Long-Term Oncological Outcomes Following Anastomotic Leakage After Colorectal Cancer Surgery: A Retrospective Monocenter Trial
Mario Kaufmann, Julia Hardt, Christopher Bozinov, Lothar Pilz, Steffen Seyfried, Christoph Reissfelder, Georgi Vassilev, Georgi Kalev

TL;DR
This study examines how anastomotic leakage after colorectal cancer surgery affects long-term survival and cancer recurrence.
Contribution
The study provides new insights into the long-term oncological outcomes associated with anastomotic leakage in colorectal cancer patients.
Findings
Anastomotic leakage occurred in 11.1% of patients with risk factors including age ≤ 65 and mid-rectal tumor location.
Anastomotic leakage did not significantly affect overall survival but increased 90-day mortality.
There was no significant impact of anastomotic leakage on local or distant cancer recurrence.
Abstract
Background and objectives: Colorectal cancer (CRC) ranks among the most common cancers worldwide. One of the most severe postoperative complications is an anastomotic leakage (AL). The aim of this study was to investigate the impact of AL on the long-term oncologic outcome. Methods: All patients who underwent curative surgery for CRC at the Department of Surgery at the University Hospital in Mannheim between January 2011 and June 2016 were retrospectively analyzed. The primary endpoint was the overall survival (OS). Results: Between January 2011 and June 2016, a total of 504 patients were included in the study. The median follow-up was 42 months. We found an AL incidence of 11.1% (n = 56) with the following risk factors: age ≤ 65 (p = 0.03) and location of the tumor in the rectum, especially mid-rectum (p = 0.012). Patients with AL were less likely to have adjuvant chemotherapy (p =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
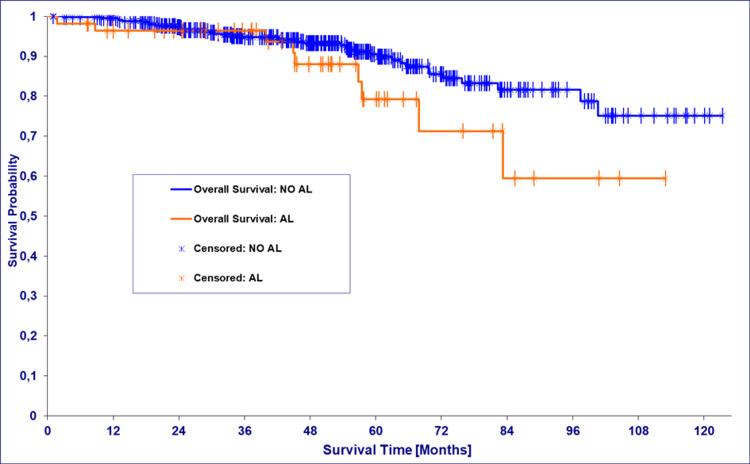 Figure 1
Figure 1| Abs. number (n = 504) | Percentage (%) | 95% CI | |
| Age (years) | |||
| ≤65 | 237 | 47.0 | 0.427-0.514 |
| >65 | 267 | 53.0 | 0.486-0.573 |
| Sex | |||
| Male | 305 | 60.5 | 0.562-0.647 |
| Female | 199 | 39.5 | 0.353-0.438 |
| Location of cancer | |||
| No information | 1 | 0.2 | <0.001-0.012 |
| Cecum | 55 | 10.9 | 0.085-0.140 |
| Ascending colon | 74 | 14.7 | 0.119-0.181 |
| Transverse colon | 28 | 5.6 | 0.038-0.079 |
| Descending colon | 12 | 2.4 | 0.013-0.042 |
| Sigmoid | 86 | 17.1 | 0.140-0.206 |
| Rectosigmoid | 1 | 0.2 | <0.001-0.012 |
| Upper rectum | 43 | 8.5 | 0.064-0.113 |
| Mid-rectum | 116 | 23.0 | 0.196-0.269 |
| Lower rectum | 71 | 14.1 | 0.113-0.174 |
| UICC stage | |||
| No information | 3 | 0.6 | 0.001-0.018 |
| I | 138 | 27.4 | 0.237-0.314 |
| II | 134 | 26.6 | 0.229-0.306 |
| III | 212 | 42.1 | 0.378-0.464 |
| IV | 17 | 3.4 | 0.021-0.054 |
| Molecular grading | |||
| Not applicable | 29 | 5.8 | 0.040-0.082 |
| G1 | 21 | 4.2 | 0.027-0.063 |
| G2 | 385 | 76.4 | 0.725-0.799 |
| G3 | 66 | 13.1 | 0.104-0.163 |
| G4 | 3 | 0.6 | 0.001-0.018 |
