Reasons for consultations and afflicted body systems in rural areas of The Republic of the Congo: A cross-sectional study
Joseph Axel Ngatse, Gilbert Ndziessi, Ange C. Niama, Tristan M. Lepage, Jérémy T. Campillo, Sébastien D. Pion, François Missamou, Ange A. Abena, Michel Boussinesq, Cédric B. Chesnais

TL;DR
This study examines common health issues and reasons for visiting clinics in rural Congo, finding that fever is the most common reason for consultation.
Contribution
The study provides insights into health patterns in rural Congo using standardized classification for consultations and body systems.
Findings
Fever was the most common reason for consultation (25.7%), followed by headache (8.9%).
Fever or chills was the most afflicted body system (29.7%), followed by the digestive system (21.2%).
Neglected tropical diseases were not commonly reported as reasons for consultation in rural health facilities.
Abstract
In the Republic of the Congo, rural areas are characterized by vulnerable populations and endemic infectious diseases, while health facilities have limited technical capabilities. Our objective was to study the distribution of reasons for consultation and afflicted body systems in rural health facilities. We conducted a cross-sectional study in Bouenza, Lékoumou, and Sangha departments. Individuals attending General Medicine outpatient services of selected health facilities were included in the study between September 2020 and January 2021. Reasons for consultation and afflicted body systems were standardized using the second edition of the International Classification of Primary Care (ICPC-2). The overall results were subsequently stratified by department, sex, and age. Most participants were females (53.2%) and the most attended health facilities for consultation were health care…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
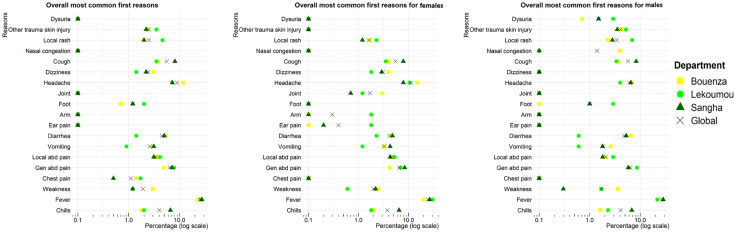 Fig 1
Fig 1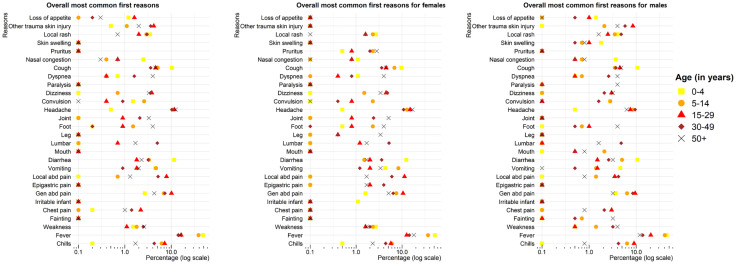 Fig 2
Fig 2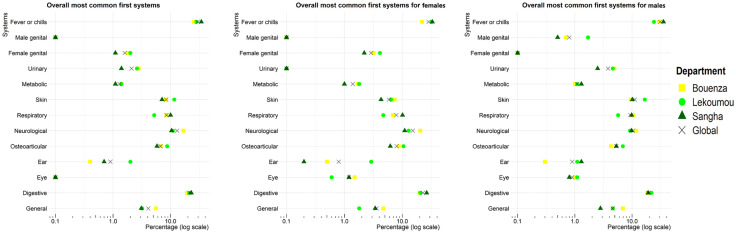 Fig 3
Fig 3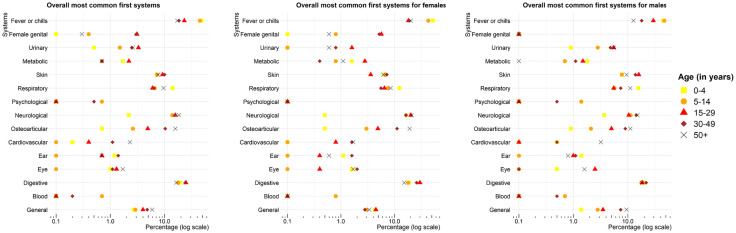 Fig 4
Fig 4- —“Coordination Organization for the Control of Endemics in Central Africa (in French, OCEAC)â€
- —German Federal Ministry for Economic Cooperation and Development (BMZ) and administered by the “Kreditanstalt für Wiederaufbau (KfW)â€
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsZoonotic diseases and public health · Mosquito-borne diseases and control · Dermatological diseases and infestations
Introduction
The epidemiological profile of a population is linked to the morbidity and mortality data available within its geographic region. These data sources collate field surveys, statistical reports generated by nations, and estimates provided by private and international organizations [1,2]. In Sub-Saharan Africa, challenges such as the suboptimal functioning of national health information systems and a dearth of high-quality research data publication in some countries have resulted in deficiencies within national health reports when it comes to producing valuable insights into disease prevalence [3–6]. These shortcomings could hinder countries from developing health policies based on evidence. It is therefore essential to estimate the epidemiological profile of populations to provide more informed guidance on health interventions.
