Red blood cell transfusion practice and cardiac comorbidities in patients with myelodysplastic syndromes
Allison Mo, Erica M. Wood, Jake Shortt, Zoe K. McQuilten

TL;DR
This study examines red blood cell transfusion practices and heart conditions in patients with myelodysplastic syndromes in a large Australian hospital network.
Contribution
The study provides real-world insights into transfusion practices and cardiac comorbidities in MDS patients.
Findings
57% of MDS patients received RBC transfusions, with transfused patients having lower hemoglobin and higher cardiac disease rates.
Restrictive transfusion strategies were common despite many patients having heart conditions.
Further research is needed to determine optimal transfusion strategies for MDS patients with cardiac comorbidities.
Abstract
Evidence guiding optimal transfusion practice for patients with myelodysplastic syndromes (MDS) is lacking. Many patients have concurrent cardiac disease. Data on practice are sparse. We aimed to describe the use of red blood cell (RBC) transfusion and the prevalence of cardiac comorbidities in patients with MDS within Australia's largest public hospital network to better understand real‐world practices and outcomes. We conducted a retrospective cohort study of patients aged ≥18 years with MDS, MDS/myeloproliferative overlap neoplasm or chronic myelomonocytic leukemia admitted from 2016 to 2018 to determine RBC transfusion‐related endpoints. One hundred and seventy‐nine patients (median age 78 years, 61.5% male) were included, with a median follow‐up of 46 weeks. Of these, 102 (57.0%) received RBC transfusion. Transfused patients had lower presenting Hb (87 vs. 105 g/L, p < 0.0001),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
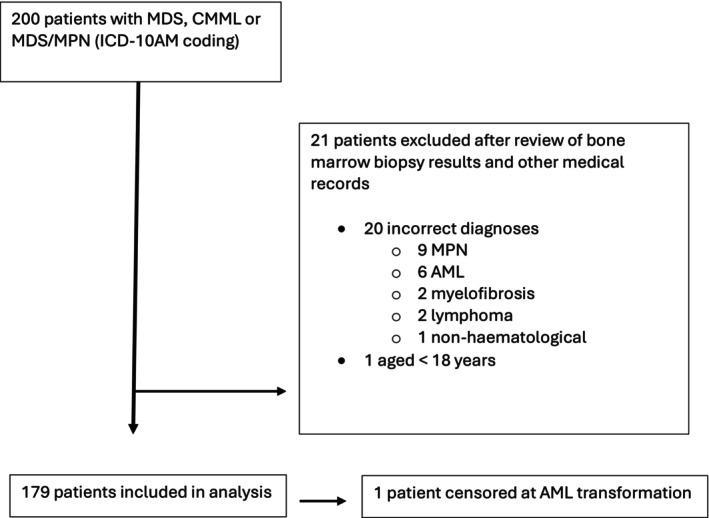 FIGURE 1
FIGURE 1| Characteristic | Entire cohort | Received RBC transfusion | No RBC transfusion |
|---|---|---|---|
| Age in years, median (IQR) | 78 (71–84) | 78 (73–84) | 78 (69–84) |
| Male | 110 (61.5%) | 67 (65.7%) | 43 (55.8%) |
| Female | 69 (38.5%) | 35 (34.3%) | 34 (44.2%) |
| Cardiac disease at any time during follow‐up, | 40 (22.3%) | 30 (29.4%) | 10 (12.9%) |
| Ischaemic heart disease | 31 (17.3%) | 25 (24.5%) | 6 (7.8%) |
| Cardiac failure | 36 (20.1%) | 26 (25.5%) | 10 (13.0%) |
| MDS classification, | |||
| MDS‐SLD | 1 (0.6%) | 1 (1.0%) | 0 |
| MDS‐RS‐SLD | 5 (2.8%) | 2 (2.0%) | 3 (3.9%) |
| MDS‐RS‐MLD | 13 (7.3%) | 6 (5.9%) | 7 (9.1%) |
| MDS‐MLD | 40 (22.3%) | 22 (21.6%) | 18 (23.4%) |
| MDS‐EB1 | 7 (3.9%) | 5 (4.9%) | 2 (2.6%) |
| MDS‐EB2 | 19 (10.6%) | 13 (12.8%) | 6 (7.8%) |
| del‐5q | 1 (0.6%) | 1 (1.0%) | 0 |
| CMML‐0 | 8 (4.5%) | 2 (2.0%) | 6 (7.8%) |
| CMML‐1 | 11 (6.2%) | 5 (4.9%) | 6 (7.8%) |
| CMML‐2 | 9 (5.0%) | 3 (2.9%) | 6 (7.8%) |