| Surgical approach | |||
| No information | 7 | 1.4 | 0.006-0.029 |
| Open | 218 | 43.3 | 0.390-0.476 |
| Laparoscopic | 276 | 54.8 | 0.504-0.591 |
| Robotic | 3 | 0.6 | 0.001-0.018 |
| Type of surgery | |||
| No information | 2 | 0.4 | 0.001-0.015 |
| Right hemicolectomy | 129 | 25.6 | 0.220-0.296 |
| Transverse colectomy | 7 | 1.4 | 0.006-0.029 |
| Left hemicolectomy | 26 | 5.2 | 0.035-0.075 |
| Sigmoid resection | 45 | 8.9 | 0.067-0.118 |
| Subtotal colectomy | 15 | 3.0 | 0.018-0.049 |
| Proctocolectomy | 15 | 3.0 | 0.018-0.049 |
| Anterior resection | 68 | 13.5 | 0.108-0.168 |
| Low anterior resection | 185 | 36.7 | 0.326-0.410 |
| Ultralow/intersphincteric resection | 12 | 2.4 | 0.013-0.042 |
| Radiotherapy | |||
| Neoadjuvant | 139 | 27.58 | 0.239-0.316 |
| Adjuvant | 7 | 1.39 | 0.006-0.029 |
| None | 358 | 71.03 | 0.669-0.748 |
| Leakage (-) (n = 445) | Leakage (+) (n = 56) | p | |||
| n (%) | 95% CI | n (%) | 95% CI | ||
| Age | |||||
| ≤65 | 202 (45.39) | 0.408-0.500 | 34 (60.71) | 0.476-0.724 | 0.030* |
| >65 | 243 (54.61) | 0.500-0.592 | 22 (39.29) | 0.276-0.524 | |
| UICC stage | |||||
| No information | 1 (0.22) | <0.001-0.014 | 0 (0.00) | - | 0.824* |
| I | 123 (27.64) | 0.237-0.320 | 14 (25.00) | 0.154-0.378 | |
| II | 121 (27.19) | 0.233-0.315 | 13 (23.21) | 0.680-0.888 | |
| III | 186 (41.80) | 0.373-0.464 | 26 (46.43) | 0.340-0.593 | |
| IV | 14 (3.15) | 0.018-0.053 | 3 (5.36) | 0.013-0.152 | |
| ASA class | |||||
| 0 | 4 (0.90) | 0.003-0.024 | 0 (0.00) | - | 0.458* |
| 1 | 107 (24.04) | 0.203-0.282 | 12 (26.79) | 0.126-0.340 | |
| 2 | 222 (49.89) | 0.453-0.545 | 30 (53.57) | 0.407-0.660 | |
| 3 | 106 (23.82) | 0.201-0.280 | 9 (16.07) | 0.085-0.280 | |
| 4 | 6 (1.35) | 0.006-0.029 | 2 (3.57) | 0.003-0.128 | |
| Location of cancer | |||||
| Cecum | 53 (11.91) | 0.092-0.153 | 1 (1.79) | <0.001-0.103 | 0.012* |
| Ascending colon | 69 (15.51) | 0.124-0.192 | 5 (8.93) | 0.035-0.197 | |
| Transverse colon | 27 (6.07) | 0.042-0.087 | 1 (1.79) | <0.001-0.103 | |
| Descending colon | 12 (2.70) | 0.015-0.047 | 0 (0.00) | - | |
| Sigmoid | 78 (17.53) | 0.143-0.214 | 8 (14.29) | 0.072-0.260 | |
| Rectosigmoid | 16 (3.60) | 0.022-0.058 | 2 (3.57) | 0.003-0.128 | |
| Upper rectum | 36 (8.09) | 0.059-0.110 | 7 (12.50) | 0.059-0.239 | |
| Mid-rectum | 93 (20.90) | 0.174-0.249 | 23 (41.07) | 0.292-0.541 | |
| Lower rectum | 61 (13.71) | 0.108-0.172 | 9 (16.07) | 0.085-0.280 | |
| Leakage (-) (n = 445) | Leakage (+) (n = 56) | p | |
| OS | |||
| Median | 60.3 | 45.2 | 0.090** |
| 95% CI | 53.7-72.4 | 39.9-83.2 | |
| Local recurrence | |||
| n (%) | 25 (5.6) | 1 (1.8) | 0.223* |
| 95% CI | 0.038-0.082 | <0.001-0.103 | |
| Distant recurrence | |||
| n (%) | 74 (16.6) | 11 (19.6) | 0.571* |
| 95% CI | 0.135-0.204 | 0.112-0.320 | |
| 30-day mortality | |||
| n (%) | 1 (0.2) | 1 (1.8) | 0.081* |
| 95% CI | <0.001-0.014 | <0.001-0.103 | |
| 90-day mortality | |||
| n (%) | 1 (0.2) | 2 (3.8) | 0.002* |