The reasons for consultation, representing patients’ reported complaints to healthcare personnel, influence the course and outcome of medical procedures and inform the diagnostic process. Frequent medical diagnoses help define public health awareness and community screening programs.
Public health facilities in rural areas of the Republic of the Congo are facing significant challenges, including a shortage of qualified personnel, difficulties in accessing the facilities due to geographical and financial constraints, and inadequate diagnostic and treatment infrastructure [7]. In these settings, patient-reported signs and symptoms are often used to diagnose patients, particularly for many neglected tropical diseases (NTD) [8]. It is therefore vital to obtain high-quality data on the reasons for consultation in rural health facilities to gain a deeper understanding of the disease landscape. However, there is a lack of studies conducted in Congo on the distribution of reasons for consultation in rural health facilities settings. To address this gap in knowledge, we conducted a comprehensive investigation to evaluate the distribution of reasons for consultation and afflicted body systems in people living in rural areas in the Republic of the Congo.
Methods
Data analyzed and the STROBE checklist for observational cross-sectional studies [9] are accessible in S1 and S2 Files, respectively.
Study design and period
We conducted a multicenter, cross-sectional analytical study. The data collection period spanned from 23 September to 17 October 2020 for Lekoumou, from 11 September to 12 October 2020 for Bouenza, and from 17 December 2020–18 January 2021 for Sangha.
Study setting
The study was conducted in public health posts and health centers, private hospitals, and public reference hospitals (also known as district hospitals) in three departments of the Republic of the Congo: Bouenza, Lékoumou and Sangha.
In the Republic of the Congo, the health system operates under a pyramid model with the health district as the operational level [10,11]. The health district (inhabitants: 30,000–100,000 in rural areas and 100,000–300,000 in urban areas) is comprised of a district hospital, also called a referral hospital, and an array of health facilities, including health posts, integrated health centers (inhabitants: 2,500–5,000 in rural areas and 5,000–10,000 in urban areas), and private hospitals (such as medical-social centers, medical offices). At the health district level of the national health pyramid, health posts are managed by community health workers or nurses, who refer patients to health centers for primary healthcare. Health centers and private hospitals are managed by nurses or general practitioners, who refer patients to district hospitals for specialized care, including cardiology and gastroenterology care.
The Bouenza department (capital: Madingou) covers an area of 12 265 km² and had an estimated population of 434 925 in 2018. The region features the Niari Valley, which is conducive to agriculture, and a humid tropical climate with corresponding temperatures ranging between 25°C and 30°C. The predominant vegetation includes herbaceous savannas, and plateaus dominate its topography [12]. The Bouenza department has 76 facilities (18 health posts, 16 health centers, 4 referral hospitals, and 38 private hospitals) and is endemic for soil-transmitted helminths (STH), urogenital schistosomiasis, onchocerciasis, lymphatic filariasis, Buruli ulcer [13], and Human African Trypanosomiasis [14]. The department is also empirically characterized by a high frequency of sickle cell disease, diabetes mellitus and hypertension [15].
The Lékoumou department (capital: Sibiti) covers an area of 20 950 km² with an estimated population of 135 643 in 2018. The region features the Chaillu granite massif, which is shared with Gabon, and has a humid tropical climate. The average annual rainfall is 2 200 mm, with temperatures ranging from 19.9°C in July to 24.5°C in March. The department’s vegetation includes vast, dense forests and shrubby savannahs in the south and north [16]. The Lékoumou department has 30 facilities (4 health posts, 21 health centers, 2 referral hospitals, and 3 private hospitals) and its endemic NTDs include leprosy, yaws, STH, onchocerciasis and schistosomiasis [13]. The department is also empirically characterized by a high frequency of sickle cell disease [15].
The Sangha department (capital: Ouesso) covers an area of 55 800 km² and had an estimated population of 120 650 in 2018. The department’s topography is characterized by a flat landscape with elevations consistently above 400 meters. The equatorial climate brings high and constant rainfall (1 600 mm annually), an average temperature of 26°C, and is characterized by a dense primary forests across the majority of the department [17]. The Sangha department has 41 facilities (8 health posts, 9 health centers, 1 referral hospital, and 23 private hospitals) and its endemic NTDs include leprosy, [18], yaws [19] and trachoma [20]. The department is also empirically characterized by a high frequency of hypertension [15].
