Expression of gamma-aminobutyric acid type A receptor subunit π and minichromosome maintenance-3 in breast cancer patients treated with neoadjuvant chemotherapy: a target molecule or a proliferation marker?
Yakup İriagac, Meltem Oznur, Eyyup Çavdar, Kubilay Karaboyun, Seray Saray, Okan Avcı, Erdoğan Selçuk Şeber

TL;DR
This study examines the expression of two proteins in breast cancer patients treated with chemotherapy to determine their potential as therapeutic targets or indicators of treatment response.
Contribution
The study identifies GABAA receptor subunit π as a potential therapeutic target and shows that MCM3 is not a reliable predictor of treatment response.
Findings
GABAA receptor subunit π is highly expressed in breast cancer cells but not in normal tissue.
MCM3 expression does not correlate with treatment response in breast cancer patients.
Triple-negative breast cancer patients had a higher pathological complete response rate than hormone receptor-positive patients.
Abstract
The receptors and cell membrane channels found in breast cancer in high numbers have been promising for drugs in the past and in the future. In addition, analyses of proliferation indices play an essential role in predicting the success of these treatments. Gamma-aminobutyric acid type A receptor subunit π and minichromosome maintenance-3 expressions were studied by immunohistochemical staining from tissue samples obtained by trucut biopsy from epidermal growth factor receptor 2-negative breast cancer patients who received neoadjuvant chemotherapy. The study included 101 patients. Almost 96.0% of the breast tumor tissues expressed gamma-aminobutyric acid type A receptor subunit π. The median value for gamma-aminobutyric acid type A receptor subunit π was calculated as 30% (19 patients) and the median for minichromosome maintenance-3 as 80% (13 patients). When neoadjuvant chemotherapy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
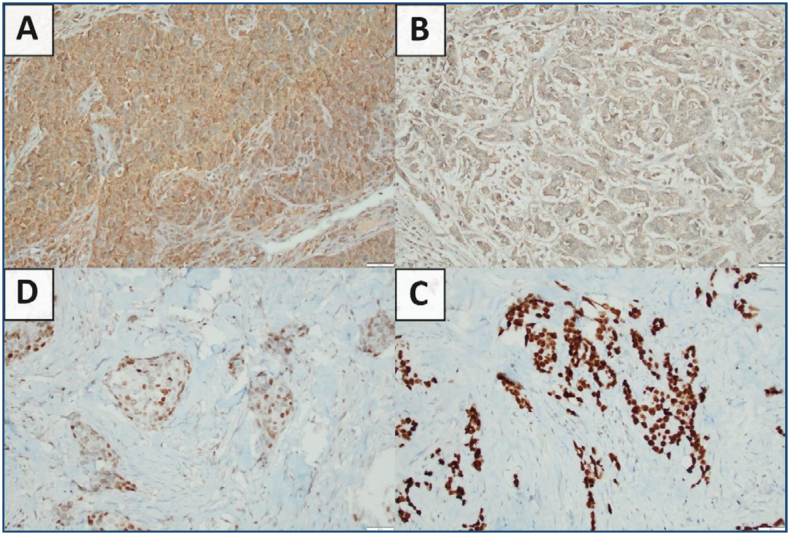 Figure 1
Figure 1| Total (n=101) | pCR (%) (n=24) | ||
|---|---|---|---|
| Age | |||
| <45 | 33 | 13 (39.4) | |
| ≥45 | 68 | 11 (16.2) | |
| Molecular subtype | 0 | ||
| Luminal A-B | 67 | 11 (16.4) | |
| TNBC | 34 | 13 (38.2) | |
| PgR | 0 | ||
| <20 | 51 | 18 (35.3) | |
| ≥20 | 50 | 6 (12.0) | |
| Ki-67 | 0 | ||
| <18 | 16 | 0 (0.0) | |
| ≥18 | 85 | 24 (28.2) | |
| Grade | 0 | ||
| Grade 1–2 | 59 | 5 (8.5) | |
| Grade 3 | 42 | 19 (45.2) | |
| Clinical T stage | 0 | ||
| T1 | 77 | 21 (27.3) | |
| T2-T3 | 24 | 3 (12.5) | |
| Clinical N | 0 | ||
| N0 | 6 | 2 (33.3) | |
| N+ | 95 | 22 (23.2) | |
| Menopause | 0 | ||
| Pre-menopause | 56 | 18 (32.1) | |
| Post-menopause | 45 | 6 (13.3) | |
| GABRP | 0 | ||
| <30 (median) | 39 | 8 (20.5) | |
| ≥30 | 62 | 16 (25.8) | |
| MCM3 | 0 | ||
| <80 (median) | 47 | 13 (27.7) | |
| ≥80 | 54 | 11 (20.4) | |
| Variable | Category | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | ||
| Age | Continuous | 0.956 (0.914–0.999) |
| ||
| Molecular subtype | Luminal/TNBC | 3.152 (1.223–8.122) |
| ||
| ER | Continuous | 0.986 (0.975–0.996) |
| ||
| PgR | Continuous | 0.972 (0.954–0.990) |
| 0.977 (0.959–0.996) |
|
| Ki-67 | <18/≥18 | 1.040 (1.019–1.063) |
| ||
| Nuclear grade | 1–2/3 | 8.922 (2.972–26.786) |
| 6.309 (2.014–19.765) |
|
| Clinical T stage | T1/T2-T3 | 0.381 (0.103–1.411) | 0.149 | ||
| Clinical N | N0/N+ | 0.603 (0.103–3.514) | 0.574 | ||
| Menopause | Pre/Post | 0.325 (0.116–0.906) |
| ||
| GABRP | Continuous | 1.001 (0.983–1.018) | 0.945 | ||
