Improving Access for Students From Widening Participation Backgrounds Applying to Medical School: A Quality Improvement Project
Shruthi Mankal, Faisa Ali, Chris Jacobs

TL;DR
A pilot program helped students from underrepresented backgrounds feel more confident and prepared when applying to medical school.
Contribution
The study introduces a student-designed program to improve medical school access for widening participation students.
Findings
Confidence in the application process significantly increased after the program.
Students reported greater exposure to life as a doctor as a key benefit.
Interview preparedness and understanding of application-strengthening themes improved significantly.
Abstract
Introduction Students from widening participation (WP) backgrounds - including those attending non-selective state schools, from lower socioeconomic groups, and from underrepresented ethnic groups - have a disproportionately low number of applications to medical school in the United Kingdom. Evidence suggests that such students have limited knowledge of the medical school application process, less support from teachers, and fewer contacts to access work experience. This quality improvement project (QIP) aims to identify challenges faced by students from WP backgrounds when applying to medical school, by implementing a pilot WP programme to address these challenges and improve their confidence and preparedness. Methods Challenges were first identified through a focus group (n = 4) and an anonymised pre-intervention survey. A WP programme was subsequently developed in line with student…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
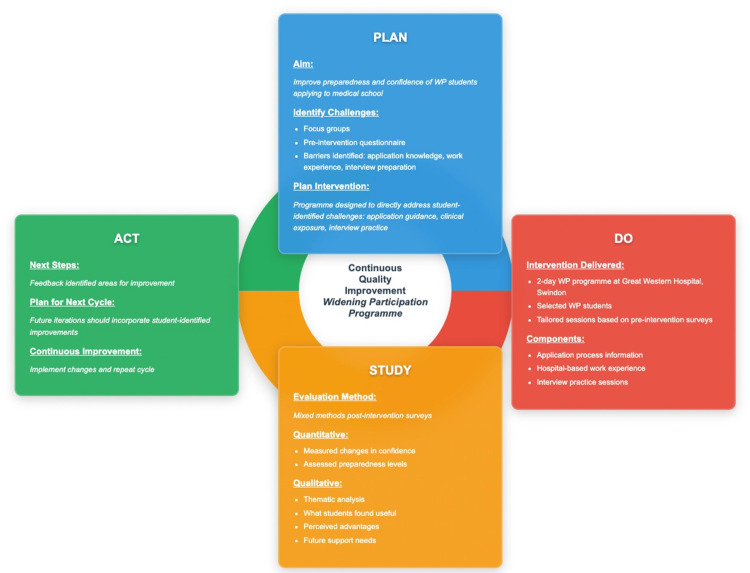 Figure 1
Figure 1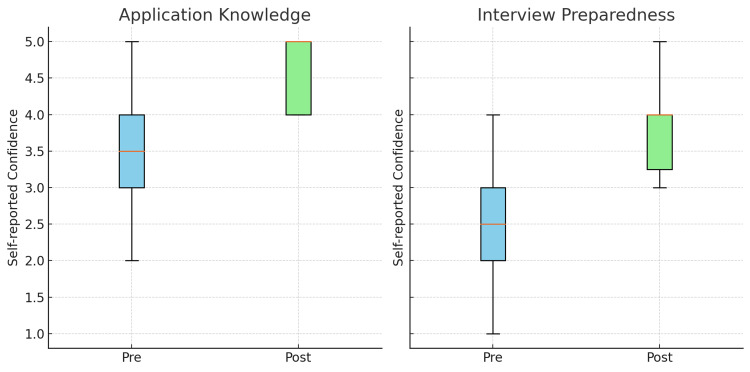 Figure 2
Figure 2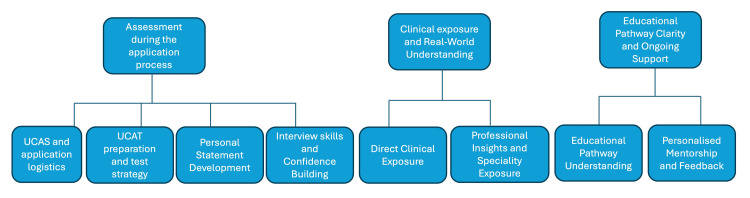 Figure 3
Figure 3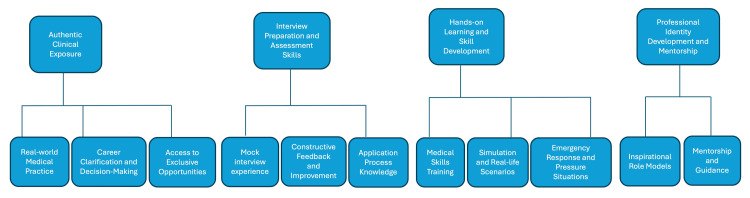 Figure 4
Figure 4| Demographic Category | Subgroup | N | % |
| Gender | Female | 14 | 73.7 |
| Male | 4 | 21.1 | |
| Non-binary | 0 | 0 | |
| Type of School Attended | Non-selective State School | 17 | 89.5 |
| Selective State (Grammar) School | 2 | 10.5 | |
| Independent/Private School | 0 | 0 | |
| Ethnicity | White - British or Other Students | 8 | 42.1 |
| Asian/Asian British - Indian or Pakistani or Other Students | 7 | 36.8 | |
| Mixed/Multiple Ethnic Groups | 2 | 10.5 | |
| Black or Black British - African Students | 2 | 10.5 |
| Theme | Sub-theme | Number of References (Total Number of Participants: n = 16) | % of Participants |
| Assessment During the Application Process | UCAS and Application Logistics | 5 | 31% |
| UCAT Preparation and Test Strategy | 3 | 19% | |
| Personal Statement Development | 3 | 19% | |
| Interview Skills and Confidence Building | 8 | 50% | |
| Clinical Exposure and Real-World Understanding | Direct Clinical Experience | 6 | 38% |
| Professional Insights and Speciality Exposure | 2 | 13% | |
| Education Pathway Clarity and Ongoing Support | Educational Pathway Understanding | 2 | 13% |
| Personalised Mentorship and Feedback | 4 | 25% |
| Theme | Sub-theme | No. of References (Total Number of Participants: n = 18) | % of Participants |
| Clinical and Career Exposure | Real-World Medical Practice | 12 | 67% |
| Career Clarification and Decision-Making | 6 | 33% | |
| Access to Exclusive Opportunities | 3 | 17% | |