Sampling strategy and participant selection
A convenience sampling was used to only retain all rural health facilities and all referral hospitals in the health districts of the study departments. An initial selection phase was conducted between September and December 2019 in each department to identify the health facilities eligible for the study. This selection considered their location, the type of health facility, local ecology, and the documented distribution of NTDs in the respective areas. The selection of health facilities was based on two criteria: (i) their location in a rural area, situated more than 15 km away from the referral hospital (for health posts and health centers), and (ii) a minimum daily consultation rate of three patients, as indicated in health facilities’ registries. A total of 44 health facilities were selected according to selection criteria: 7 referral hospitals (4 in Bouenza, 2 in Lékoumou, and 1 in Sangha), 26 health centers (12 in Bouenza, 8 in Lékoumou, and 6 in Sangha), 4 private hospitals (3 medical-social centers and 1 clinic), and 7 health posts in Sangha. In comparison with the other two departments, Sangha had an insufficient number of health centers, which resulted in the selection of health posts and private facilities. The names and geographic coordinates of selected health facilities are presented in S3 File. To enhance clarity regarding abbreviations, a comprehensive list of these abbreviations is presented in S4 File.
Finally, we included all consenting patients who attended General Medicine outpatient services in the three selected departments during the study period. The consent provided was written in French and the two local languages (Lingala and Kituba). Participants who were recruited directly from the community instead of the health facility were excluded. The overall demographic composition of the study sample, representing age groups with a range of five years, reveals an overrepresentation of children under the age of five and females, compared with national population pyramids for 2018 and those of the three study departments, as produced by the National Statistics Institute (S5 File).
Data collection
The data were collected prospectively for each patient during his/her consultation at each health facility by locally trained healthcare staff (community health workers or nurses for health posts, nurses or general practitioners for health centers, private hospitals, and general practitioners for reference hospitals). The data collection process at each respective health facility started for each health facility on the day the data collection tools were provided to the local health staff.
The initial version of the questionnaire was developed in 2019 and subsequently evaluated at 18 health facilities across the three departments towards the end of that same year. Following the receipt of feedback from health personnel, a revised version was developed at the outset of 2020. However, due to the onset of the COVID-19 pandemic, travel to the departments was suspended during this period. Consequently, this new updated version was exclusively assessed at health facilities located on the outskirts of Brazzaville. The definitive version of the questionnaire was officially validated in August 2020. The questionnaire gathered general consultation variables derived from the curative consultation records at the health centers visited. The initial section of the questionnaire documented the reasons for consultation, as reported by the patients (see S6 File).
Data was collected using paper-based questionnaires. This choice was driven by logistical constraints: purchasing electronic tablets for each of the 44 selected health facilities was not cost-effective, and in rural areas, the lack of electricity would have limited the use of electronic devices due to battery depletion. Data collection was prospectively completed by trained local healthcare professionals during patient consultations. We collected data on participants’ demographics (age, sex, occupation), department, type of health facility for consultation, reasons for consultation, and afflicted body systems. Standard body system categories were used (e.g., “abdominal”), with the addition of two separate systems: “general”, for reasons that could not be categorized within a specific body system, and “fever or chills”, designed to reduce the frequency of these two reasons being reported under the “general” system.
Given the variability in the number of reasons for consultation reported by patients, each of the six reasons provided was treated as a separate variable. To ensure consistency in documenting reasons for consultation and affected body systems, we used the International Classification of Primary Care, second edition [21,22]. This classification system, developed in 1998 by the “World Organization of National Colleges, Academies, and Academic Associations of General Practitioners/Family Physicians”, enables comparability across study sites – most of which were primary healthcare facilities (health posts and health centers) – and with other studies conducted in African settings. In ICPC-2, each reason for consultation is coded with a letter representing the afflicted body system, followed by two numbers indicating the specific complaint/reason for consultation [23].
The data from the paper questionnaires were entered into an electronic format using the REDCap mobile application (www.projectredcap.org), a tool developed by Vanderbilt University (Nashville, Tennessee, USA) [24,25]. To ensure accuracy and minimize errors, trained interviewers conducted a double-entry process. Furthermore, the geographic coordinates (longitude and latitude) for each study site were collected using the Global Positioning System smartphone application.
Statistical analysis
The data collected on REDCap was exported to Microsoft Excel 2016 (version 16.0) from Microsoft Office, where it was cleaned. Subsequently, the data was exported for statistical analyses on R 4.0.3 software, utilizing the RStudio 2022.02.03 interface.