| MCM3 | Continuous | 1.000 (0.984–1.017) | 0.985 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Stress, Anesthesia, and Immune Response · Tea Polyphenols and Effects · Cancer-related Molecular Pathways
INTRODUCTION
According to current data, breast cancer is the most common type of cancer and the second most common cause of cancer-related deaths in women^ 1 ^. One of the preferred treatment options for locally advanced breast cancer is neoadjuvant chemotherapy (NAC). This approach increases the feasibility of breast- and axilla-conserving surgery while also providing the opportunity to evaluate the sensitivity of the tumor to chemotherapy^ 2 ^. Large-scale studies and meta-analyses have demonstrated that achieving a pathological complete response (pCR) following NAC is a strong prognostic indicator for all breast cancer subtypes. In July 2020, the United States Food and Drug Administration (FDA) approved pCR as a safe endpoint for NAC^ 3,4 ^. However, NAC candidate patients should be selected carefully because there is a risk that patients who do not respond may lose their chance at surgery. Moreover, NAC consists of anti-cancer treatments that can lead to significant complications. Additionally, the residual cancer burden (RCB) index stratifies patients into distinct survival groups post-NAC, independent of pCR status^ 5,6 ^. However, in many centers, RCB is not performed as a routine test in daily practice.
Gamma-aminobutyric acid type A receptor subunit π (GABRP) is the π subunit of the GABA-A receptor and is expressed in various non-neuronal tissues^ 7 ^. GABRP, expressed via the receptor on chromosome 5q34, is thought to play a role in the development of breast, ovarian, gastric, cervical, and pancreatic cancer^ 8 ^. Studies have found that GABRP expression is significantly increased in pancreatic cancer tissues, has been associated with poor prognosis, has been found to contribute to tumor growth and metastasis, and has also been shown to have an immunomodulatory function^ 9 ^. In pancreatic cancer, GABRP causes an increase in intracellular calcium levels, and this increase activates the mitogen-activated protein kinase/extracellular signal-regulated kinase (MAPK/ERK) signaling pathway, leading to cancer progression^ 10 ^. In basal-like breast cancer cells, GABRP stimulates migration activities and expression of basal-like cytokeratins via the ERK cascade^ 11 ^. In triple-negative breast cancer (TNBC) stem cells, GABRP has been shown to interact with the epidermal growth factor receptor (EGFR) and maintain EGFR expression, resulting in maintenance of stem cell survival and chemotherapy resistance^ 12 ^.
MCM3, a subunit of MCM, is part of the multimeric Cdc45/Mcm/GINS (CMG) complex that functions as a helicase during DNA replication^ 13 ^. There are studies in the literature reporting that MCM3 is associated with treatment response in tubo-ovarian cancers^ 14 ^. Some studies investigating the role of the MCM protein family in tumor formation and progression in breast cancer have found that high expression of MCM3 is associated with treatment failure or poor prognosis, and have even identified MCM proteins as potential treatment targets^ 15,16 ^. MCM3 has been shown to be a predictive marker of response to endocrine therapy; a coordinated signaling network centered on MCM3 that limits the response to endocrine therapy in estrogen receptor (ER)-positive breast cancer has been revealed, and MCM3 has been identified as a clinically useful prognostic and predictive biomarker that allows personalized treatment of ER-positive breast cancer patients^ 17 ^.