| Interview Preparation and Assessment Skills | Mock Interview Experience | 7 | 39% |
| Constructive Feedback and Improvement | 5 | 28% | |
| Application Process Knowledge | 2 | 11% | |
| Hands-On Learning and Skill Development | Medical Skills Training | 1 | 6% |
| Simulation and Real-Life Scenarios | 4 | 22% | |
| Emergency Response and Pressure Situations | 2 | 11% | |
| Professional Identity Development and Mentorship | Understanding Professional Roles | 7 | 39% |
| Inspirational Role Models | 2 | 11% | |
| Mentorship and Guidance | 1 | 6% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Medical Education and Admissions · Global Health Workforce Issues
Introduction
Admission to medical school in the United Kingdom (UK) is characterised by persistent disparities in applicant demographics and success rates. Widening participation (WP) refers to efforts to increase access to higher education for students from underrepresented or disadvantaged backgrounds, including those from lower socioeconomic groups, state-funded schools, and certain ethnic groups [1]. A large retrospective analysis of candidates sitting the UK Clinical Aptitude Test (UCAT), a prerequisite for UK undergraduate medical school entry, demonstrated that 80% of applicants originated from higher socioeconomic groups [1]. The proportion of applicants from independent schools was nearly four times higher than expected, whereas the ratio for those from state-funded schools was only 0.78 of what is expected relative to their representation in the wider population. Students attending private schools have higher acceptance rates into medicine, independent of academic ability, suggesting that additional factors may enhance their applications [2]. Evidence highlights that secondary school students from WP backgrounds face barriers due to limited knowledge of the medical school application process and less support from teachers knowledgeable about the application process [3]. Furthermore, inequalities within WP groups are evident, with some students able to secure work experience placements through personal networks, while others lack such opportunities. Representation also varies across ethnic groups, as UK medical school admission ratios differ tenfold between applicants identifying as Asian students (over-represented) and those identifying as White students (under-represented) [4].
WP initiatives seek to address these inequities by providing targeted support to students from disadvantaged backgrounds, enabling greater access to higher education opportunities [1]. Previous interventions have shown promise, with a UK-based, medical student-led WP initiative improving participants’ understanding of topics assessed in the application process [5]. However, these initiatives were largely designed around faculty-identified priorities rather than being informed by the specific needs and perspectives of students themselves. This highlights a gap in student-led interventions that are co-designed with, and tailored to, the needs of WP students. This quality improvement project (QIP) aims to identify challenges faced by students from WP backgrounds when applying to medical school, and to implement a pilot WP programme to address these challenges - ultimately aiming to improve confidence and preparedness for applying to medical school.
