient due to the short‐lived nature of growth factor activity. Similarly, fibroblast therapy alone has demonstrated promise in improving scar quality and dermal architecture but may require multiple sessions and extended time frames to achieve substantial clinical improvements [17].
By combining these two therapies, we aimed to harness the immediate regenerative stimulus provided by PRP along with the sustained, structural remodeling capabilities of fibroblasts, thus offering a synergistic effect [10]. This combined approach potentially leads to more durable and enhanced tissue restoration compared to either treatment alone.
Compared to previous studies, [10, 17] reported moderate improvements in skin texture with PRP monotherapy in sclerotic skin conditions, while Shams et al. [17] demonstrated gradual but significant improvements in scar remodeling using autologous fibroblast injections. However, neither study reported rapid or marked improvements in dermal thickness and elasticity within a short follow‐up period as observed in our case. Furthermore, to our knowledge, no previous studies have investigated the use of combined autologous fibroblasts and PRP therapy specifically for morphea, making our report a novel contribution to the field.
These findings suggest that the combination therapy could offer a superior therapeutic strategy for morphea by simultaneously targeting vascular, fibrotic, and regenerative pathways.
The observed improvement in our patient may be attributed to the combined action of PRP‐derived growth factors and the immunomodulatory effects of fibroblasts. This combination likely disrupted the pathological fibrotic pathways, enhanced cellular repair mechanisms, and improved the structural integrity of the affected skin.
To the best of our knowledge, this is the first documented case exploring the combined use of autologous fibroblasts and PRP for inactive‐phase morphea. While the results are encouraging, larger‐scale studies with controlled clinical trials are necessary to validate these findings, optimize treatment protocols, and better understand the underlying mechanisms driving tissue regeneration in morphea.
Limitations
6
One major limitation of our study is the relatively short follow‐up period of 3 months. Given the slow and insidious progression of en coup de sabre morphea, a longer follow‐up duration would be necessary to fully assess the stability and durability of the treatment outcomes. Future studies with extended observation periods are warranted to validate these preliminary findings.
Author Contributions
Sona Zare: conceptualization, methodology, project administration, supervision. Alireza Jafarzadeh: writing – original draft, writing – review and editing. Maryam Nouri: software, supervision. Elaheh Lotfi: conceptualization, investigation, methodology. Solmaz Zare: visualization, writing – original draft. Mohammad Ali Nilforoushzadeh: conceptualization, project administration, supervision. Nastaran Kabiri Samani: writing – review and editing.
Disclosure
Transparency Declaration: Authors declare that the manuscript is honest, accurate, and transparent. No important aspect of the study is omitted.
Ethics Statement
The researchers were committed to and adhered to the principles of the Helsinki Convention and the Ethics Committee of the Iran University of Medical Sciences at all stages.
Consent
After providing the necessary explanations, written informed consent was obtained from the patient regarding the submission of their clinical condition to medical journals. Additionally, the patient has been assured that their name and personal details will be kept confidential by the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. Knobler , P. Moinzadeh , N. Hunzelmann , et al., “European Dermatology Forum S 1‐Guideline on the Diagnosis and Treatment of Sclerosing Diseases of the Skin, Part 1: Localized Scleroderma, Systemic Sclerosis and Overlap Syndromes,” Journal of the European Academy of Dermatology and Venereology 31, no. 9 (2017): 1401–1424.28792092 10.1111/jdv.14458 · doi ↗ · pubmed ↗
- 2S. Florez‐Pollack , E. Kunzler , and H. T. Jacobe , “Morphea: Current Concepts,” Clinics in Dermatology 36, no. 4 (2018): 475–486.30047431 10.1016/j.clindermatol.2018.04.005 · doi ↗ · pubmed ↗
- 3S. C. Li , “Scleroderma in Children and Adolescents: Localized Scleroderma and Systemic Sclerosis,” Pediatric Clinics of North America 65, no. 4 (2018): 757–781.30031497 10.1016/j.pcl.2018.04.002 · doi ↗ · pubmed ↗
- 4A. S. Bazargan , A. Jafarzadeh , and N. N. Nobari , “Successful Treatment of Resistant Plantar Ulcerative Lichen Planus With Tofacitinib: A Case Report and Comprehensive Review of the Literature,” Clinical Case Reports 11, no. 10 (2023): e 8066, 10.1002/ccr 3.8066.37854265 PMC 10580686 · doi ↗ · pubmed ↗
- 5M. Arthur , N. M. Fett , E. Latour , et al., “Evaluation of the Effectiveness and Tolerability of Mycophenolate Mofetil and Mycophenolic Acid for the Treatment of Morphea,” JAMA Dermatology 156, no. 5 (2020): 521–528.32236497 10.1001/jamadermatol.2020.0035 PMC 7113833 · doi ↗ · pubmed ↗
- 6A. Jafarzadeh , A. Pour Mohammad , H. Keramati , R. Zeinali , M. Khosravi , and A. Goodarzi , “Regenerative Medicine in the Treatment of Specific Dermatologic Disorders: A Systematic Review of Randomized Controlled Clinical Trials,” Stem Cell Research & Therapy 15, no. 1 (2024): 176, 10.1186/s 13287-024-03800-6.38886861 PMC 11184747 · doi ↗ · pubmed ↗
- 7A. Jafarzadeh , A. Pour Mohammad , and A. Goodarzi , “A Systematic Review of the Efficacy, Safety and Satisfaction of Regenerative Medicine Treatments, Including Platelet‐Rich Plasma, Stromal Vascular Fraction and Stem Cell‐Conditioned Medium for Hypertrophic Scars and Keloids,” International Wound Journal 21, no. 4 (2024): e 14557, 10.1111/iwj.14557.38126221 PMC 10961894 · doi ↗ · pubmed ↗
- 8M. Roohaninasab , A. Jafarzadeh , A. Sadeghzadeh‐Bazargan , et al., “Evaluation of the Efficacy, Safety and Satisfaction Rates of Platelet‐Rich Plasma, Non‐Cross‐Linked Hyaluronic Acid and the Combination of Platelet‐Rich Plasma and Non‐Cross‐Linked Hyaluronic Acid in Patients With Burn Scars Treated With Fractional CO 2 Laser: A Randomized Controlled Clinical Trial,” International Wound Journal 21, no. 10 (2024): e 70065, 10.1111/iwj.70065.39358919 PMC 11447842 · doi ↗ · pubmed ↗