Pyogenic Spondylitis Due to Erysipelothrix rhusiopathiae Infection: A Case Report
Yusuke Oshita, Takeshi Eguro, Satoshi Kimura, Keikichi Kawasaki, Yoshifumi Kudo

TL;DR
An 82-year-old man developed rare spinal infection from Erysipelothrix rhusiopathiae, likely due to unsanitary living conditions rather than animal contact.
Contribution
Reports a rare case of E. rhusiopathiae-induced spondylitis without traditional zoonotic exposure.
Findings
E. rhusiopathiae was identified as the cause of spondylitis through blood culture.
The patient's infection was linked to unsanitary living conditions rather than livestock contact.
Spinal surgery and ampicillin treatment led to significant improvement and no recurrence.
Abstract
The incidence of pyogenic spondylitis is growing worldwide, but that caused by zoonotic bacteria is not well-reported. Erysipelothrix rhusiopathiae infections of the spine are rare. We report a case of spondylitis caused by E. rhusiopathiae in a patient without a history of livestock industry work. An 82-year-old retired Japanese man experienced vomiting, loss of consciousness, and incontinence during dinner. Subsequently, an ambulance was dispatched, and he was transferred to a local general hospital. Upon admission, brain computed tomography and magnetic resonance imaging revealed no abnormalities, and echocardiography ruled out infective endocarditis. The patient presented with a fever of unknown origin and received piperacillin/tazobactam. Seven days later, a blood culture test identified E. rhusiopathiae, leading to a diagnosis of bacteremia caused by this organism. The treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
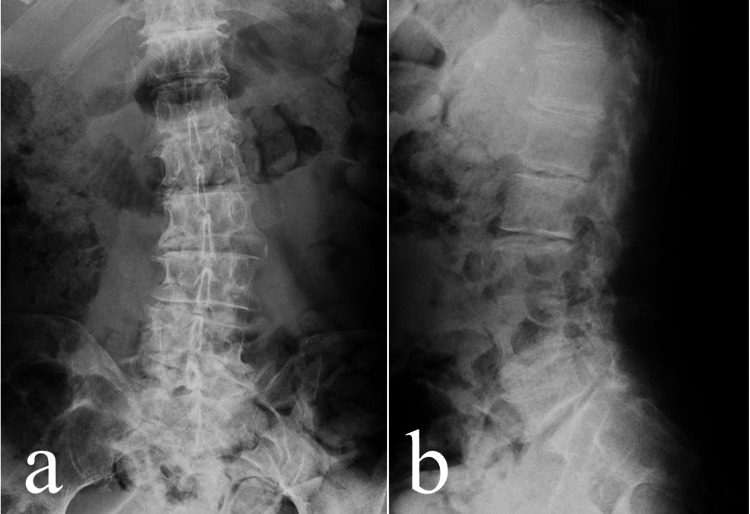 Figure 1
Figure 1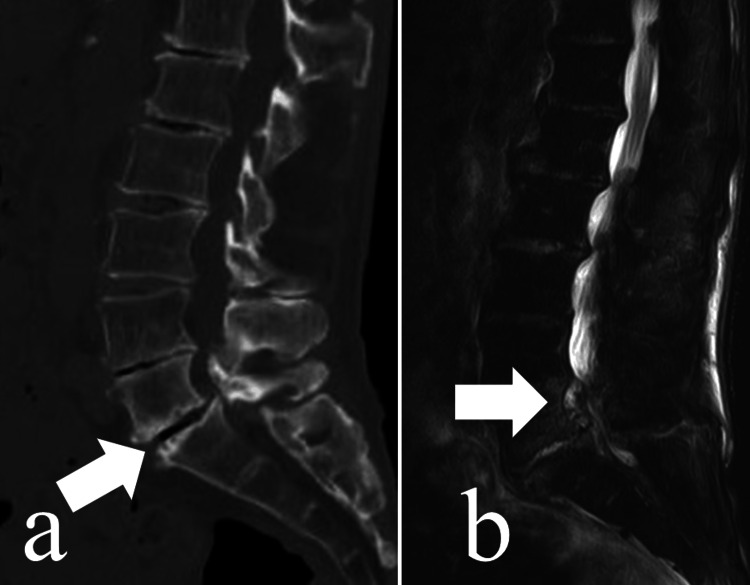 Figure 2
Figure 2| Time Period | Event Description | Antimicrobials |
| Six days before | Sciatic nerve pain developed | |
| Day 0 | Loss of consciousness: Fever of unknown origin | PIPC/TAZ |
| Day 7 | Enhanced lumbar MRI: Diagnosed pyogenic spondylitis | ABPC |
| Day 12 | Transferred from a general hospital to a university hospital | ABPC/SBT |
| Day 13 | Spinal surgery | |
| Day 24 | Resolution of inflammation | Oral CLDM |
| Day 34 | Transferred from the university hospital to a rehabilitation hospital | |
| Day 106 | Discharge to home | |
| Day 117 | Outpatient follow-up: No symptoms | Terminate antimicrobials |
| Day 138 | Lumbar MRI: No evidence of recurrence | |
| Day 481 | Final check-up at this point: No symptoms |
| Age | Sex | Occupation | |
| 58 | Male | Fisherman | 2008 Yamamoto et al. [ |
| 67 | Male | Fisherman | 2011 Haradaet al.[ |
| 42 | Female | Voluntary worker | 2013 Miura et al. [ |
| Age | Sex | Occupation | Risk | Infection Site | Treatment | |