Materials and methods
Theoretical framework and study design
This QIP followed the Plan-Do-Study-Act (PDSA) framework [6], with the study design outlined in Figure 1. The results of the first PDSA cycle are included, with the report prepared in accordance with the Standards for Quality Improvement Reporting Excellence in Education (SQUIRE-EDU) guidelines (Appendix A) [7]. A mixed-methods approach combined quantitative self-reported data collected pre- and post-intervention with thematic analysis of qualitative free-text responses. A 20-minute focus group (n = 4) was conducted by two researchers to explore students’ perspectives. Participants were recruited from students expressing interest in attending the programme or who had attended an open evening explaining the WP initiative. The focus group followed a semi-structured guide (Appendix B) and was audio-recorded, anonymised, and transcribed. Transcripts were reviewed to identify common themes (Appendix C). Responses to a pre-intervention survey from successful applicants from WP backgrounds informed programme design. Post-programme surveys evaluated outcomes and identified opportunities for improvement, which we will state as actionable steps for Cycle 2.
Plan-Do-Study-Act (PDSA) cycle implementation for the widening participation quality improvement project.
Participants
Twenty students who are in sixth form from WP backgrounds participated in this pilot programme. Recruitment was conducted through flyers sent to local schools and an open evening held at Great Western Hospital, Swindon, where students interested in pursuing a career in medicine could find out more about the WP programme. All students were invited to complete a standardised application form. Eligibility criteria included being aged 16-18 years and attending a state-funded school. Initial priority was given to students attending non-selective state schools; however, the inclusion criteria were later expanded to include students attending selective state schools, due to the availability of remaining places.
Descriptive results from the anonymised pre-intervention demographics survey (n = 19) are summarised in Table 1. As the project evaluated an educational intervention for school students aged ≥16, without involving patients or clinical staff providing direct patient care, it was classified as an educational QIP. All participants provided informed consent, and data were collected anonymously.
Intervention
This two-day WP programme was conducted at Great Western Hospital, Swindon. On the first day, resident doctors gave talks on the medical school application process, including timelines and the key components of the application. Students attended clinical skills workshops and participated in simulated assessments of unwell patients. Mock panel interviews were conducted to provide interview practice. The second day focused on hospital work experience, with students assigned a full day at either a medical, surgical, or urgent care department at this district general hospital.
Data collection
Pre- and post-intervention data were collected anonymously using online questionnaires (Appendices D and E). The two main assessment criteria for UK medical school entry involve the candidate’s initial application (encompassing the UCAT) exam score and personal statement) and interviews. Hence, confidence scores regarding the medical school application process and interview preparedness were measured using a five-point Likert scale (1 = lowest, 5 = highest), before and after the programme.
A checklist-style question, “What advantages do you feel strengthen your medical application?” was administered pre- and post-programme, allowing participants to select from a predefined list of potential advantages. Free-text responses were also collected to identify the support participants perceived as most useful pre-intervention, and what they found most valuable post-intervention.
Analysis
Anonymous identifiers were used to maintain confidentiality but enable paired analysis of pre- and post-intervention responses. Due to the ordinal nature of Likert scale responses, non-parametric tests were used to assess changes in confidence in knowledge of the application process and preparedness for interviews. Normality was assessed using the Shapiro-Wilk test, which indicated non-normal distribution. Consequently, changes in paired responses were analysed using the Wilcoxon signed-rank test, with effect sizes (r) calculated to quantify the magnitude of change. To assess whether participants identified a broader range of application-strengthening factors after the programme, the number of distinct coded themes in paired pre- and post-intervention responses was calculated and compared using the Wilcoxon signed-rank test. Additionally, McNemar’s test was applied to assess directional changes in theme count. All statistical analyses were performed using R software (v4.5.1; R Foundation for Statistical Computing, Vienna, Austria).
Qualitative data from free-text survey responses underwent reflexive thematic analysis following Braun and Clarke’s six-step method [8]. This involves initial familiarisation with the data, before generating initial codes, searching for themes, reviewing, defining, and naming the themes, and writing a final report. Two researchers - one being a medical educator and the other having a background working in widening access to higher education - independently coded the data, then collaboratively identified common themes through an inductive approach and iterative process.
Results
There were 16 responses to the pre-intervention questionnaire and 18 responses for the post-intervention questionnaire after removing duplicates (pre-programme n = 1 and post-programme n = 2).