In this study, we aimed to investigate the effects of the π subunit of the GABA-A receptor (GABRP) and MCM3 on chemotherapy responses in breast cancer and to reveal the relationship between them and the clinicopathological data of the patients. In addition, we aimed to validate the hypotheses of GABRP as a "target for drug research" and MCM-3 as a "proliferation marker".
METHODS
Patients
The study included patients with invasive ductal-type breast cancer who received neoadjuvant chemotherapy and then underwent surgery between March 2014 and August 2020 at Tekirdağ Namık Kemal University Hospital. Trucut biopsy samples obtained from primary breast tissue before neoadjuvant chemotherapy were used for immunohistochemical (IHC) staining of MCM3 and GABRP, Ki-67, ER, progesterone receptor (PgR), and nuclear-grade assessments. Other data were obtained from patient records.
The study included patients with human EGFR 2 (Her2)-negative tumors aged 18 years and older with sufficient tumoral tissue for trucut biopsy. All patients had invasive ductal-type histology and received standard chemotherapy. Patients who were HER2-positive, had invasive non-ductal pathology, or received chemotherapy outside of standard treatment, and patients from whom sufficient tissue samples could not be obtained for staining were not included in the study.
Clinical and pathological staging was performed according to TNM 8th Edition. Informed consent was obtained from all patients, and the study received local ethics committee approval (ethical committee protocol: 2020.230.09.17).
Pathological assessments
Paraffin-embedded tissues and hematoxylin–eosin stained preparations previously prepared with trucut biopsy were obtained from the hospital's pathology laboratory archives, and sections were taken with a microtome by two pathology technicians. IHC staining was performed on the sections, and the sections were placed on the BenchMark XT device. Staining procedures were performed using estrogen (SP1. Ventana), progesterone (1E2. Ventana), GABRP (1:1000; ab26055; Abcam, Cambridge, UK), MCM3 (1:1000; PA1651; Boster Bio), HER-2 (anti-HER-2/neu; 4B5. Ventana), and Ki-67 (30-9. Ventana) antibodies. Normal breast tissue was used as an external control. In Her2 staining, no staining out of 3 or 1+ staining was considered negative according to the ASCO/CAP guidelines. Notably, 2+ was separated as Her2-negative and Her2-positive with fluorescence in situ hybridization (FISH)^ 18 ^.
Statistical analysis
All statistical analyses were performed using SPSS 24 (SPSS Inc., Chicago, Ill.), and logistic regression analysis was used in multivariate and univariate model analyses to predict pathological complete response (pCR). The multivariate model was established using the "Forward: Likelihood Ratio (LR)" method. Receiver operating characteristic (ROC) analysis was used and visualized to find the ideal cut-off. The Kolmogorov-Smirnov test was used for the normality test, and Mann-Whitney U test was used for the comparison of non-normally distributed data. p-value below 0.05 was accepted for statistical significance.
RESULTS
A total of 101 patients were included in the study, and both tumor tissues and normal breast tissues were stained using immunohistochemistry. The median age of the patients was 50 years (min: 28, max: 71). A total of 67 patients (66.3%) had luminal-type (A or B) breast cancer, while 34 patients (33.7%) had TNBC. In the pre-treatment clinical staging, 76.2% of the patients were classified as clinical T1, and 94.1% had axillary metastases. Following neoadjuvant chemotherapy, pathological complete response (pCR) was achieved in 24 patients (23.8%). The pCR rates were 39.4% in patients under 45 years of age, 38.2% in TNBC cases, and 45.2% in grade 3 tumors (Table 1).
GABRP and MCM3 staining were performed with IHC (Figure 1A–1D). When normal breast tissue and tumor tissue of all patients were evaluated, there was no GABRP staining in normal breast tissue. In total, 97 patients (96.0%) with breast cancer expressed GABRP, and tissues of 4 patients (4%) did not show staining with GABRP (2 patients HR-positive, 2 patients TNBC). All patients had MCM3 staining (min: 1–max: 100).
Gamma-aminobutyric acid type A receptor subunit π and minichromosome maintenance-3 staining examples [(A) minichromosome maintenance-3 Strong nuclear staining (B) minichromosome maintenance-3 Weak nuclear staining (C) gamma-aminobutyric acid type A receptor subunit π Strong cytoplasmic staining (D) gamma-aminobutyric acid type A receptor subunit π Weak cytoplasmic staining].