| 95% CI | <0.001-0.014 | 0.112-0.320 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Cardiac, Anesthesia and Surgical Outcomes · Colorectal and Anal Carcinomas
Introduction
Colorectal cancer (CRC) is one of the leading causes of cancer death worldwide. In the United States, it is the third most common cause of cancer-related death in both men and women. CRC is the second most common malignant tumor in women and the third most common in men in German-speaking countries. The average age of onset is 70-75 years. However, there has been an age shift in recent years: increasingly younger patients are developing CRC; one-fifth of patients are in their early 50s or even younger when they develop CRC [1].
Although the treatment of CRC-especially rectal cancer-is increasingly multimodal, surgical oncological resection remains the mainstay of curative therapy. Probably the most important and still the most feared complication after CRC surgery is anastomotic leakage (AL). AL is responsible for one-third of postoperative mortality after surgery for rectal cancer [2]. Accordingly, 30-day mortality has been shown to be significantly higher for patients with AL (8.8% vs. 2.5%) [3].
Studies have identified several risk factors for the occurrence of AL. It was shown that the localization of the anastomosis plays an important role: especially, low rectal anastomoses have a high risk of AL. Moreover, male gender and preoperative radiotherapy may increase the risk of AL [4]. Further independent predictors of AL are obesity, emergency surgery, absence of a diverting ileostomy, American Society of Anesthesiologists (ASA) score ≥ III, preoperative tumor complications, extensive additional (multivisceral) resection, and preoperative hypoalbuminemia indicating malnutrition [5,6].
However, despite standardized double-stapled anastomosis technique and perioperative measures to reduce patient risk factors (nutritional advice, patient blood management, prehabilitation programs, combined bowel preparation, etc.), AL remains a relevant complication that leads to further potentially severe secondary morbidity. In addition, AL could be associated with a poorer oncological long-term outcome for the affected patients [7]. The aim of this study was to determine whether AL is associated with overall survival (OS), recurrence rates, and postoperative mortality using a large monocentric cohort from a CRC center certified by the German Cancer Society and a center of excellence for coloproctology of the German Society for General and Visceral Surgery.
Materials and methods
Study design, location, and setting
This retrospective cohort study was designed in accordance with the Declaration of Helsinki. After approval (2020-844R) from the institutional ethics committee, the Ethics Committee II of the University of Heidelberg, Medical Faculty Mannheim, the study was conducted at the Department of Surgery at the University Hospital in Mannheim, Germany.