Quantitative pre- and post-intervention comparisons
For matched results, there were 14 participants after removing four unmatched responses (due to lack of post-programme responses) and two duplicates.
Confidence in the Application Process and Medical School Interviews
There was a statistically significant increase in participants’ confidence regarding their knowledge of the application process (W = 5.0, Z = -2.87, n = 13, p = 0.003), with a large effect size (r = 0.79). Median scores increased from 3 (IQR: 3-4) before the programme to 4 (IQR: 4-5) afterwards, as demonstrated in Figure 2. Similarly, participants reported greater preparedness for medical school interviews following the intervention (W = 0.0, Z = -2.98, n = 11, p = 0.003), with a large effect size (r = 0.90). Median scores rose from 2 (IQR: 1-3) pre-programme to 3 (IQR: 3-4) post-programme, as seen in Figure 2. These findings suggest that the programme had a meaningful and substantial positive impact on participants’ perceived readiness for the medical school application process.
Boxplots illustrating the differences in self-reported confidence of participants in application knowledge (left) and interview preparedness (right), pre- and post-intervention. Error bars indicate interquartile ranges.
Advantages of Strengthening Medical School Application
Participants reported a significantly greater number of distinct themes post-programme (median = 3, IQR: 2-4) compared to pre-programme (median = 2, IQR: 1-3), indicating an expanded awareness of factors that strengthen a medical application (Wilcoxon signed-rank test, W = 5.5, p = 0.003). Moreover, McNemar’s exact test confirmed a statistically significant shift in thematic breadth: 12 participants identified more themes after the programme than before, while only one showed a decrease (p = 0.003). These findings suggest that the programme not only influenced the frequency of specific themes, such as exposure, but also broadened participants’ overall understanding of what constitutes a strong medical application.
Participants’ open-ended responses describing perceived advantages for their medical school applications were thematically coded into four categories: confidence, knowledge of the application process, exposure to life as a doctor, and connections. McNemar’s tests were used to evaluate whether the frequency of each theme changed significantly following the intervention. Mentions of confidence increased from 7 participants pre-programme to 11 post-programme; however, this change was not statistically significant (χ²(1, n = 14) = not significant, p = 0.45). In contrast, the number of participants identifying exposure to life as a doctor as a key advantage rose markedly from 3 to 12. This increase was statistically significant, indicating that the programme substantially enhanced participants’ awareness of clinical experience as an important application strength (p = 0.004). Mentions of connections remained relatively stable, increasing only slightly from one to four participants, with no statistically significant change observed (p = 1.00).
Qualitative thematic analysis
According to the six steps outlined by Braun and Clarke’s guidelines for performing a thematic analysis [8], key themes and sub-themes were generated for free-text responses to two questions in the pre-intervention and post-intervention questionnaires.
What Type of Support Would Be Most Helpful for You?
Participants in the pre-intervention questionnaire were asked: “What type of support would be most helpful for you - give at least TWO answers.” This questionnaire had 16 responses, after removing one duplicate, from which three broad themes were generated: “assessment during application process,” “clinical exposure and real-world understanding,” and “educational pathway clarity and ongoing support.” Each key theme had further sub-themes, as outlined in Figure 3, with the number of responses discussing each sub-theme outlined in Table 2.
Key themes (first row) and sub-themes (second row) generated from student responses to the question: “What type of support would be most helpful for you (in applying to medical school) - give at least TWO answers.”UCAS, Universities and Colleges Admissions Service; UCAT, UK Clinical Aptitude Test
Assessment during the application process: Of the 16 responses, there were 19 mentions of aspects of the theme “assessment during the application process” and its sub-themes. The most popular sub-theme by far was “interview skills and confidence building,” with eight individuals listing it as a type of support that would be most helpful for them. Another popular sub-theme was “UCAS and application logistics,” with five individuals listing it as their most helpful type of support. Students reported that they needed “support in the application process” and guidance on “what I should do in terms of UCAS.”
Clinical exposure and real-world understanding: Clinical experience and exposure to specialities were another theme generated by student responses. There were eight total mentions in the responses, with six of the eight being categorised into the “direct clinical experience” sub-theme. Students felt they would benefit most from “having a clinical placement” and wanted “exposure to life as a doctor.” Two students also mentioned that clinical exposure would be helpful in providing them with professional insights and exposing them to different specialities.