| Other MDS/MPN overlap | 12 (6.7%) | 10 (9.8%) | 2 (2.6%) |
| Therapy‐related MDS | 5 (2.8%) | 3 (2.9%) | 2 (2.6%) |
| Unknown (bone marrow biopsy not available) | 48 (26.8%) | 29 (28.4%) | 19 (24.7%) |
| IPSS‐R category, | |||
| Very low risk | 21 (11.7%) | 7 (6.9%) | 14 (18.2%) |
| Low | 50 (27.9%) | 28 (27.5%) | 22 (28.6%) |
| Intermediate | 15 (8.4%) | 10 (9.8%) | 5 (6.5%) |
| High | 9 (5.0%) | 6 (5.9%) | 3 (3.9%) |
| Very high | 9 (5.0%) | 7 (6.9%) | 2 (2.6%) |
| Unknown | 75 (41.9%) | 44 (43.1%) | 31 (40.0%) |
| Hemoglobin (g/L) at first admission, median (IQR) | 93 (83–108) | 87 (77–95) | 105 (95–117) |
| ESA, | 11 (6.2%) | 9 (8.8%) | 2 (2.6%) |
| Iron chelation, | 12 (6.7%) | 10 (9.8%) | 2 (2.6%) |
| Azacitidine, | 42 (23.5%) | 32 (31.4%) | 10 (13.0%) |
| Lenalidomide, | 1 (0.56%) | 1 (0.98%) | 0 |
| Number of outpatient day unit episodes, median (IQR) | 1 (0–3) | 2 (0–4) | 1 (0–1) |
| Number of inpatient hospital admissions, median (IQR) | 1 (0–2) | 1 (0–3) | 0 (0–1) |
| No of patients | 65 |
| Age, years, median (IQR) | 77 (72–82) |
| Sex, male, | 41 (63.1%) |
| Azacitidine use, | 23 (35.4%) |
| ESA use, | 6 (9.2%) |
| Total no. of outpatient RBC transfusion admissions | 388 |
| No. of outpatient RBC transfusion admissions per patient, median (IQR; range) | 3 (IQR 1–7; range 1–55) |
| No. of RBC units transfused (total) | 717 |
| No. RBC units transfused per episode, median (IQR; range) | 2 (IQR 1–2; range 1–4) |
| Interval (days) between transfusion episodes, median (IQR; range) | 14 (IQR 7–23; range 2–314) |
| Pre‐transfusion Hb (g/L) | 80 (IQR 74–86; range 28–105) |
| 24‐h post‐transfusion Hb increment (g/L), median (IQR; range) | +13 (IQR +2 to +21; range −2 to +48) |
- —National Health and Medical Research Council10.13039/501100000925
- —Monash University10.13039/501100001779
- —National Blood Authority10.13039/100015675
- —Haematology Society of Australia and New Zealand10.13039/501100003463
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Hemoglobinopathies and Related Disorders · Blood disorders and treatments
INTRODUCTION
1
Myelodysplastic syndromes (MDS) are hematological malignancies characterized by cytopenias and bone marrow failure, usually affecting the elderly. Management is largely supportive, as the only curative treatment, bone marrow transplantation (BMT), is unsuitable for many due to age and comorbidities. Anemia is common and associated with worse quality of life (QoL).1 Red blood cell (RBC) transfusion aims to improve patient symptoms. Although newer therapies such as erythropoiesis‐stimulating agents (ESAs) and erythroid maturation agents (EMAs)2 can improve MDS‐related anemia, these may not be available or suitable for all patients and are costly; thus, transfusion remains vital to management.