When separated by median value for GABRP and MCM3, the median value for GABRP was calculated as 30% (19 patients) and the median for MCM3 as 80% (13 patients). There were 39 patients (38.6%) with a GABRP value below median, 62 patients (61.4%) with the median and above. There were 47 patients (46.5%) with MCM3 below median, 54 patients (53.5%) with the median and above value.
The mean GABRP staining percentage for all patients was 35.6±26.1%, with a mean 33.4±26.1% in HR-positive population and a mean of 39.1±26.1% for TNBC patients. Statistically both groups were similar (p=0.249). There was no correlation between GABRP expression percentage and ER, PR, and Ki-67. The mean staining percentage for MCM3 was 69.1±27.8%, 73.8±25.1 for HR-positive, and 59.9±30.6 for TNBC patients, and there was a statistically significant difference (p=0.025). There was no correlation between Ki-67 and GABRP (r=0.128, p=0.202) and MCM3 (r=-0.147, p=0.141).
When evaluated with ROC analysis, the cut-off value for pCR could not be calculated for GABRP [AUC=0.504 (95%CI 0.370–0.638), p=0.949]. The cut-off value predicting complete response could not be determined for MCM3 [AUC=0.484, (95%CI 0.354–0.614), p=0.814].
When neoadjuvant chemotherapy response was evaluated, pCR was achieved in 23.8% (n=24) of the patients. PCR was achieved in 16.4% of the patients for HR-positive and in 38.2% of the patients for TNBC. When the factors predicting pCR were evaluated by univariate analysis, age (OR 0.956, 95%CI 0.914–0.999, p=0.044), molecular subtype (OR 3.152, 95%CI 1.223–8.122, p=0.017), menopausal status (OR 0.325, 95%CI 0.116–0.906, p=0.032), Ki-67 increase (OR 1.040, 95%CI 1.019–1.063, p<0.001), ER decrease (OR 0.986, 95%CI 0.975–0.996, p<0.006), PgR decrease (OR 0.972, 95%CI 0.954–0.990, p<0.002), grade (OR 8.922, 95%CI 2.972–26.786, p<0.001) predicted treatment response. No significant association was found between treatment response and GABRP.
In multivariate analysis, nuclear grade and PgR formed a model for predicting treatment response (OR 6.309, 95%CI 2.014–19.765, p=0.002; OR 0.977, 95%CI 0.959–0.996, p=0.018, respectively) (Table 2).
DISCUSSION AND CONCLUSION
GABRP is naturally expressed in breast tissue. In breast tissue, GABRP is primarily expressed in myoepithelial/basal cells and is hypothesized to be associated with tissue contraction function^ 19 ^. In the study by Wali et al., 4,467 breast cancers were analyzed, and it was determined that GABRP was expressed at low levels in normal tissues and overexpressed in TNBC^ 20 ^. In their study, the GABRP protein was expressed in approximately half of the breast cancer tissues^ 20 ^. However, in our study, almost all (96%) of the tissues of 101 true breast cancer patients had GABRP-positive staining. This unexpectedly high positivity strengthens the potential of GABRP as a therapeutic target for both ER-positive and TNBC cases. Consistently, Wang et al. also proposed GABRP as a novel therapeutic target for TNBC^ 21 ^. The detection of GABRP expression in 32 patients with TNBC included in our study supports the hypothesis that this receptor is required for both a possible treatment target and carcinogenesis, in line with the literature.
Azuma et al.'s study on human prostate cancer cell lines demonstrated that GABA stimulation increased the production of matrix metalloproteinase (MMP) in vitro and the invasive ability of cancer cells^ 22 ^. Meng et al.'s study revealed that GABRP activates the MEK/ERK pathway, facilitates cell metastasis and tumor growth, and promotes the progression of pancreatic cancer^ 23 ^. Sizemore et al.'s study, following the seed–soil hypothesis, suggested that there may be a relationship between high GABA levels in the CNS and more frequent brain metastasis in TNBC-expressing GABRP^ 11 ^. Packard's study observed a correlation between high GABRP mRNA and preferential metastatic progression to the brain^ 24 ^. Hong et al.'s study found that upregulation of GABRP was associated with tumor cell proliferation and metastasis in the BLBC subtype^ 25 ^.