As a first step in variable construction, we examined the sequence in which patients reported their reasons for consultation. Accordingly, “reason 1” (R_1_) was defined as the first reason for consultation mentioned by the patient, while “system 1” (S_1_) represented the afflicted body system corresponding to R_1_. The variables R_1-3_ and S_1-3_ referred to the combination of the first three reasons for consultation and their afflicted body systems that a patient expressed, respectively. In a second step, we created the variable “all reasons for consultation”, encompassing all reasons for consultation mentioned by a given patient, regardless of order. Similarly, “all body systems” included all afflicted body systems related to “all reasons for consultation”, without regard to order.
For descriptive statistical analysis, categorical variables were summarized as frequencies and percentages. To compare proportions between groups, we used the Chi-square test. Fisher’s exact test was applied when expected cell counts were below 5 or when assumptions for the Chi-square test were not met. Age was treated as a categorical variable. A two-sided p-value of <0.05 was considered to denote statistically significant results. For each proportion, 95% confidence intervals (95% CI) were computed using either the Wald when np ≥ 5 and n(1 − p)≥5 or Wilson method [26,27]. No statistical test was performed to compare the frequencies of the different combinations of reasons for consultation (R1–R3) as well as first combinations of afflicted body systems, as each combination represented a unique, non-mutually exclusive group. These frequencies are presented descriptively, along with their 95% confidence intervals, to illustrate the most frequently reported patterns.
The results were presented for the overall study population, then stratified by sex, department, and age group. All the most common first reasons for consultation and afflicted body systems were presented, as reported by patients from each study department (see S7 File for description).
Ethical issues
The ethical clearance was obtained from the Health Sciences Research Ethics Committee (CERSSA, in French) on 29 July 2019, under the reference N°166/MRSIT/IRSSA/CERSSA, for a broader study entitled “Assessment of the Burden of Neglected Tropical Diseases in Rural Areas of the Republic of the Congo”. This article is the first in a series of publications on neglected tropical diseases, and a unique sampling and data collection strategy was employed. The study was conducted in accordance with the principles of the Helsinki Declaration [28].
Results
Sociodemographic characteristics of the study population
The study revealed that the largest age group of participants was those aged 15–29 (24.1%), while females (53.2%) and students (20.5%) were the most frequent (Table 1).
Table 1: Study sites and characteristics of the 1876 patients.
Reasons for consultation
Overall distribution.
According to the ICPC-2 classification, the distribution of R_1_ indicates that 25.6% (95% CI: 23.7–27.6) of the subjects reported having a fever, with the percentage being consistent across all departments (Table 2). The most frequent R_1-3_ combination (Table 3) was “fever-cough-nasal congestion” (4.5%, 95% CI: 3.5–5.8), followed by “fever-asthenia-anorexia” (2.2%, 95% CI: 1.5–3.3).
Table 2: Top 28 first reasons for consultation. N = 1867.
Table 3: Most frequent combinations of the first three reasons for consultation (N = 1110).
Distribution by sex and department.
Regarding R_1_, patients in Bouenza reported a higher prevalence of headaches (11.6%) and asthenia (3.0%) compared with those in Lékoumou (7.2% and 1.2% respectively, p = 0.006) and Sangha departments (7.2% and 1.2% respectively, p = 0.025). In contrast, patients in Lékoumou had rashes more frequently (4.6%), compared with those in Bouenza and Sangha (2.0% and 2.0% respectively, p = 0.016). Conversely, the proportion of diarrhea was notably lower in Lékoumou (1.4%) compared with Bouenza and Sangha (5.4% and 5.0%, respectively) (p = 0.010). Additionally, patients in Sangha reported a higher frequency of cough (8.1%) and chills (6.6%) compared with those in Bouenza (3.8% and 1.8% respectively, p < 0.001) and Lékoumou (3.5% and 2.0% respectively, p < 0.001).
The findings on R_1_ regarding headache, rash, cough, and chills were consistent within each sex and displayed similar patterns between both sexes. Specifically, joint complaints were more frequent in Bouenza (3.0%) than in Lékoumou (1.2%) or Sangha (0.7%) (p = 0.032). Conversely, complaints about arm issues were exclusively reported in Lékoumou (1.8%, p = 0.006), while ear pain was more frequent in Lékoumou (1.8%) than in Bouenza (0.0%) or Sangha (0.2%) (p = 0.020) (Fig 1).
Distribution of the first reasons for consultation stratified by sex and department.
Distribution by sex and age groups.