| 67 | Female | Not specified | Alcoholic/injection drug use | L3 osteomyelitis | Antibiotics | 2001 Romneyet al. [ |
| 62 | Male | Farmar | Diabetes mellitus | T5/6 epidural abscess | Surgical drainage | 2009 Andrychowski et al. [ |
| 62 | Male | Farmar | Diabetes mellitus | L2/3 epidural abscess | Surgical drainage | 2014 Upapan et al |
| 48 | Male | Not specified | Puncture injury to his left index finger from the barb of a sea fish | L5/S osteomyelitis | Antibiotics | 2018 Lorenz et al. [ |
| 71 | Male | Homeless | Diabetes mellitus, chronic obstructive pulmonary disorder (COPD), chronic leukocytosis, and dirty daily life | Th6/7 | Drainage | 2022 Narvaezet al. [ |
| 82 | Male | Retired | Dirty daily life/Diabetes mellitus | L5/S Pyogenic spondylitis subdural abscess | Surgical drainage | 2025 Our case |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Infectious Diseases and Tuberculosis · Orthopedic Infections and Treatments
Introduction
The number of older and nutritionally compromised patients has been increasing, increasing the number of cases of bacterial infections such as pyogenic spondylitis [1-3]. The increasing incidence has been attributed to multiple factors, including chronic diseases and invasive spinal procedures [1], the aging population [2], and immunocompromising conditions [3]. In Japan, the annual incidence rate of pyogenic spondylodiscitis has been reported to range between 2 and 7 per 100,000 population [4].
The predominant causative organisms of pyogenic spondylitis are Gram-positive cocci, particularly Staphylococcus aureus [1,3], followed by Streptococcus, Enterococcus species [3], and Gram-negative bacilli such as Escherichia coli, Klebsiella, and Pseudomonas aeruginosa [3]. In contrast, infections caused by Erysipelothrix rhusiopathiae, a zoonotic, rod-shaped, Gram-positive bacterium, are rarely reported. Only a few cases have been published worldwide [5-9].
E. rhusiopathiae is of particular interest because it is a zoonotic bacterial infection, transmitted from animals to humans, yet spinal involvement has rarely been reported. In general, zoonotic bacterial infections have been reported in livestock workers and farmers. In this study, we report a case of spondylitis caused by* E. rhusiopathiae*, in which the patient had no history of employment in such occupations and no experience keeping pets, indicating an absence of direct animal contact. However, based on the work history of a woodcraft artisan, this patient resided in a home littered with garbage, with no apparent cleanup efforts. Although the route of infection was unclear, we encountered a case in which E. rhusiopathiae bacteremia led to the development of spondylitis. Thus, we assume that unsanitary living conditions might be a risk factor for such infections.