Patient recruitment
All patients who were at least 18 years old and underwent curative surgery for CRC between January 2011 and June 2016 were included in the analysis.
Inclusion and exclusion criteria
In order not to distort the survival statistics, patients who had never received curative treatment and were never tumor-free were excluded. On the other hand, patients in Union for International Cancer Control (UICC) stage IV were also included if they only had oligometastatic disease, i.e., if they could be treated curatively. Furthermore, all patients who did not undergo primary restoration of intestinal continuity by means of intestinal anastomosis-such as those who underwent Hartmann’s procedure or abdominoperineal resection-were excluded.
Definition of AL
AL was defined and graded according to the proposal by the International Study Group of Rectal Cancer [8]. Even if this classification was initially proposed for rectal cancer, it seems reasonable to adopt it also for AL occurring after resection for colon cancer. This pragmatic approach can also be found in comparable studies [9]. However, it must be taken into account that AL occurring after colon resection is usually not asymptomatic (grade A) and in most cases cannot be managed using non-surgical interventions (grade B, e.g., endoscopic vacuum therapy and CT-guided percutaneous drainage), but is very likely to require repeat surgery (grade C). Thus, after colon resection, a significantly higher proportion of grade C AL in the total number of AL cases is to be expected. In cases of clinical and/or laboratory suspicion of AL, a CT scan was initially performed in accordance with our internal hospital standards. In cases of rectal resection, a sigmoidoscopy was also performed if necessary.
Surgical procedures
All patients scheduled for elective oncological colorectal resection with primary anastomosis were eligible for inclusion in the study, regardless of the choice of surgical approach (laparoscopic, open, or robotic). The study cohort contains only very few robot-assisted procedures, as robotic surgery was only established at the Department of Surgery at the University Hospital in Mannheim in 2016. All resections included complete mesocolic excision (CME), partial mesocolic excision (PME), or total mesorectal excision (TME), depending on the tumor location in the colon and rectum. After colon resection, the bowel was reconstructed either intracorporeally as a side-to-side stapler anastomosis or extracorporeally as an end-to-end circular hand suture anastomosis. Reconstruction after rectal resection was routinely performed by creating a double-stapled side-to-end anastomosis using a 28 or 29 circular stapler. A protective ileostomy was generally performed in accordance with our hospital standard. The standard reconstruction technique after intersphincteric resection for ultralow rectal cancer patients was end-to-end handsewn coloanal anastomosis. All patients were monitored in accordance with the German guideline for CRC using regular CT scans, colonoscopies, clinical examinations, and carcinoembryonic antigen (CEA) measurements.
Study endpoints
The primary endpoint of the study was OS. The survival statistics were calculated as follows: OS refers to the patient's survival since the date of surgery. The end of the calculation period was the date on which the patient died, regardless of the underlying cause. Disease-free survival (DFS) is defined as a period of freedom from disease during which the patient survives without any symptoms of the tumor. This period begins with the date of surgery if it leads to tumor freedom and ends with the first date a disease recurrence (local or distant) is diagnosed or the last date of follow-up if no recurrence occurs. The secondary endpoints of the study were recurrence (including both local and distant recurrences) and 30- and 90-day mortality.
Statistical analysis
The patient characteristics were given in absolute numbers and percentages with the corresponding confidence intervals (CIs). The 95% CI was calculated using the modified Wald test.