The distribution of R_1_ by age group (Fig 2) revealed that children aged 0–4 years had the highest proportions of cough (10.3%) and diarrhea (11.5%), in comparison with children aged 5–14 years (5.1% and 3.3%, respectively), 15–29-year-old individuals (4.6% and 1.8%, respectively), 30–49-year-old individuals (3.6% and 3.2%, respectively), and those aged 50 years and over (4.6% and 2.3% respectively, p < 0.001). The highest proportions of seizures were observed in individuals aged 5–14 years (2.6%), while the percentages were lower in the 0–5 years, 15–29 years, 30–49 years, and 50 years and over (1.5%, 0.4%, 0.9%, and 0.0% respectively, p = 0.014). In the case of generalized or localized abdominal pain, individuals aged 15–29 years had the highest proportions (10.1% and 7.9%, respectively), while lower percentages were observed in the 0–4-year-old (2.7% and 0.0%, respectively), 5–14-year-old (6.9% and 0.7%, respectively), 30–49-year-old (7.3% and 5.2%, respectively), and 50 years and over (4.3% and 1.3% respectively, p < 0.001). For low back pain, the 30–49-year-olds had the highest proportions (5%), compared with the 0–4-year-olds, 5–14-year-old, 15–29-year-old, and 50 years and over (0.0%, 0.0%, 0.7%, and 1.7%, respectively, p < 0.001). Furthermore, individuals aged 50 years and over had the highest proportions of dyspnea (3.9%) and joint complaints (3.3%), compared with 0–4-year-old (0.7% and 0.0%, respectively), 5–14-year-old (0.4% and 0.0%, respectively), 15–29-year-old (0.4% and 0.9%, respectively) and 30–49-year-old age groups (1.6% and 2.1%, respectively) (p < 0.001 for both dyspnea and join complaints).
Distribution of the first reasons for consultation stratified by sex and age group.
Additionally, several reasons for consultation were only reported by females: joint complaints were more prevalent in those aged 50 years and over (5.1%) when compared with the 0–4-year-old, 5–14-year-old, 15–29-year-old, and 30–49-year-old age groups (0.0%, 0.0%, 0.8%, and 2.4%, respectively, p = 0.001). Complaints about leg issues were more frequent in those aged 50 years and over (3.4%), compared with the 0–4-year, 5–14-year, 15–29 year, and 30–49-year age groups (0.0%, 0.0%, 0.4%, and 0.4% respectively, p = 0.004). Epigastric pain was more frequent in those aged 30–49 years (4.0%) compared with the 0–4-year, 5–14-year, 15–29 year, and 50 years and over age groups (0.0%, 0.0%, 2.0%, and 1.7% respectively, p = 0.008).
Several reasons for consultation were exclusively reported by males. These included the loss of appetite, which was more frequent in children aged 0–4 years (1.4%), compared with the 5–14 year, 15–29-year, 30–49 year, and 50 years and over age groups (0.0%, 1.0%, 0.5%, and 0.0% respectively, p = 0.012). Additionally, traumatic skin injuries were more frequent among those aged 15–29 years (8.5%), compared with those aged 0–4 years, 5–14 years, 30–49 years, and 50 years and over (0.0%, 2.1%, 5.8% and 4.0% respectively, p < 0.001). Paralysis was exclusively reported by patients aged 50 years and over (4.0%, p < 0.001), fainting (loss of consciousness) was more common in the 50 years and over (3.2%), compared with the 0–4-year, 5–14-year, 15–29 year and 30–49 year age groups (0.0%, 0.7%, 0.0%, and 0.5% respectively, p = 0.004).
The distribution for each department of the first reasons for consultation, stratified by sex and age (in S8 File), shows proportions higher than 10% of fever for all age groups in all departments. Additionally, the presence of distinct R_1_ with proportions exceeding 10% is observed in the 0–4-year-old age group, including diarrhea in Bouenza (15.4%), localized rash in Lékoumou (10.9%), and cough in Sangha (16.5%). For reasons for consultation considered regardless of their order of expression (in S9 File), the highest proportions were observed for headaches in Bouenza, for the 5–14, 15–29, 30–49 and 50 years and over (12.5%, 12.5%, 11.2%, 12.7%, respectively). Additionally, cough was identified as most frequent in Lékoumou and Sangha in children aged 0–4 years (12.6% and 18.0% respectively). Finally, the “fever-cough-nasal congestion” combination (in S10 File) was observed to be more frequent in Sangha (6.7%), and in 0–4-year-olds (16.2%).
Afflicted body systems
Overall distribution.