We herein report a rare case of pyogenic spondylitis caused by E. rhusiopathiae, underscoring the critical role of matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) in the rapid diagnosis of uncommon bacterial pathogens.
Case presentation
An 82-year-old retired Japanese man (height, 167 cm; weight, 53.2 kg) experienced sudden vomiting, loss of consciousness, and incontinence during dinner. The patient was then transported by ambulance to a local general hospital. Six days earlier, he had experienced pain in the left sciatic nerve. Radiographic examination at the initial visit showed age-related degenerative changes (Figure 1).
Radiographic image at the first hospital visita. Anterior-to-posterior view; b. Lateral view Radiographs demonstrated only age-related changes without any abnormal findings
The patient had comorbidities, including diabetes mellitus, hypertension, asbestos lung, and bipolar head arthroplasty of the right hip joint following a femoral neck fracture. No dental cavities or full dentures were found. The body temperature was 37.8 °C. Brain computed tomography (CT) and magnetic resonance imaging (MRI) showed negative findings. Laboratory data revealed a white blood cell (WBC) count of 7,800/μL (reference range: 3,300-8,600/μL; neutrophils, 89.3% (42.4-75.0%); lymphocytes, 3.8% (16.5-49.5%); eosinophils, 0.4% (0.0-8.5%); basophils, 0.1% (0.0-2.5%); monocytes, 6.4% (2.0-10.0%)), C-reactive protein (CRP) level of 10.85 mg/dL (reference range: <0.14 mg/dL), and glycated hemoglobin (HbA1c) of 7.9% (reference range: 4.6-6.2%). Urinary tract infection and COVID-19 infection were ruled out. Echocardiography revealed no evidence of infective endocarditis. Whole-body CT did not reveal the source of the fever.
The patient was diagnosed with a fever of unknown origin and was treated with piperacillin/tazobactam (PIPC/TAZ). The next day, the fever spiked to 40.0 °C, and the vital signs were: P 93/min, BP 134/43 mmHg, RR 16/min, SpO₂ 97%. After three days’ admission, the body temperature decreased to 37.8 °C, with a CRP level of 23.53 mg/dL and a WBC count of 10,400/μL (neutrophils, 89.3%; lymphocytes, 5.0%; eosinophils, 0.1%; basophils, 0.2%; monocytes, 6.4%). Gram-positive rods were detected after seven days of blood culture.
Using a mass spectrometry technique, especially the MALDI-TOF mass spectrometry system, by Bruker Daltonics (Yokohama, Japan) with the Biotyper software, version 3.1 (Bruker Daltonics), the isolate was identified as E. rhusiopathiae. Antimicrobial susceptibility testing showed that the isolate was susceptible to PCG (penicillin G), ABPC (ampicillin), MINO (minocycline), CEZ (cefazolin), CTM (cefotiam), SBT/CPZ (sulbactam/cefoperazone), FMOX (flomoxef), EM (erythromycin), CLDM (clindamycin), FOM (Fosfomycin), CPFX (ciprofloxacin), LVFX (levofloxacin), CFPM (cefepime), and MEPM (meropenem), but resistant to GM (gentamicin) and VCM (vancomycin). According to the results of susceptibility testing, the antibiotic was changed to ABPC. Lower back pain was observed during treatment. Although radiography showed almost normal findings, CT of the lumbar spine was performed and revealed a lytic lesion at the L4/5-disc level. For further evaluation of this lesion, enhanced MRI was subsequently performed, which demonstrated discitis and epidural abscesses (Figure 2).