Survival statistics were calculated using the Kaplan-Meier method. The log-rank test was used to compare the survival times of two groups. The calculation of the CIs of the survival statistics as a “function” of an AL was carried out using two different methods, described by Brookmeyer and Crowley and by Reid [10,11]. The K-sample test was used to test the homogeneity of the samples. The local and distant recurrence rates, 30- and 90-day mortality, and corresponding subgroup analyses were carried out using the chi-squared distribution test. For the plausibility checks of data, MS Excel (Microsoft Office LTSC Professional Plus 2021; Microsoft, Redmond, WA, US) was used. For the analysis of ordinal data and survival data, we used SAS University Edition Software, Version 9.4 (SAS Inc., Cary, NC, US). For the calculation of the CIs of proportions and ordinal data, GraphPad Prism was used, version 9.3 (GraphPad Software, Dotmatics, Boston, MA, US). Categorical variables are expressed as absolute frequencies and proportions (%); CIs are given using the Wald method and compared between two groups using the χ² tests. The odds ratio (OR), 95% CI, and p-value are calculated according to Altman using the 2 x 2 table of events/non-events in each of the groups. All significance tests were two-tailed with type I error set at α = 0.05.
Results
Between January 2011 and June 2016, a total of 504 patients underwent curative surgery for CRC with preservation of bowel continuity at the Department of Surgery at the University Hospital in Mannheim, Germany, and could therefore be included in the present study. The median age was 66 years, with an age range from 27 to 97 years. The study cohort consisted of 60.5% men, whereas women were in the minority with the remaining 39.5%. The most common tumor location was the mid-rectum with 23%. Overall, almost half of the tumors (45.6%) were in the rectum, whereby tumors of the rectosigmoid junction were not included here but were evaluated as colon carcinomas. Most diagnoses were made in UICC stage III with 42.1%, followed by UICC stage I with 27.4% and II with 26.6%. The majority of operations (54.8%) were performed conventionally laparoscopically, 43.3% of patients underwent open surgery, and only 0.6% underwent robot-assisted surgery. Further patient, tumor, and procedure characteristics can be found in Table 1.
AL and associated factors
Of the 504 patients in the study cohort, 56 patients suffered AL (11.1%). Grade B AL was the most common AL type (4.8%). Grade C AL was similarly common (4.2%). Grade A AL was the least frequently diagnosed (1.8%). To determine the risk factors associated with AL in this study cohort, subgroup analyses were carried out (Table 2). The comparison of the cohorts with and without AL showed that most patients with AL (60.7%) were significantly younger, i.e., under 65 years of age. In contrast, 54.6% of the cohort of patients without AL were over 65 years old (p = 0.030). Furthermore, the occurrence of AL was found to be significantly dependent on the tumor location. AL occurred most frequently after resection of tumors of the mid-rectum (41.1%). In general, AL occurred more frequently after resection of rectal carcinoma than after colon carcinoma resection (69.6%, p = 0.012). Even though the proportion of patients with UICC stages III and IV or with ASA class IV was higher in the cohort with AL, UICC stage and ASA class were not significantly associated with the development of AL.
Primary outcomes
Initially, the survival probability of patients with AL is only slightly worse. After about 3.5 years, however, there is a clear divergence of the two survival curves to the disadvantage of the cohort with AL (Figure 1). Patients with an AL had a median OS of 60.3 months (95% CI 53.7-72.4), and patients without an AL had a median OS of 45 months (95% CI 39.9-83.2) (Table 3).
Kaplan-Meier estimate: overall survival with or without anastomotic leakage (AL)
Secondary outcomes
The median follow-up regarding the oncological endpoints was 42 months (range 1-114). Sufficient data were available from 501 patients for the evaluation of recurrences in relation to the occurrence of AL. Local recurrences occurred in 5.4% of the patients (26/501). Distant recurrences were even more frequent, affecting 17.5% of the patients (85/501). Of the 56 patients with AL, one patient (1.8%) developed a local recurrence and 11 patients (19.6%) a distant recurrence. In contrast, 25 of the 445 patients without AL (5.6%) had a local recurrence, and 74 patients (16.6%) had a distant recurrence. There was no statistically significant difference regarding recurrence rates between the AL and non-AL cohorts (local recurrence: p = 0.223; distant recurrence: p = 0.571). Furthermore, we assessed both 30- and 90-day postoperative mortality. One patient died in each of the two cohorts with and without AL within 30 days after surgery (AL: 1/56 (1.8%) vs. non-AL: 1/445 (0.2%); p = 0.081). Two patients with AL died within 90 days of surgery (3.8%), whereas there was no further death in the non-AL cohort between postoperative days 30 and 90. Thus, significantly more patients died within 90 days if AL had occurred (p = 0.002).