Educational pathway clarity and ongoing support: Finally, students reported that they would find more information about the academic course itself and personalised mentorship useful. Four individuals mentioned that they would benefit from mentorship in various domains, including support with aspects of the application, the interview process, “constructive feedback,” and “personal and wellbeing support.”
What Did You Find Most Useful in This Programme?
The same process was performed for the post-intervention questionnaire. Students answered the question: “What did you find most useful in this programme? Why?” This yielded 18 free-text responses, after removing two duplicates. From these responses, four key themes were generated, including “clinical and career exposure,” “interview preparation and assessment skills,” “hands-on learning and skill development,” and “professional identity development and mentorship.” The key themes and their sub-themes are outlined in Figure 4, with the number of responses to each sub-theme outlined in Table 3.
Key themes (first row) and sub-themes (second row) generated from student responses to the question: “What did you find most useful in this programme? Why?”
Clinical and career exposure: This theme accounted for the majority of student responses to the post-intervention questionnaire, with 12 individuals reporting the sub-theme “real-world clinical practice” as the most useful aspect of the programme - by far the most of any sub-theme. Students reported that the “clinical placement was incredibly useful,” as it showed “what it is like to be a doctor,” instead of just “learning and hearing about it.” Students also found that they had greater “career clarification” and “support with decision-making,” with six individuals identifying this sub-theme as what they found most useful. Students also found the intervention useful in that it was an exclusive experience.
Interview preparation and assessment skills: There were 11 total mentions sorted into this theme, across the sub-themes: “mock interview experience,” “constructive feedback and improvement,” and “application process knowledge.” The most responses were recorded for “mock interview experience,” which had seven responses in total. Students reported that they found the mock interview most useful, as it “is the first one” they’ve done “specifically for Medicine.”
Professional identity development and mentorship: There were 10 overall mentions of “professional identity development and mentorship” across this theme, with the majority falling under the sub-theme “understanding professional roles.” Seven students referenced this as the most useful part of their experience, mentioning that “it was a way to experience real life as a doctor instead of just learning and hearing about it,” and that it was “incredibly useful,” as they did not really “know what you’re getting yourself into unless you experience it.”
Discussion
This pilot study was well-represented in the schooling background of participants: 17 of the 19 who completed the survey were from non-selective state school backgrounds, highlighting that the study successfully targeted students of the correct schooling background when aiming to widen participation. The programme also had clear impacts across three domains: students’ exposure to life as a doctor, confidence in the application process, and interview skills. Notably, “exposure to life as a doctor” showed a statistically significant increase in student responses, from 3 to 12 (p = 0.004), reflecting how the programme provided access to experiences that are otherwise difficult to obtain without personal connections [3,9]. Confidence improved significantly in matched pre- and post-intervention responses [10], while interview skills and preparation were consistently valued, with mock interview practice helping to address recognised gaps for WP students [3]. These domains emerging as those most strongly impacting students across both the quantitative and qualitative analyses is of note; these qualities often constitute the “silent advantages” of students from more privileged backgrounds. By levelling the playing field in these areas, the programme addressed barriers that disproportionately affect applicants from underrepresented groups.
While it has historically been the case that students from minority ethnic backgrounds are less likely to be accepted into medical school - with McManus et al. establishing this in their seminal paper [11] - this is no longer the case. Indeed, as previously outlined, students from certain ethnic minority backgrounds are over-represented as medical school applicants [4]. This refers specifically to students from Asian backgrounds, who were the most over-represented; there was a 600-fold difference in admission ratios between Asian students of the highest social class and Black students of the lowest. This demonstrates that the puzzle of equitable admissions is multi-layered and no longer an issue of ethnic minority groups as a whole being underrepresented [12]. Rather, mobility is being seen within particular ethnic groups, and, more importantly, among members of these ethnic groups with the highest socioeconomic statuses [4]. Evidence consistently indicates that socioeconomic status has a profound impact on the likelihood of admission of students; social gradients can be generated for students who have been accepted into medical school, with the highest proportions coming from the most affluent postcodes and the lowest from the least affluent [1].
It is with this context that the results of our study should be considered. Most students were from a white background (eight), followed closely by students from a South Asian background (seven), compared to only two students from a Black or Black African background. Thus, while the intervention aimed to increase access to medical school, the extent to which it can be considered a comprehensive WP initiative is limited by the relatively low representation of minority ethnic groups. Future programmes of this type may benefit from prioritising the recruitment of students from ethnic backgrounds that remain underrepresented over others in the selection process. Increasing general awareness of the application process via the programme could also directly address historic weaknesses in the applications of students from minority ethnic backgrounds, including being “less qualified” and “applying later on” compared to their white counterparts [11]. Similar corrective measures should be taken to ensure there are students from diverse socioeconomic backgrounds, with students from the most deprived areas being prioritised in future cycles of the programme. Application forms could include questions on postcodes, with areas of highest need conferring priority to students most likely to be selected. Additionally, with the aim of increasing the scale of the programme in future cycles, travel bursaries may be beneficial to ensure student attendance.