Preoperative CT and MRI imagesa. CT before surgery. Lytic lesions were detected in the L4/5 intervertebral disc (white arrow).b. MRI before surgery. An abscess was detected at L4/5 (white arrow).
After being diagnosed with spondylitis, the patient was transferred to a university hospital. The day of the transfer, a board-certified dermatologist conducted a thorough skin examination and confirmed the absence of any skin infection, such as scabies, ticks, or lice. The day after the transfer, L4/5/S1 laminoplasty surgery was performed. During the surgery, a subdural abscess compressing the dura mater of the nerve root was removed. Postoperatively, the pain decreased. Seven days after surgery, the inflammatory parameters improved: CRP levels decreased to 0.79 mg/dL and WBC count to 3,470/μL (neutrophils, 69.1%; lymphocytes, 20.5%; eosinophils, 3.7%; basophils, 1.2%; monocytes, 5.5%), with no symptoms of infection. On hospital day 24, after resolution of inflammation, the intravenous ampicillin/sulbactam (ABPC/SBT) was switched to oral clindamycin (CLDM) 450 mg/day. The patient did not experience spinal complications such as palsy or dysuria. Twenty days after the surgery, the patient was transferred to a rehabilitation hospital. Ninety-two days after surgery, the patient was discharged and could walk unaided. During hospitalization, the family hired a cleanup company to maintain cleanliness at the patient’s home.
On postoperative day 125, MRI revealed no abscesses. CT imaging showed a trend toward union. At 195 days post-surgery, radiography indicated slight disc height narrowing, yet the patient remained asymptomatic. Five months post-surgery, no typical changes were observed. One year and six months post-surgery, there were no symptoms of pyogenic spondylitis recurrence.
The overall clinical course of this case, including clinical events, antibiotic administration, diagnostic procedures, and outcomes, is summarized in Table 1. This case underscores the clinical significance of recognizing the progression from fever of unknown origin to bacteremia, identification of E. rhusiopathiae, and subsequent spinal infection, which may facilitate earlier diagnosis and management in similar cases.
Discussion
Recent studies from South Korea and Germany have shown an increasing incidence of pyogenic spondylitis [1-3]. Reported rates range from 5.4 per 100,000 in Germany in 2005 to 11.0 per 100,000 in 2019, representing a two-fold increase [2], and from 22.9 to 35.8 per 100,000 in South Korea between 2010 and 2019, representing a 1.5-fold increase [1].
Rostamian et al. reviewed 62 case reports of E. rhusiopathiae infection [5]. The review describes only four cases from Japan, of which three were infective endocarditis. Of these three patients, two were fishermen [10,11] and one was a voluntary worker in a school for handicapped children [12] (Table 2). The remaining case was a soft tissue infection of the right hand caused by a cat bite [13].
Romney et al. reported that* E. rhusiopathiae* is sensitive to penicillin and carbapenem but resistant to vancomycin [14]. In this case, although the isolate was susceptible to ABPC, the regimen was switched to intravenous ampicillin/sulbactam (ABPC/SBT) after transferring due to the hospital formulary policy, and oral CLDM was added based on the results of antimicrobial susceptibility testing.
The patient had no history of animal contact other than exposure to rats and had not been bitten. Hypertension and diabetes were the underlying comorbidities. According to the patient, he had not changed his bed linen in these years; he deduced that brown rats might have settled in his room, and he saw cockroaches daily. Moreover, the patient bathed once a week with reused water. Narvaez et al. also report a homeless spondylosis case without any exposure to any animal contact [6]. Thus, we assume that sanitation is important to prevent this infection. A review reported that 21 out of 62 cases (34%) presented with skin lesions and 23 cases (37.1%) with heart valve infections [5]. However, the present case exhibited neither skin lesions nor infective endocarditis.
In general, some reports state that pyogenic spondylitis can arise from dental cavities [15,16], but no dental cavities were identified in this case. In contrast to the typical cause of pyogenic spondylitis, the fact that E. rhusiopathiae is not part of the oral flora might have an impact. Interestingly, the other reports of E. rhusiopathiae infection cases do not discuss the oral infections [5,7-13]. A few case reports have described spinal infections caused by* E. rhusiopathiae* (Table 3).