Discussion
This single-center retrospective cohort study investigated the factors associated with AL and the influence of AL on the oncological outcome of patients with CRC after curative surgery at a certified center of excellence for CRC surgery. A total of 504 patients were included in the study. The AL incidence of 11.1% (n = 56) is comparable to similar studies [12,13]. Hasegawa et al. described in a retrospective cohort (n = 395) an incidence of 12.7% for rectal cancer patients with UICC classes I-III [13]. The analyses of the Netherlands Cancer Register (n = 65,299 colon cancer; n = 22,855 rectal cancer) by Arron et al. showed an AL incidence of 4.8% (n = 3,136) and 7.9% (n = 1,814) for colon and rectal cancers, respectively [12].
Our study revealed that patients with AL were significantly younger (<65 years), and the localization of the tumor also played a decisive role. Patients with a tumor in the mid-rectum had a significantly higher AL rate than patients with colon cancer. The results regarding age are controversial in the literature: While Stormark et al. (n = 22,985 colon cancer) showed a higher risk of AL in older patients (>79 years), Arron et al. described a higher risk in younger patients (<70 years) [9,12]. A smaller analysis by Hasegawa et al. (n = 395) showed no differences regarding the impact of patient age on the risk of AL. An extensive resection of locally advanced tumors can potentially be associated with an increased risk for AL. The evidence regarding the localization of the tumor as a risk factor for AL is also heterogeneous, whereby the different classifications should be noted here in particular. When considering colon carcinoma alone, tumors distal to the right flexure or transverse resections and subtotal colectomies appear to be particularly at risk of AL [9,12].
It was shown in this study, comparable to the literature, that patients with AL were significantly less likely to receive planned adjuvant chemotherapy [12]. Patients with a non-complicated postoperative course could reach a faster return to intended oncologic treatment (RIOT). Postoperative complications in oncologic liver and gastric surgery are risk factors for an inability to RIOT, which in turn is correlated with a shortness of OS [14,15].
The median OS was 45.2 months in the AL group compared to 60.3 months in the non-AL group, presumably reflecting the significantly higher proportion of patients over 65 years of age in the non-AL group. There was no statistically significant impact of the occurrence of an AL on OS. However, there was a divergence of the Kaplan-Meier curves after 3.5 years in favor of the patients who did not develop AL. Significant effects for this parameter were shown in meta-analyses [16,17]. Regarding five-year relative survival, large registry analyses showed a significant disadvantage for patients with AL in the entire cohort [9]. It is to be expected that we would also have seen this effect with a larger number of cases. The subgroup analyses according to the UICC classification and tumor location showed that colon cancer patients in UICC stage III and rectal cancer patients in UICC stages III and IV had a lower survival rate after AL [9,12].
Our study could not identify AL as a significant risk factor for local and distant tumor recurrence. This is in part in contrast with meta-analyses that showed a significant increase in local recurrence but not in distant recurrence after AL [16,17]. Generally, no local tumor cell contamination is to be expected after R0 resection in the case of AL. In patients who suffer AL after resection of a locally advanced CRC potentially preceded by neoadjuvant radiotherapy or radiochemotherapy (rectal cancer), indicated adjuvant chemotherapy is often delayed or not administered at all. This may be a possible explanation for the correlation between AL and local recurrence in patients treated according to the traditional treatment paradigms. Future studies will show whether the application of complete chemotherapy prior to surgery in the sense of total neoadjuvant therapy (TNT) would limit the impact of AL on the recurrence rate in rectal cancer patients.
Another common theory is that AL leads to localized inflammation and is, therefore, potentially more likely to result in recurrence, as the local immune competence that fights the inflammation is at least partially reduced [18]. Regarding 30- and 90-day mortality rates, the 90-day mortality rate was significantly higher after the occurrence of AL. Although a significant difference was found (p = 0.002), only a few patients died within the first 90 days after surgery: two patients (3.8%) in the AL group vs. one patient (0.2%) in the non-AL group.