Chronic RBC transfusions may have complications, such as transfusion reactions, alloimmunization, and iron overload, and can be costly.3 Additionally, patients may find repeated blood tests and transfusions burdensome,4 contributing to the time toxicity of cancer treatments.5
The evidence base guiding RBC transfusion in MDS is sparse. Cochrane reviews of RBC transfusion hemoglobin (Hb) thresholds in different clinical settings6 and in patients with hematological malignancy treated with chemotherapy/radiotherapy7 were unable to make definitive conclusions for MDS patients. Although transfusion is given to improve QoL, systematic reviews have found no definitive evidence that a higher Hb transfusion strategy improves QoL,8, 9 though significant limitations were identified in included studies. This uncertainty is reflected in national10 and international guidelines,11 which are unable to recommend specific transfusion thresholds for chronically transfused outpatients, whereas restrictive strategies (Hb threshold <70–80 g/L) are recommended in acute settings.10, 11 Additionally, cardiac comorbidities are common in elderly patients but optimal transfusion strategies to reduce cardiac complications are unknown.6, 12
Despite the paucity of clear guidelines and data, in our 2017 Australasian MDS clinical practice survey, clinicians reported they would typically transfuse patients at Hb thresholds of <80 g/L^13^, consistent with a restrictive strategy. An international survey showed variability in Hb thresholds, with the commonest being <80 g/L.4 As these surveys are self‐reported, with the potential for responder bias or inaccuracies, we aimed to conduct a study of real‐world transfusion practice, to better understand practices, transfusion thresholds, transfusion burden, and cardiac comorbidity prevalence in patients with MDS.
METHODS
2
Study design and patient population
2.1
Following ethics approval (HREC reference RES‐17‐0000‐778Q), we conducted a retrospective cohort study of all patients aged ≥18 years with a diagnosis of MDS, chronic myelomonocytic leukemia (CMML), and other MDS/myeloproliferative overlap neoplasms (MDS/MPN) per World Health Organization (WHO) criteria14 admitted to the Monash Health hospital network in Melbourne, Australia, from August 1, 2016 to July 31, 2018. This time period was selected to coincide with the timing of our Australasian practice survey.13 Monash Health is a tertiary‐level public hospital network and includes five adult hospitals, serving approximately 25% of Melbourne's population, with >4 million patient annual admission episodes.
Patients were identified through hospital records. In Australia, all hospital diagnoses and procedures are recorded using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD‐10‐AM).15 We retrieved all admission records from Monash Health during the study period with ICD‐10‐AM codes for MDS, CMML, and MDS/MPN overlap (Table S1). The diagnosis was confirmed via patient medical records.
Data collection
2.2
All hospital admission episodes following the first diagnosis of MDS/CMML in our institution's records were extracted, including demographics, diagnoses, and RBC transfusion code (ICD‐10‐AM #1370602). This included both multi‐day “inpatient” hospitalizations and single‐day “outpatient” admissions in the hospital day unit.
Hb on the first day of hospital admission was recorded, for all included episodes.
ESAs, 5‐azacytidine (AZA; the only hypomethylating agent which was reimbursed under the Australian Pharmaceutical Benefits Scheme [PBS] during the time of the study), lenalidomide (PBS‐reimbursed for patients with deletion 5q MDS) and iron chelation prescriptions were obtained from pharmacy records. ESAs are not reimbursed under the PBS schedule for MDS in Australia. EMAs were not available during the study period outside a clinical trial.
Anemia management
2.3
Transfusions were administered at the discretion of treating clinicians. Hospital policies reference national guidelines, which do not specify a particular Hb threshold in this setting (due to lack of evidence).10 All RBC units issued by the national blood service (Australian Red Cross Lifeblood) are leucodepleted.
