Severe Hypokalemic Paralysis Unmasking Renal Tubular Acidosis in a Patient With Sjögren’s Syndrome
Harisanth Rajaram, Sherwin Ganegoda, Kesavan Sivanesan, Aishwarya Chitnis, Naim Ahmadouk

TL;DR
A woman with Sjögren’s syndrome experienced severe muscle paralysis due to low potassium from kidney issues, which improved with intensive treatment.
Contribution
This case highlights HPP as a rare but critical manifestation of SS-related RTA requiring urgent care.
Findings
Acute hypokalemic paralysis occurred in a patient with Sjögren’s syndrome due to distal RTA.
Central potassium and bicarbonate replacement led to significant clinical improvement.
Early recognition and multidisciplinary care are crucial to prevent relapse and improve outcomes.
Abstract
Hypokalemic periodic paralysis (HPP) is a rare but life-threatening complication in patients with Sjögren’s syndrome (SS), often due to distal renal tubular acidosis (RTA) caused by autoimmune-mediated renal damage. We report a case of a woman in her 30s with a history of rheumatoid arthritis and SS who presented with acute, flaccid paralysis secondary to profound hypokalemia from distal RTA, requiring intensive care support. This patient was treated with central potassium and bicarbonate replacement, leading to marked clinical improvement. This report emphasizes the importance of early recognition of HPP as a manifestation of SS-related RTA and underscores why multidisciplinary management and active long-term follow-up are essential to prevent relapse and optimize patient outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
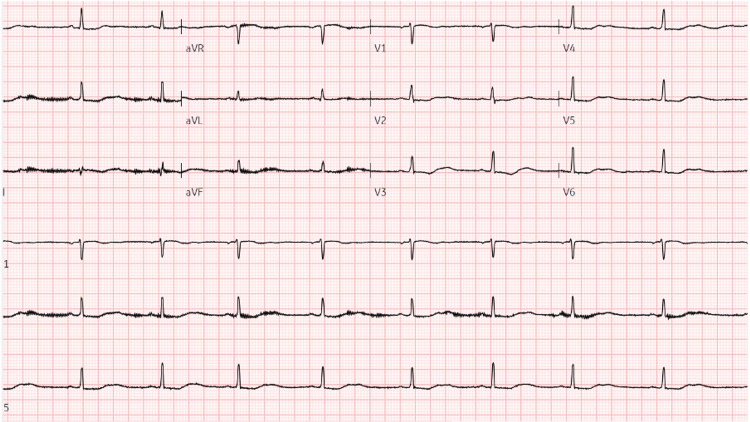 Figure 1
Figure 1| Serum | Initial values | Reference range |
| Sodium (mmol/L) | 139 | 136-145 |
| Potassium (mmol/L) | 1.7 | 3.5-5.1 |
| Magnesium (mmol/L) | 0.8 | 0.7-1 |
| Urea (mmol/L) | 5 | 2.5-6.7 |
| Creatinine (μmol/L) | 95 | 50-98 |
| eGFR (mL/min/1.73 m²) | 68 | >90 |
| Adjusted calcium (mmol/L) | 2.24 | 2.1-2.55 |
| Albumin (g/L) | 38 | 35-50 |
| Chloride (mmol/L) | 116 | 98-107 |
| Creatine kinase (IU/L) | 487 | 29-168 |
| ESR (mm/h) | 65 | 3-12 |
| CRP (mg/L) | 3.3 | 0-5 |
| Blood gas | ||
| pH | 7.18 | 7.35-7.45 |
| Lactate (mmol/L) | 1.7 | 0.5-2.2 |
| HCO3 (mmol/L) | 11.5 | 22-26 |
| Base excess (mmol/L) | -15 | -2-3 |
| Urine | ||
| pH | 7 | 4.5-8.0 |
| Sodium (mmol/L) | 62 | - |
| Potassium (mmol/L) | 8 | - |
| Chloride (mmol/L) | 64 | - |
| 24-hour potassium excretion (mmol/day) | 80 | <30 |
| Urine protein creatinine ratio (mg/mmol) | 66.7 | 0-30 |
| ECG | ||
| Rate (bpm) | 40 | 60-100 |
| QTc (ms) | 590 | <460 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Diabetes and associated disorders · Gastroesophageal reflux and treatments
Introduction
Sjögren’s syndrome (SS) is a chronic autoimmune disorder with a prevalence of up to 2.1% [1]. It is characterized by lymphocytic infiltration of the exocrine glands, most commonly causing sicca symptoms, such as dry eyes and mouth [2]. Renal involvement is one of the more common extraglandular manifestations, with heterogeneous manifestations ranging from electrolyte imbalances to interstitial nephritis, glomerulonephritis, and distal renal tubular acidosis (RTA) [3,4]. RTA can cause profound hypokalemia, a critical electrolyte imbalance that may result in hypokalemic periodic paralysis (HPP) [5]. This case report highlights the importance of recognizing HPP as a manifestation of SS-related RTA, a pertinent differential diagnosis for muscle weakness in a patient with SS.