The most frequently afflicted body systems related to first expressed reasons for consultation were “Fever or chills” (29.7%, 95% CI: 23.7–27.6), followed by digestive (21.2%, 95% CI: 19.3–23.0), neurological (13.0% 95% CI: 11.5–14.4), and respiratory (8.5%, 95% CI: 7.3–9.8) systems (Table 4). Making a correspondence between each of the first reasons for consultation and a body system, the most frequent combination of systems was “ Respiratory – Respiratory – Respiratory” (3.8%), followed by “Digestive – Neurological – Fever or chills” (3.4%) (Table 5).
Table 4: Afflicted body systems according to first reasons for consultation. N = 1867.
Table 5: Most frequent triplets of afflicted body systems according to the triplets of first reasons for consultation in each patient. N = 1110.
Distribution by sex and department.
Regarding the afflicted body systems in relation to R_1_ (Fig 3), patients in Bouenza more frequently reported neurological system-related complaints (16.8%) and less frequently reported issues with the Ear-Nose-Throat system (0.4%), compared with patients in Lékoumou (11.0%, and 2.0%, respectively) and Sangha (10.4%, and 0.7% respectively, p < 0.001, and p = 0.030 for neurological and Ear-Nose-Throat based complaints, respectively). In contrast, patients in Lékoumou expressed more frequently skin-related complaints (11.6%), compared with those in Bouenza and Sangha (8.3% and 7.1% respectively, p = 0.043).
Distribution of the first afflicted body systems stratified by sex and department.
Distribution by sex and age groups.
The respiratory system (related to R_1_) was more frequently affected in the 0–4-year age group (14.1%), compared with the 5–14-year, 15–29-year, 30–49 year, and 50 years and over age groups (6.6%, 6.0%, 6.4%, and 9.6% respectively, p < 0, 001). The urinary system (related to R_1_) was less frequently affected in 0–4 age group compared with the 5–14-year, 15–29-year, 30–49 year, and 50 years and over age groups (1.5%, 3.3%, 2.5%, and 2.6% respectively, p = 0.048). Furthermore, the osteoarticular system (related to R_1_) was found to be significantly less affected in the 0–4 age group (0.7%) compared with the 5–14-year, 15–29-year, 30–49-year, and 50 years and over age groups (2.6%, 4.9%, 10.3%, and 15.8%, respectively; p < 0.001) (Fig 4).
Distribution of the first afflicted body systems stratified by sex and by age group.
The distribution of afflicted body systems matched to R1 by department, sex and age showed that the osteoarticular system (see S11 File) was more affected in individuals aged 50 years and over across all three departments (Bouenza: 14.1%, Lekoumou: 16.3%, Sangha: 18.4%), as compared with the age groups 0–4, 5–14, 15–29, and 30–49 years (Bouenza: 0.7%, 1.2%, 5.3% and 10.3%, Lékoumou: 1.8%, 4.2%, 2.9% and 12.3%, Sangha: 0.5%, 2.8%, 5.2%, and 9.3%, p < 0.05). A similar pattern for osteoarticular system was identified across all departments, for all the reasons for consultation that were expressed, irrespective of the order in which the underlying reasons for consultation were expressed (see S12 File). Finally, the distribution of combinations of afflicted body systems related to R_1_-R_2_-R_3_ (see S13 File) revealed that the combination “Respiratory-Respiratory-Fever or chills” was more prevalent in Sangha department (10.2%) as compared with Bouenza and Lékoumou departments (3.5% and 2.7%, respectively), and was more frequent in children aged 0–4-years (20.5%), as compared with participants aged 5–14, 15–29, 30–49, and 50 years and over (5.0%, 3.1%, 1.1%, and 2.1% respectively, p < 0.05).
Discussion
The objective of this study was to describe the reasons for consultation and afflicted body systems in rural health facilities in three departments of the Republic of the Congo. Fever was the main reason for consultation followed by four reasons for consultation: headache, generalized abdominal pain, cough and diarrhea. Based on the revised ICPC-2 classification, the four most afflicted body systems were, by decreasing order of frequency: “Fever or chills”, digestive system, neurological system, and respiratory system.
Except for a few publications on specialized hospital units, there is a notable lack of comprehensive data on the distribution of reasons for consultation in rural health facilities in sub-Saharan Africa. The limited available data was presented in theses, particularly in West Africa, and on one or two health facilities [29–43]. In Mali, three similar studies on reasons for consultation in general practice, conducted in 2007 [31], 2013–2015 [41] et 2018 [33] reported that fever was the most prevalent reason for consultation (23%, 26.1%, and 25.4%, respectively), followed by headache for the first study (8%), vomiting for the second (10.6%) and abdominal pain for the last study (12.9%). In Cameroon, a prospective study conducted at the maternal and child prevention center between 1988 and 1989 [32] reported that, fever was also the first expressed reason (56.6%), while in mainly primary public healthcare facilities of Senegal (Diourbel region, during the Grand Magal of Touba) [39] in 2016, it was the second reason (17.2%), preceded by headache (28.4%).