Additional limitations of this study include the small sample size (n = 20), which restricts statistical power, preventing subgroup analyses - such as the impacts of ethnic minority status on domains of the intervention reported to be most useful - alongside gender and the type of school attended. The single-centre design restricts external validity, and the absence of a control or comparison group limits causal inference. Furthermore, outcomes were self-reported and measured immediately post-intervention, introducing potential response bias and limiting insight into sustained impact.
Given these limitations, this study should be viewed as an exploratory pilot, with potential replicability at a greater scale in different regions of the UK to provide more robust, statistically well-powered, and generalisable data. Future iterations would benefit from multi-centre implementation, larger and more diverse cohorts, and longitudinal follow-up to assess sustained effects on application success rates. Changes for future cycles should be considered and acted upon in a similar manner to how participants were directly informed of the interventions in this programme. Student feedback will also directly inform its future iterations; as part of the post-intervention questionnaire, students were asked, “What further support would be most beneficial?” Students suggest that ongoing mentorship would improve the programme, further supported by evidence from another WP programme, which found an improved sense of community after establishing “Families,” by pairing prospective medical students with current ones [13]. Responses provided specific, constructive feedback for the next cycle of the WP programme, building on the precedent set in this study of addressing students’ needs by directly implementing their solutions in WP programmes for them and future prospective medical students.
Conclusions
To conclude, this QIP provides preliminary evidence that a pilot WP programme, tailored to students’ needs, increases their knowledge of the application process across various domains - including their exposure to life as a doctor - and improves confidence in navigating applications and interview preparedness. This indicates its utility as a template for future WP programmes, suggesting student-informed approaches could be applied to support underrepresented students more effectively. Large, multi-centre studies are required to better ascertain the reproducibility of results and determine which subgroups of students benefit most. Moving beyond the scope of this study, similar techniques could be used to reduce the attrition rates of these same students in medical school by ensuring their needs are both addressed and well-supported - not just in applying, but also in retaining their positions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fair access to medicine? Retrospective analysis of UK medical schools application data 2009-2012 using three measures of socioeconomic status BMC Med Educ Steven K Dowell J Jackson C Guthrie B 111620162675905810.1186/s 12909-016-0536-1PMC 4711010 · doi ↗ · pubmed ↗
- 2Private schooling and admission to medicine: a case study using matched samples and causal mediation analysis BMC Med Educ Houston M Osborne M Rimmer R 1361520152628971710.1186/s 12909-015-0415-1PMC 4545993 · doi ↗ · pubmed ↗
- 3Widening interest, widening participation: factors influencing school students' aspirations to study medicine BMC Med Educ Martin AJ Beska BJ Wood G Wyatt N Codd A Vance G Burford B 1171820182984368910.1186/s 12909-018-1221-3PMC 5975409 · doi ↗ · pubmed ↗
- 4The standardised admission ratio for measuring widening participation in medical schools: analysis of UK medical school admissions by ethnicity, socioeconomic status, and sex BMJ Seyan K Greenhalgh T Dorling D 1545154632820041521787210.1136/bmj.328.7455.1545 PMC 437150 · doi ↗ · pubmed ↗
- 5Widening participation to medicine: a student-led workshop for medical school applicants Med Ed Publish Ryan B Kitchen A Chan A Gibson H Haque E 130720183807452910.15694/mep.2018.0000130.1PMC 10699362 · doi ↗ · pubmed ↗
- 6Application of continuous quality improvement to medical education Med Educ Wong BM Headrick LA 72815520213279093010.1111/medu.14351 · doi ↗ · pubmed ↗
- 7SQUIRE-EDU (standards for quality improvement reporting excellence in education): publication guidelines for educational improvement Acad Med Ogrinc G Armstrong GE Dolansky MA Singh MK Davies L 146114709420193099857510.1097/ACM.0000000000002750 PMC 6760810 · doi ↗ · pubmed ↗
- 8Using thematic analysis in psychology Qual Res Psychol Braun V Clarke V 7710132006