Polyostotic Fibrous Dysplasia of the Middle Finger
Tristán Igual-Pacheco, Nicolas De Vos, Jonas De Melio

TL;DR
This paper highlights that fibrous dysplasia should be considered in children with finger lesions and suggests using CT scans for better diagnosis.
Contribution
The paper emphasizes the importance of considering fibrous dysplasia in pediatric finger lesions and recommends CT scans for assessment.
Findings
Polyostotic lesions in pediatric fingers may indicate fibrous dysplasia.
CT scans are useful for identifying ground-glass densities in such cases.
Abstract
Teaching point: When a polyostotic lesion in the fingers is seen in a pediatric patient, fibrous dysplasia should be included in the differential diagnosis and a CT scan should be considered for the assessment of ground-glass densities.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1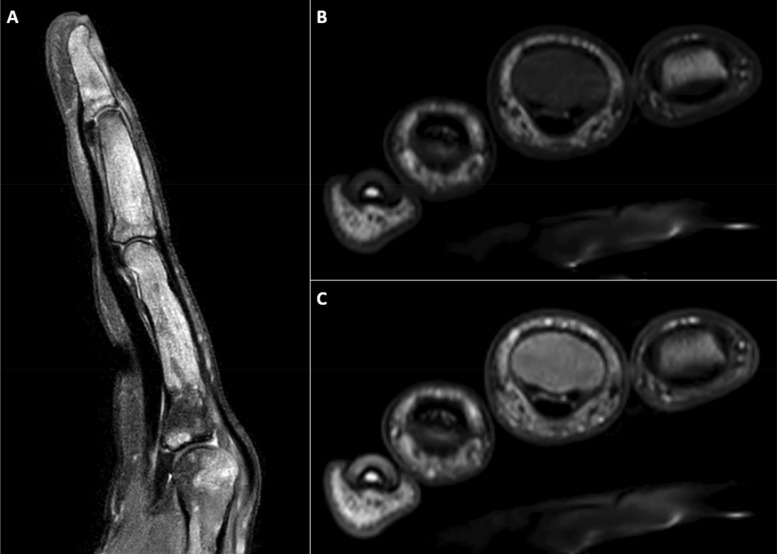 Figure 2 A–C
Figure 2 A–C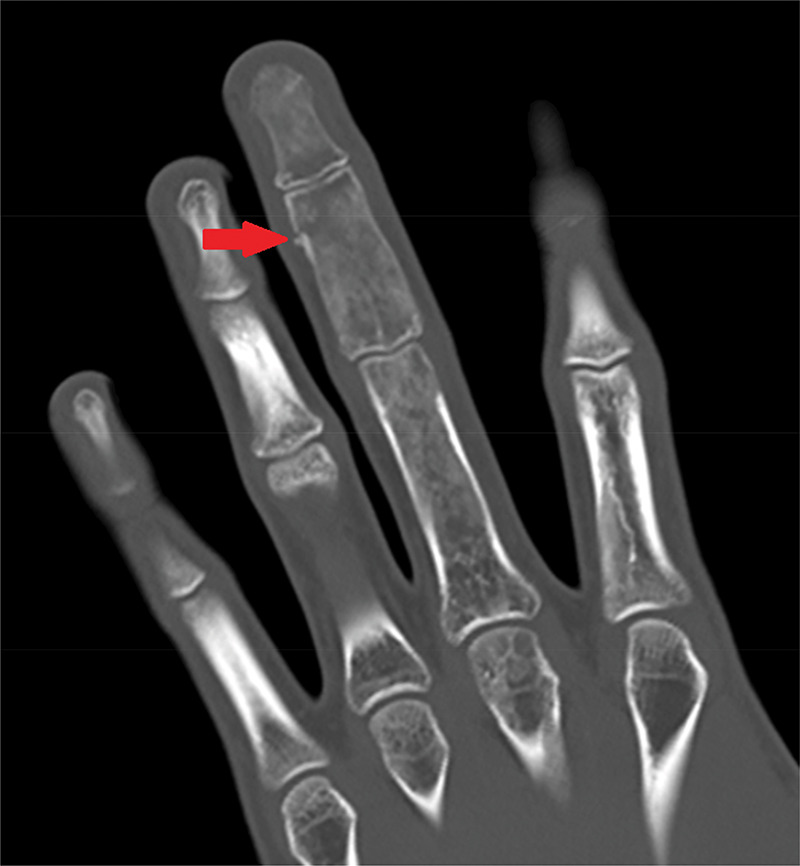 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Sarcoma Diagnosis and Treatment · Oral and Maxillofacial Pathology
Case
A 16-year-old male patient presented to the emergency department after injuring his left middle finger while playing basketball. X-ray showed a fracture of the middle phalanx and an aberrant expansile aspect of all phalanges of the middle finger (Figure 1). On MRI, multiple T2-hyperintense (Figure 2A), T1-hypointense (Figure 2B) and enhancing lesions (Figure 2C) were seen in the phalanges and metacarpal head, causing an expansion of the trabecular bone and thinning of the cortical bone. On CT, the lesions contained multiple ground-glass densities, and the cortical fracture in the middle phalanx was visible (Figure 3). Given the fact that the patient was known to have a history of a pathological femoral fracture caused by an aneurysmal bone cyst secondary to fibrous dysplasia (FD), the diagnosis of polyostotic FD with a pathologic fracture of the middle phalanx of the middle finger was made.
Anteroposterior X-ray of the left hand showing an expansile lesion involving all phalanges of the middle finger and a visible fracture line in the middle phalanx.
MRI of the left hand demonstrating multiple T2-hyperintense (A), T1-hypointense (B), and enhancing (C) lesions involving the phalanges and metacarpal head, leading to trabecular expansion and cortical thinning.
CT scan of the left hand showing multiple ground-glass bone lesions and a cortical fracture of the middle phalanx.
Comments
FD is a benign bone disease in which an abnormal differentiation of osteoblasts occurs, leading to the replacement of normal bone marrow and trabecular bone by fibrous stroma and immature bone. FD can either be monostotic (80%) or polyostotic (20%). Usually FD is found incidentally, but complications like a pathologic fracture, aneurysmal bone cysts or malignant degeneration can occur. FD can be one of the characteristics of McCune–Albright syndrome or Mazabraud syndrome.
Monostotic FD (MFD) is most often observed in the ribs, tibia, femur, humerus, mandible and skull. Asymptomatic MFD usually does not cause significant deformity, and most often does not convert to the polyostotic form. MFD usually becomes inactive during puberty.
The polyostotic variant (PFD) is most commonly seen in the skull, facial bones, pelvis and spine. It is often unilateral and is often limited to one limb. PFD is more often associated with fractures and deformations. Similarly to MFD, it usually does not proliferate and becomes inactive around puberty.
According to Fitzpatrick et al. [1], FD appears as intramedullary expensile lesions on medical imaging. A smooth cortical contour is always present, but endosteal scalloping can occur. The lesions appear hazy with ground-glass opacities, but can also be completely radiolucent or sclerotic. On MRI, FD typically shows an intermediate to low intensity on T1-weighted images and intermediate to high intensity on T2-weighted images with heterogeneous enhancement after gadolinium administration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.