Future studies must take a closer look at the pathophysiological effects of AL, preventive measures, early detection, and treatment methods. The identification of patients at risk is the decisive factor in preventing AL through closer monitoring. If AL and its secondary complications can be successfully prevented, more patients will be able to continue their intended oncological therapy, which could be associated with an improvement in prognosis.
Limitations
The retrospective design and its relatively small number of cases, which results in insufficient statistical power, limit the study. While the T4 stage and the presence of lymph node metastases, as known risk factors for local recurrence, were assessed by recording the UICC stage, data on other risk factors such as R0 status and, in patients with rectal cancer, a positive circumferential margin or extramural venous invasion were not collected [16,19-21]. It was, therefore, not possible to compare the groups with and without AL regarding these risk factors, which represents a potential source of bias. Similar to some other authors, we analyzed the OS and the rate of local and distant recurrence as measures of long-term outcome, but we did not evaluate disease-free and cancer-specific survival since the data required to calculate these parameters were not available [22-24]. Furthermore, this study examined data collected between January 2011 and June 2016, so the impact of more recently proposed treatment strategies such as immunotherapy or TNT in patients with rectal cancer was not evaluated. In this cohort study, AL did not significantly affect OS or recurrence, but further prospective studies with multivariable adjustment are needed.
Conclusions
The occurrence of AL continues to be a serious complication in the postoperative course after colorectal surgery. In our study cohort, young patients and patients with tumors located in the mid-rectum were particularly frequently affected. AL had a significant impact on 90-day mortality. However, the occurrence of AL did not significantly influence the OS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Colorectal cancer statistics, 2023 CA Cancer J Clin Siegel RL Wagle NS Cercek A Smith RA Jemal A 2332547320233685657910.3322/caac.21772 · doi ↗ · pubmed ↗
- 2Meta-analysis of the risk for anastomotic leakage, the postoperative mortality caused by leakage in relation to the overall postoperative mortality Eur J Surg Oncol Snijders HS Wouters MW van Leersum NJ 101310193820122295452510.1016/j.ejso.2012.07.111 · doi ↗ · pubmed ↗
- 3Oncologic outcome and recurrence rate following anastomotic leakage after curative resection for colorectal cancer Surg Oncol Ramphal W Boeding JR Gobardhan PD Rutten HJ de Winter LJ Crolla RM Schreinemakers JM 7307362720183044950010.1016/j.suronc.2018.10.003 · doi ↗ · pubmed ↗
- 4Preoperative risk factors for anastomotic leakage after resection for colorectal cancer: a systematic review and meta-analysis Colorectal Dis Pommergaard HC Gessler B Burcharth J Angenete E Haglind E Rosenberg J 6626711620142465578410.1111/codi.12618 · doi ↗ · pubmed ↗
- 5Different risk factors for early and late colorectal anastomotic leakage in a nationwide audit Dis Colon Rectum Sparreboom CL van Groningen JT Lingsma HF 125812666120183023939510.1097/DCR.0000000000001202 · doi ↗ · pubmed ↗
- 6Preoperative hypoalbuminemia is an independent risk factor for increased high-grade morbidity after elective rectal cancer resection Int J Colorectal Dis Hardt J Pilz L Magdeburg J Kienle P Post S Magdeburg R 143914463220172882306410.1007/s 00384-017-2884-7 · doi ↗ · pubmed ↗
- 7Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis Ann Surg Mirnezami A Mirnezami R Chandrakumaran K Sasapu K Sagar P Finan P 89089925320112139401310.1097/SLA.0b 013e 3182128929 · doi ↗ · pubmed ↗
- 8Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer Surgery Rahbari NN Weitz J Hohenberger W 33935114720102000445010.1016/j.surg.2009.10.012 · doi ↗ · pubmed ↗