In the Republic of the Congo, studies mainly focused on recruited subjects at the Hospital and specialized units of University Center of Brazzaville [44–47]. Two studies conducted in rural areas were identified. The first study was conducted between January 1982 and January 1983 in the Kouilou department and revealed that diarrhea was the primary reason for consultation among children under two years of age (25.2%) and cough (21.0%) among 2–5-year-olds [37]. The second study was conducted in a semi-rural area in close proximity to Brazzaville [48]. In 1981, digestive and respiratory systems accounted for over 50% of consultations in the 0–4 age group, with fever being a common accompanying symptom. Although NTDs are empirically considered to be common diseases in rural areas of the Republic of the Congo, reasons for consultation related to NTDs were uncommon in this study. Despite the paucity of comparable studies, the primary reasons for consultation and afflicted body systems in the overall population and age sub-groups in Sub-Saharan Africa appear to be similar and remained stable over time.
The high proportion of fever can be attributed to the endemic presence of malaria, which accounts for 54% of the causes of consultation in the Republic of the Congo [7], or to the COVID-19 pandemic, for which fever is the most frequent symptom [49–51]. However, the lack of comparable data prevents us from conducting a comparative analysis and accurately estimating the potential impact of COVID-19. The 2019 health report for the countries of the Economic Community of West African State also revealed malaria to be the leading medical cause of consultation, with 38.4% of the general population, 41.7% of children under 5 and 27.0% of adults aged 25 and over affected [30]. Regarding the high proportion of headaches, the description of R_1-3_ combinations (see S10 File) indicated an association with fever in the 30–49 age group, which is likely to be related to an infectious disease. In contrast, the older population had muscle pain or dizziness, and these headaches may be due to several reasons such as cervical arthralgia, tension headaches or arterial hypertension [52,53]. Frequent complaints of abdominal pain were strongly associated with fever and population 0–29 years old, which may suggest benign infections as well as medical-surgical emergencies [54]. While fever and upper respiratory system infection or otorhinolaryngological issues could be the most probable causes, the high frequency of cough may indicate pulmonary tuberculosis and respiratory allergies due to woodworking activities in the logging companies in the Sangha department could explain the higher frequency of cough reported in Sangha [55].
The NTD-related reasons for consultation (rash and pruritus, convulsion, skin swelling, hematuria) were less frequent in reported first reasons for consultation. This may be attributed to the mild nature of these signs and symptoms, which may not require a consultation. Additionally, the decline in morbidity associated with NTDs following the sustained efforts of mass drug administration for numerous NTDs through control programs in these departments may also contribute to this trend. Furthermore, NTDs are mainly chronic diseases, whereas consultations in rural areas are generally for acute pathologies in the Republic of the Congo. This low frequency of NTDs-related symptoms highlights the necessity for active screening for these diseases in the community, as opposed to the collection of data in health facilities, as demonstrated in our methodology.
Our study was not without limitations. Indeed, the participants were not randomly selected, which may have resulted in the findings not fully reflecting the reality of the selected local areas. Furthermore, the refusal of some participants to respond could lead to nonresponse bias, resulting in an underestimation of the reasons for consultation and afflicted body systems. This underestimation could also be observed for signs and symptoms of diseases that are more prevalent during the rainy season, such as malaria [56,57], as the data collection period was restricted to the dry season.. Moreover, the collection period was limited to one month, which may not have been sufficient for patients with chronic conditions. Also, we only reported reasons for consultation, in other words symptoms, while for a given symptom, there are many differential diagnoses. For instance, malaria may not be the only diagnostic of fever, rash can be associated with conditions such as dengue, chikungunya, leishmaniasis, and scabies, whereas pruritus was encountered in cases of onchocerciasis and scabies [58]. In a context where soil-transmitted helminths are endemic, cough may suggest Loëffler’s syndrome [13]. Due to the limitations, we are unable to provide further extrapolations from our data or to discuss all potential diagnostic possibilities. Despite the limitations, the results provide a valuable source of information for public authorities and health care practitioners, as they offer insight into the reasons for consultation and afflicted body systems for which information is often of poorer quality at departmental level and after stratification by age and sex. The choice of the ICPC-2 questionnaire ensured a standardized categorization of health complaints across diverse primary care settings. This enabled internal comparisons between health posts and health centers—which represented most consultations in our study (11.9% and 55.9%, respectively)—and external comparisons with similar research conducted in sub-Saharan Africa [59–61]. Our experience also highlights the practical challenges of data collection in low-resource settings, where electricity shortages and cost constraints often hinder the use of digital tools.