Definition of inpatient versus outpatient transfusion episodes
2.4
RBC transfusion may occur during an “outpatient” day unit episode, or as part of a multi‐day “inpatient” hospitalization admission. We particularly focused on outpatient episodes as these transfusions are typically planned in stable outpatients, whereas intercurrent illnesses (e.g., infection or bleeding) are more likely to affect transfusions for inpatients.
Definition of cardiac events and transfusion reactions
2.5
Cardiac events and transfusion reactions were identified by ICD‐10‐AM codes (Table S1). Ischemic cardiac disease included any diagnostic codes containing the terms myocardial infarction, angina, ischemic heart disease or coronary thrombosis. Cardiac failure diagnostic codes included the terms pulmonary edema, heart failure, ventricular failure, fluid overload, cardiogenic, shock or generalized/localized edema. This approach using ICD‐10‐AM codes only identifies events which require hospitalization, or occurring during hospitalization.
Statistical analysis
2.6
Statistical analyses were performed using Stata version 11.0 (Statacorp LP, College Station, Tex). Patients were censored at BMT or acute myeloid leukemia (AML) transformation (≥20% blasts), as these events are likely to affect transfusion requirements. Comparisons for significance of differences were performed using Chi‐square or Mann–Whitney tests, and p < 0.05 was considered statistically significant.
RESULTS
3
From August 1, 2016 to July 31, 2018, 200 patients were identified. After excluding 21 patients (20 for non‐MDS diagnoses and one patient aged <18 years; Figure 1), 179 patients with a total of 804 admission episodes were included. Fifty‐five patients died (30.7%). Nine patients (5.0%) were lost to follow‐up (defined as no contact with the health service for >12 months). Median follow‐up time was 32 weeks (IQR 12–55 weeks).
Consort diagram of study patient selection.
Patient characteristics
3.1
Table 1 shows clinical characteristics. Median age was 78 years (IQR 71–84); 110 (61.5%) were male. Forty patients (22.3%) had cardiac disease documented during follow‐up.
The commonest MDS subtype was MDS with multilineage dysplasia (n = 40, 22.3%). Forty‐eight patients (26.8%) had unknown classification due to unavailable bone marrow biopsy results (e.g., performed elsewhere). R‐IPSS risk categories16 were high to very high in 18 (10%) (Table 1).
The median Hb at first admission was 93 g/L (IQR 83‐108 g/L). Eleven patients (6.2%) received ESA, 12 patients (6.7%) received iron chelation therapy, and 42 (23.5%) received AZA during the study period. One patient (with del5q MDS) received lenalidomide. No patients received both ESA and AZA or lenalidomide.
One hundred and two patients (57.0%) received one or more RBC transfusions during the study period, during an inpatient admission or outpatient episode. Transfused patients had a median Hb of 87 g/L at first admission, compared to Hb 105 g/L for those who were not transfused (p < 0.0001). Of the 102 transfused patients, 21 (20.6%) became transfusion independent, defined as not requiring RBC transfusion for a minimum of 8 weeks17 maintained until the end of follow‐up.
Patients receiving outpatient RBC transfusion
3.2
Sixty‐five patients (36.3%) received outpatient RBC transfusion over 388 episodes, using a total of 717 RBC units. Table 2 shows outpatient transfusion characteristics. Twenty‐three patients (35.4%) received AZA and six (9.2%) received ESA; no patients received both. The median number of outpatient transfusion episodes per patient was three (IQR 1–7), with a median of two RBC units transfused per episode and 14 days between transfusions. The median pre‐transfusion Hb was 80 g/L (IQR 74–86 g/L), with a median 24‐h post‐transfusion Hb increment of +13 g/L.
Transfusion reactions
3.3
No transfusion reactions were recorded in the coding data during the study period.
Cardiac comorbidities prevalence and transfusion thresholds
3.4
Forty patients (22.3%) had cardiac disease at any time during the study period, either documented as a comorbid condition or a new diagnosis. There was no difference in pre‐transfusion Hb for patients with versus without any cardiac disease (median Hb 79 g/L vs. 81 g/L, p = 0.1), or when subdivided into those with ischemic cardiac disease (median Hb 81 g/L vs. 80 g/L, p = 0.7) or cardiac failure (81 g/L vs. 70 g/L, p = 0.12).