Case presentation
A woman in her late 30s presented with a four-week history of generalized muscle weakness, myalgia, dysphagia, and progressive dyspnea. She had a past medical history of seropositive rheumatoid arthritis (RA) and SS overlap, and was not on any disease-modifying anti-rheumatic drugs (DMARDs). She reported chronic sicca symptoms (dry mouth and dry eyes), as well as a six-month history of gradually worsening breathlessness. In the days preceding her admission, she developed profound symmetrical weakness in all four limbs and marked fatigue, prompting presentation to the emergency department for further evaluation.
On examination, she was alert and oriented. Her vital signs were as follows: blood pressure 95/63 mmHg, respiratory rate 19 breaths per minute, heart rate 51 beats per minute, temperature 36.2°C, and oxygen saturation 100% on room air. Cardiovascular, respiratory, and abdominal examinations were unremarkable, except for palpable parotid gland enlargement. Neurological examination revealed flaccid quadriparesis, with Medical Research Council (MRC) grade 1/5 strength in all limbs, globally diminished deep tendon reflexes with preserved sensation and cranial nerve function.
Initial venous blood gas analysis revealed a metabolic acidosis (pH 7.18, bicarbonate 11.5 mmol/L, base excess -15 mmol/L, lactate of 1.2 mmol/L). Serum biochemistry revealed normal sodium (139 mmol/L), severe hypokalemia (potassium 1.7 mmol/L), elevated chloride (116 mmol/L), and elevated creatine kinase (487 IU/L). Immunoglobulin screen revealed a polyclonal hypergammaglobulinemia. The estimated glomerular filtration rate (eGFR) was above 60 mL/min/1.73 m². Urinalysis revealed a spot urine pH of 7, 24-hour urinary potassium excretion of 80 mmol/day, urinary anion gap of 6 mmol/L, and a urine protein creatinine ratio of 66.7 mg/mmol. The calculated serum anion gap was 12 mmol/L, consistent with a hyperchloremic normal anion gap metabolic acidosis (Table 1). An electrocardiogram (ECG) demonstrated sinus bradycardia with a prolonged QTc interval of 590 ms (Figure 1).
Patient's ECG on admission.
Imaging included a computed tomography scan of the kidneys, ureters, and bladder, which excluded obstructive uropathy but identified an atrophic right kidney and a bicornuate uterus. An esophago-gastro-duodenoscopy to investigate dysphagia was unremarkable. The elevated creatine kinase prompted an MRI of the femurs, which demonstrated non-specific signal changes in the tensor fascia lata muscles bilaterally, with no radiological evidence of myositis.
Her clinical background, in combination with profound hypokalemia, hyperchloremic normal anion gap metabolic acidosis, increased urinary potassium excretion, and a positive urine anion gap strongly supported a diagnosis of distal (type 1) renal tubular acidosis secondary to SS.
She was promptly admitted to the intensive care unit for urgent management of hypokalemia, where she received central venous catheter (CVC) potassium replacement and peripheral intravenous bicarbonate. After stabilization, she was gradually weaned off CVC potassium replacement and transitioned to high-dose oral therapy with SANDO-K (four tablets, four times daily) and sodium bicarbonate (1 g, four times daily) until discharge.
Prior to discharge, the patient showed significant improvement in her muscle weakness and breathlessness, with normalization of her potassium levels. However, she reported some residual symptoms, including lower limb myalgia, arthralgia exacerbated by cold weather (particularly in the first metatarsophalangeal joints, hand joints, and knees), and ongoing sicca symptoms.
For long-term management, she was started on hydroxychloroquine (200 mg twice daily) with no steroid cover. She had previously tried methotrexate and leflunomide but was unable to tolerate the side effects. She was also prescribed 800 IU of vitamin D daily and advised on the importance of sun protection. With her electrolyte and acid-base balance now stable on oral therapy, she was discharged with active outpatient follow-up by both rheumatology and nephrology.
Discussion
This case demonstrates a classic example of distal renal tubular acidosis (RTA) in the setting of secondary Sjögren’s syndrome, manifesting as severe hypokalemia and flaccid paralysis. The lack of disease-modifying therapy given this patient's background of autoimmunity may have contributed to the development of the severe electrolyte imbalance seen.
Distal RTA is characterized by impaired hydrogen ion secretion in the α-intercalated cells of the distal nephron, resulting in difficulty acidifying urine despite systemic acidosis. Clinically, this results in a normal anion gap (hyperchloremic) metabolic acidosis, often leading to hypokalemia from the urinary potassium wasting. A positive urine anion gap, a urine pH higher than 5.5, and increased urinary potassium excretion are key diagnostic indicators of distal RTA [6].
In SS, distal RTA originates from lymphocytic infiltration and immune-mediated destruction of the distal nephron, leading to interstitial nephritis and tubular dysfunction [7]. Renal involvement occurs in about 5-15% of people with primary SS, and although distal RTA is the most common renal manifestation, it often remains unnoticed until symptoms become severe. This patient displayed the typical traits of HPP, a rare but recognized outcome of distal RTA [8].