Since people in these rural areas have little or no access to complementary examinations, we recommend that the authorities ensure the production of this information on a regular basis at the national level. Furthermore, it is recommended that health professionals working in rural health facilities guarantee the quality of the data collected in their consultation registries, take ownership of the results of this research, inform the community and provide effective treatment for diseases associated with the afflicted body systems identified in the results.
Conclusions
This study is the first of its kind in rural areas of the Republic of the Congo. The main reason for consultation was fever, with no difference between departments and “fever or chills” was found to be the most frequently afflicted body system, followed by the digestive system. Rural professionals should be able to well identify digestive signs and pathologies, and referral health facilities should have specialists in this field. To gain a deeper insight into the health status of the rural population in The Republic of the Congo, it is essential to complete these data with the history of diseases, the medical diagnoses made during consultations, and with associated social factors. Furthermore, future similar studies should collect information during rainy seasons as well, given the seasonal nature of several diseases [56,57,62].
Supporting information
S1 FileProject database.(XLSX)
S2 FileStrobe checklist.(DOCX)
S3 FileHealth facilities and geographic coordinates.(XLSX)
S4 FileList of abbreviations.(DOCX)
S5 FilePopulation pyramid.(TIF)
S6 FileSurvey questionnaire.(PDF)
S7 FileSelection procedure.(TIF)
S8 FileFirst expressed reasons for consultation from each department.(DOCX)
S9 FileAll reasons for consultation without order of expression.(DOCX)
S10 FileCombination of reasons for consultation stratified by sex, department and age.(DOCX)
S11 FileFirst expressed afflicted body systems from each department.(DOCX)
S12 FileAll afflicted body systems from each department without order of expression.(DOCX)
S13 FileCombination of afflicted body systems related to reasons stratified by sex, department and age.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22.33069326 10.1016/S 0140-6736(20)30925-9PMC 7567026 · doi ↗ · pubmed ↗
- 2World Health Organization. World health statistics 2022: monitoring health for the SD Gs, sustainable development goals. 2022. p. 131.
- 3Izugbara CO, Kabiru CW, Amendah D, Dimbuene ZT, Donfouet HPP, Atake EH. It takes more than a fellowship program: reflections on capacity strengthening for health systems research in sub-Saharan Africa. BMC Health Serv Res. 2017;17(Suppl 2):696.29219076 10.1186/s 12913-017-2638-9PMC 5773879 · doi ↗ · pubmed ↗
- 4Ezeh AC, Izugbara CO, Kabiru CW, Fonn S, Kahn K, Manderson L, et al. Building capacity for public and population health research in Africa: the consortium for advanced research training in Africa (CARTA) model. Glob Health Action. 2010;3:10.3402/gha.v 3i 0.5693. doi: 10.3402/gha.v 3i 0.5693 21085517 PMC 2982787 · doi ↗ · pubmed ↗
- 5Kabiru CW, Izugbara CO, Wairimu J, Amendah D, Ezeh AC. Strengthening local health research capacity in Africa: the African Doctoral Dissertation Research Fellowship Program. Pan Afr Med J. 2014;17 Suppl 1(Suppl 1):1. doi: 10.11694/pamj.supp.2014.17.1.3729 24624239 PMC 3946224 · doi ↗ · pubmed ↗
- 6Mbondji PE, Kebede D, Soumbey-Alley EW, Zielinski C, Kouvividila W, Lusamba-Dikassa P-S. Health information systems in Africa: descriptive analysis of data sources, information products and health statistics. J R Soc Med. 2014;107(1 suppl):34–45. doi: 10.1177/0141076814531750 24914127 PMC 4109358 · doi ↗ · pubmed ↗
- 7Ministère de la Santé et de la Population (République du Congo). Politique Nationale de Santé 2018-2030 (PNS 2018-2030) [Internet]. 2021 [cited 2022 Jul 3]. Available from: https://sante.gouv.cg/politique-nationale-de-sante-2018-2030-pns-2018-2030/
- 8World Health Organization. Working to overcome the global impact of neglected tropical diseases: first WHO report on neglected tropical diseases [Internet]. World Health Organization; 2010 [cited 2022 Jul 2]. Report No.: WHO/HTM/NTD/2010.1. Available from: https://apps.who.int/iris/handle/10665/44440