DISCUSSION
4
This study shows that patients with MDS frequently require RBC transfusion, and a restrictive transfusion threshold is common, with a median pre‐transfusion Hb of 80 g/L, in keeping with our13 and other surveys.4 Additionally, cardiac comorbidities are common, seen in nearly one‐quarter of patients.
Despite the high transfusion burden, with over one‐third of patients with MDS receiving outpatient RBC transfusion, there are limited clinical trial data on optimal transfusion strategies. Although not powered for clinical outcomes, the combined results of two pilot studies (n = 66) showed liberal transfusion thresholds improved QoL in selected domains, compared to restrictive thresholds.18, 19, 20 Another MDS transfusion threshold study was terminated early due to slow recruitment.21 One ongoing study is investigating whether maintaining a more stable Hb (rather than a specific threshold) with weekly transfusion also impacts patient outcomes.22
The high prevalence of cardiac comorbidities in patients with MDS, and potential impacts on transfusion outcomes, is also important. Chronic anemia in MDS may lead to cardiac dysfunction and remodeling due to pathophysiological adaptions.23 Cardiac iron overload also occurs in transfusion‐dependent MDS (17% in one study).24 There is the risk of transfusion‐associated circulatory overload (TACO) with each transfusion. However, optimal transfusion practice in patients with cardiac comorbidities remains uncertain.6 In the recent Myocardial Ischemia and Transfusion (MINT) trial in patients with acute MI and anemia, although a liberal transfusion strategy did not reduce the risk of recurrent MI or death at 30 days, it was consistently favored over a restrictive strategy in point estimates for death, cardiac death, recurrent MI, and hospital readmission, without safety concerns.25 Guidelines highlight ongoing uncertainty regarding the safety of restrictive thresholds in patients with ischemic cardiac disease.11, 26
No transfusion reactions were documented in our study, based on ICD‐10AM codes. This may be due to under‐recognition, under‐reporting, and/or reflect ICD‐10AM limitations as there are only five relevant codes (ABO incompatibility, Rh incompatibility, anaphylactic shock due to serum, other serum reaction, shock during or result from a procedure not otherwise specified; Table S1).
Limitations of our study include the retrospective design, the possibility of missing/incorrect diagnostic codes (e.g., incorrect code recorded for transfusion), lack of QoL data, and we could not capture complications occurring outside the hospital setting, though these are likely less severe. Additionally, ESAs and EMAs are not currently reimbursed in Australia for patients with MDS; hence, our findings may not be generalizable internationally. However, even in countries in which ESAs are widely available, transfusion rates in patients with MDS remain high.4
Strengths of the study include real‐world data which follows up on our clinician survey findings, and detailed laboratory data regarding transfusion thresholds and transfusion rates in MDS outpatients.
CONCLUSIONS
5
Patients with MDS are typically elderly, frequently have cardiac comorbidities, and are chronically anemic. Despite the lack of evidence supporting any particular transfusion strategy, restrictive transfusion strategies are commonly used, including in patients with cardiac disease. Given our findings and emerging evidence suggesting liberal transfusion may be preferred in patients with subtypes of cardiac disease, there is a need for research to investigate the optimal transfusion strategy in patients with MDS, particularly focusing on cardiac outcomes.
AUTHOR CONTRIBUTIONS
Allison Mo, Zoe K. McQuilten, Erica M. Wood, and Jake Shortt developed the study concept and design. Allison Mo performed the data collection. Allison Mo and Zoe K. McQuilten conducted the data analysis. All authors wrote and edited the manuscript.
FUNDING INFORMATION
Allison Mo receives PhD scholarship funding from the National Health and Medical Research Council (NHMRC), National Blood Authority, Monash University, and Haematology Society of Australia and New Zealand. Jake Shortt and Zoe K. McQuilten are supported by Australian NHMRC Emerging Leadership Fellowships (grant no. Zoe K. McQuilten: 1194811, Jake Shortt: 2009177). Erica M. Wood is supported by an NHMRC Leadership Fellowship (grant no. 1177784). Monash Health acknowledges the support of a donation from Dr. Alexander Baxter for its MDS research program.