The study by Løkkegaard et al. found that upregulation of MCMs, including MCM3, was associated with resistance to endocrine therapy in patients with ER-positive breast cancer^ 17 ^. In their study, reducing MCM3 expression in breast cancer cells resistant to endocrine therapy restored drug sensitivity^ 17 ^. Zhao et al. showed that MCM3 is a proliferation marker and that there is a positive correlation with Ki-67, and that high MCM3 is a poor prognostic indicator^ 15 ^. Zou et al. concluded that low MCM3 may be a poor prognostic indicator^ 26 ^. Liu et al. showed that some MCMs may be prognostic markers, but MCM3 is not a prognostic indicator but is overexpressed in breast cancer^ 16 ^. In our study, a negative correlation was found between MCM3 and Ki-67, which was not statistically significant, and it was concluded that MCM3 expression has no effect on chemotherapy response. Indirectly, it was concluded that it is not a strong proliferation marker. However, the conclusion that low expression of MCM3 in TNBC may be a poor prognostic indicator is consistent with the studies by Zou and Liu. Many clinical factors such as heterogeneity of the cohorts and BMI may have had an impact on these results^ 5 ^.
There are some limitations in our study. The main limitation is that GABRP and MCM3 gene expressions could not be examined due to the high study cost. Another limitation is that the prognostic data of our study were immature due to insufficient follow-up, and this data was not included in the study. Another limitation was that the data obtained were retrospective and the sample group was heterogeneous. However, what makes the study strong is that we showed high GABRP in breast tumors in a real patient population, not in the estimated results from databases.
In conclusion, in our study, we showed that GABRP is expressed at a very high rate in breast cancer cells due to its molecular structure and is not expressed in normal breast tissue, and therefore, consistent with the literature, it may be a "potential target" for therapies to be developed. We also concluded that MCM3 is not a proliferation index and cannot predict treatment response, inconsistent with some previous studies. Future studies should evaluate whether GABRP expression correlates with RCB and long-term survival, as RCB has been validated as a prognostic tool in locally advanced breast cancer^ 6 ^.
ETHICS STATEMENT
Approval no: 2020.230.09.17 (Non-Interventional Ethics Committee of Tekirdağ Namık Kemal University).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL Kratzer TB Giaquinto AN Sung H Jemal A Cancer statistics, 2025 CA Cancer J Clin 2025751104510.3322/caac.2187139817679 PMC 11745215 · doi ↗ · pubmed ↗
- 2Cardoso F Kyriakides S Ohno S Penault-Llorca F Poortmans P Rubio IT Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†Ann Oncol 20193081194122010.1093/annonc/mdz 17331161190 · doi ↗ · pubmed ↗
- 3Spring LM Fell G Arfe A Sharma C Greenup R Reynolds KL Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: a comprehensive meta-analysis Clin Cancer Res 202026122838284810.1158/1078-0432.CCR-19-349232046998 PMC 7299787 · doi ↗ · pubmed ↗
- 4FDA Pathological complete response in neoadjuvant treatment of high-risk early-stage breast cancer: use as an endpoint to support accelerated approval guidance for industry. US Dep Heal Hum Serv Food Drug Adm Oncol Cent Excell Cent Drug Eval Res (CDER), Cent Biol Eval Res 2020119 Available from: https://www.fda.gov/media/83507/download
- 5Nobrega GB Mota BS Freitas GB Maesaka JY Mota RMS Goncalves R Locally advanced breast cancer: breast-conserving surgery and other factors linked to overall survival after neoadjuvant treatment Front Oncol 2023131293288129328810.3389/fonc.2023.129328838023121 PMC 10657840 · doi ↗ · pubmed ↗
- 6Gomes Cunha JP Goncalves R Silva F Aguiar FN Mota BS Chequim BB Validation of the Residual Cancer Burden Index as a prognostic tool in women with locally advanced breast cancer treated with neoadjuvant chemotherapy J Clin Pathol 202376423924310.1136/jclinpath-2021-20777134620608 · doi ↗ · pubmed ↗
- 7Yang Y Ren L Li S Zheng X Liu J Li W GABRP is a potential prognostic biomarker and correlated with immune infiltration and tumor microenvironment in pancreatic cancer Transl Cancer Res 202211464966810.21037/tcr-21-202135571651 PMC 9091018 · doi ↗ · pubmed ↗
- 8Juvale IIA Hassan Z Has ATC The emerging roles of π subunit-containing GABAA receptors in different cancers Int J Med Sci 202118163851386010.7150/ijms.6092834790061 PMC 8579298 · doi ↗ · pubmed ↗