The pathophysiology of HPP occurs due to the role potassium plays in maintaining the resting membrane potential and neuromuscular excitability. A reduction in extracellular potassium hyperpolarizes the resting membrane potential, impairing depolarization and reducing the ability of skeletal muscle fibers to generate action potentials. This results in decreased muscle contractility and, in severe cases, produces flaccid paralysis. Additionally, hypokalemia impairs activity of the sodium-potassium ATPase, further disrupting ion gradients critical for neuromuscular function. Clinically, this imbalance manifests as acute, symmetrical, ascending weakness with preserved sensation, consistent with the flaccid quadriparesis observed in this case [9,10].
The flaccid paralysis in all four limbs, weakened reflexes, and preserved sensation are consistent with muscle weakness induced by severe hypokalemia, likely exacerbated by the underlying autoimmune condition. A review of current literature showed that HPP is a rare manifestation of SS, and timely recognition is critical, as delays in potassium correction can lead to respiratory failure, arrhythmias, and even death [5].
ECG features, such as sinus bradycardia, a prolonged QTc interval, and U waves, are well-recognized signs of severe hypokalemia. The QTc of 590 ms in this patient significantly increased the risk of ventricular arrhythmias, such as torsades de pointes, emphasizing the need for urgent critical care monitoring and treatment [11].
The patient’s laboratory profile, characterized by a normal anion gap metabolic acidosis, elevated urinary potassium loss, and high urine pH, met the criteria for diagnosing distal RTA. The presence of an atrophic kidney was most likely a congenital abnormality as her eGFR remained above 60 mL/min/1.73 m², with normal creatinine levels, indicating adequate overall kidney function [12]. A clinical risk-benefit decision was made not to do a renal biopsy at the time of presentation, given the acuity and supportive biochemical findings of distal RTA.
While distal RTA in SS can typically be managed with potassium and bicarbonate supplements, it is imperative that immunomodulatory therapy is given to help prevent recurrences by controlling the underlying autoimmune activity. Hydroxychloroquine, commonly used in treating SS and RA, was appropriately started in this patient, considering her joint pain, fatigue, and autoimmune indications. While no formal protocols for managing RTA in SS exist, case series suggest that approximately one-third of patients respond with supportive therapy alone, while others need corticosteroids or immunosuppressive agents [13].
Conclusions
This case contributes to the small but growing body of literature on SS-related RTA and HPP, emphasizing the need for clinicians to recognize and manage these rare complications. Multidisciplinary care and close monitoring are critical to managing symptoms, preventing relapse, and addressing comorbidities. Importantly, treatment should be tailored to the degree of renal involvement, patient's autoimmune profile, and their risk of relapse. In certain cases, supportive management may be sufficient, whereas in others, immunomodulation may be required for systemic control. Future studies are needed to help develop evidence-based guidelines on electrolyte management and the role of immunosuppressive therapy in preventing recurrent HPP in SS-related RTA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The epidemiology of Sjögren's syndrome Clin Epidemiol Patel R Shahane A 247255620142511459010.2147/CLEP.S 47399 PMC 4122257 · doi ↗ · pubmed ↗
- 2Sjögren’s syndrome Lancet Fox RI 32133136620051603933710.1016/S 0140-6736(05)66990-5 · doi ↗ · pubmed ↗
- 3Current state of knowledge on primary Sjögren's syndrome, an autoimmune exocrinopathy J Clin Med Parisis D Chivasso C Perret J Soyfoo MS Delporte C 9202010.3390/jcm 9072299 PMC 740869332698400 · doi ↗ · pubmed ↗
- 4Primary Sjögren's syndrome N Engl J Med Mariette X Criswell LA 93193937820182951403410.1056/NEJ Mcp 1702514 · doi ↗ · pubmed ↗
- 5Hypokalemic paralysis due to primary Sjögren syndrome: case report and review of the literature Case Rep Rheumatol Garza-Alpirez A Arana-Guajardo AC Esquivel-Valerio JA Villarreal-Alarcón MA Galarza-Delgado DA 2017201710.1155/2017/7509238 PMC 555660328835864 · doi ↗ · pubmed ↗
- 6Renal tubular acidosis: the clinical entity J Am Soc Nephrol Soriano JR 216021701320021213815010.1097/01.asn.0000023430.92674.e 5 · doi ↗ · pubmed ↗
- 7Renal involvement in primary Sjögren's syndrome: a clinicopathologic study Clin J Am Soc Nephrol Maripuri S Grande JP Osborn TG Fervenza FC Matteson EL Donadio JV Hogan MC 14231431420091967966910.2215/CJN.00980209 PMC 2736689 · doi ↗ · pubmed ↗
- 8The occurrence of renal involvement in primary Sjögren's syndrome: a study of 78 patients Rheumatology (Oxford) Pertovaara M Korpela M Kouri T Pasternack A 111311203819991055626510.1093/rheumatology/38.11.1113 · doi ↗ · pubmed ↗