CONFLICT OF INTEREST STATEMENT
Allison Mo does not have any conflict of interest to disclose for the submitted work. Jake Shortt has served on advisory boards for Pfizer, Bristol Myers Squibb, Otsuka, Mundipharma, and Novartis. Jake Shortt has received research funding from Astex Pharmaceuticals. Jake Shortt has received speaker's fees from Mundipharma and Novartis (all disclosures for Jake Shortt are outside of the submitted work). Erica M. Wood and Zoe K. McQuilten have received research funding to their institution from: Abbvie, Amgen, Antengene, AstraZeneca, Beigene, Bristol‐Myers Squibb, CSL Behring, Gilead, GSK, Janssen‐Cilag, Novartis, Pfizer, Roche, Sanofi, and Takeda, and research support from Sobi, all outside the submitted work.
Supporting information
TABLE S1. ICD‐10‐AM diagnostic codes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jansen AJ , Essink‐Bot ML , Beckers EA , Hop WC , Schipperus MR , van Rhenen DJ . Quality of life measurement in patients with transfusion‐dependent myelodysplastic syndromes. Br J Haematol. 2003;121:270–274.12694248 10.1046/j.1365-2141.2003.04272.x · doi ↗ · pubmed ↗
- 2Platzbecker U , Della Porta MG , Santini V , Zeidan AM , Komrokji RS , Shortt J , et al. Efficacy and safety of luspatercept versus epoetin alfa in erythropoiesis‐stimulating agent‐naive, transfusion‐dependent, lower‐risk myelodysplastic syndromes (COMMANDS): interim analysis of a phase 3, open‐label, randomised controlled trial. Lancet. 2023;402:373–385.37311468 10.1016/S 0140-6736(23)00874-7 · doi ↗ · pubmed ↗
- 3Gupta P , Le Roy SC , Luikart SD , Bateman A , Morrison VA . Long‐term blood product transfusion support for patients with myelodysplastic syndromes (MDS): cost analysis and complications. Leuk res. 1999;23:953–959.10573142 10.1016/s 0145-2126(99)00113-7 · doi ↗ · pubmed ↗
- 4Vijenthira A , Starkman R , Lin Y , Stanworth SJ , Bowen D , Harrison L , et al. Multi‐national survey of transfusion experiences and preferences of patients with myelodysplastic syndrome. Transfusion. 2022;62:1355–1364.35686926 10.1111/trf.16946 · doi ↗ · pubmed ↗
- 5Gupta A , Eisenhauer EA , Booth CM . The time toxicity of cancer treatment. J Clin Oncol. 2022;40:1611–1615.35235366 10.1200/JCO.21.02810 · doi ↗ · pubmed ↗
- 6Carson JL , Stanworth SJ , Dennis JA , Trivella M , Roubinian N , Fergusson DA , et al. Transfusion thresholds for guiding red blood cell transfusion. Cochrane Database Syst Rev. 2021: CD 002042.10.1002/14651858.CD 002042.pub 5PMC 869180834932836 · doi ↗ · pubmed ↗
- 7Radford M , Estcourt LJ , Sirotich E , Pitre T , Britto J , Watson M , et al. Restrictive versus liberal red blood cell transfusion strategies for people with haematological malignancies treated with intensive chemotherapy or radiotherapy, or both, with or without haematopoietic stem cell support. Cochrane Database Syst Rev. 2024;5:Cd 011305.38780066 10.1002/14651858.CD 011305.pub 3PMC 11112982 · doi ↗ · pubmed ↗
- 8Pagano MB , Dennis JA , Idemudia OM , Stanworth SJ , Carson JL . An analysis of quality of life and functional outcomes as reported in randomized trials for red cell transfusions. Transfusion. 2023;63:2032–2039.37723866 10.1111/trf.17540 · doi ↗ · pubmed ↗