Notably, Upapan et al. reported a case of a psoas abscess with E. rhusiopathiae without endocarditis [7], which was treated with surgical drainage. Moreover, Andrychowski et al. reported thoracic spondylitis caused by E. rhusiopathiae [8], in which the abscess was drained. In our case, the epidural abscess caused sciatic nerve pain, drainage, and nerve root decompression. Importantly, symptoms of lower back and sciatic nerve pain disappeared immediately after spinal surgery. In this case, we assumed that surgical drainage with nerve root decompression. Systematic reviews of pyogenic spondylitis have also reported that prompt surgical intervention is crucial for the avoidance of lumbar complaints after surgery [17].
Until recently, E. rhusiopathiae infections have not been frequently reported. As we report in this paper, MALDI-TOF testing will enable us to identify these zoological microorganisms more easily.
Conclusions
We successfully treated a patient with spondylitis secondary to bacteremia caused by E. rhusiopathiae. As far as we could ascertain, this is the first reported case of* E. rhusiopathiae*-induced spondylitis from Japan. Although limited to a single case, this report highlights that* E. rhusiopathiae* infection can pose a potential risk in compromised hosts and provides educational value for clinicians in recognizing and managing such severe infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence and treatment trends of infectious spondylodiscitis in South Korea: a nationwide population-based study P Lo S One Son HJ Kim M Kim DH Kang CN 018202310.1371/journal.pone.0287846 PMC 1030963037384614 · doi ↗ · pubmed ↗
- 2Epidemiological trends of pyogenic spondylodiscitis in Germany: an EANS Spine Section Study Sci Rep Kramer A Thavarajasingam SG Neuhoff J 202251320233798037110.1038/s 41598-023-47341-z PMC 10657388 · doi ↗ · pubmed ↗
- 3Epidemiology and management of infectious spondylitis in Korea: a narrative review Ewha Med J Park KH 047202410.12771/emj.2024.e 37PMC 1209358040703465 · doi ↗ · pubmed ↗
- 4Seasonal trends of pyogenic spondylodiscitis in Japan: a nationwide inpatient database study Int J Infect Dis Motoyoshi T Ogawa T Fukushima K Kutsuna S Schermann H Fushimi K Yoshii T 10776715320253971663610.1016/j.ijid.2024.107767 · doi ↗ · pubmed ↗
- 5Clinical manifestations, associated diseases, diagnosis, and treatment of human infections caused by Erysipelothrix rhusiopathiae: a systematic review Germs Rostamian M Rahmati D Akya A 1631122022 https://pmc.ncbi.nlm.nih.gov/articles/PMC 9113682/3560194410.18683/germs.2022.1303 PMC 9113682 · doi ↗ · pubmed ↗
- 6Triple threat: a case of Erysipelothrix rhusiopathiae septicemia complicated by multi-valvular endocarditis, spinal osteomyelitis, and septic embolic stroke Cureus De Narvaez E Schoenfeld D Elshereye A Tran JD Oehler RL 014202210.7759/cureus.27789 PMC 945159736106220 · doi ↗ · pubmed ↗
- 7Erysipelothrix rhusiopathiae bacteremia without endocarditis associated with psoas abscess: the first case report in Thailand J Med Assoc Thai Upapan P Chayakulkeeree M 232236972014 https://www.thaiscience.info/journals/Article/JMAT/10905953.pdf 24772603 · pubmed ↗
- 8Empyema in spinal canal in thoracic region, abscesses in paravertebral space, spondylitis: in clinical course of zoonosis Erysipelothrix rhusiopathiae Eur Spine J Andrychowski J Jasielski P Netczuk T Czernicki Z 06321 Suppl 4201210.1007/s 00586-012-2289-9PMC 336904822526696 · doi ↗ · pubmed ↗