Analysis of the representation of skin tone diversity amongst medical resources illustrating dermatological manifestations of dermatomyositis, systemic sclerosis and vasculitis
Stacey Kihumba, Giles Dixon, Matthew Wells, Sarah Rudd, Jo Hardy, Harsha Gunawardena, John D Pauling, Huzaifa Adamali, Shaney L Barratt

TL;DR
Medical resources show a lack of skin tone diversity in images of dermatological conditions, leading to potential healthcare inequities.
Contribution
This study quantifies the underrepresentation of diverse skin tones in medical literature for specific autoimmune diseases.
Findings
A significant unequal distribution of skin tones was found in medical images (P < 0.001).
No improvement in skin tone representation was observed from 2009 to 2022.
Images predominantly depicted lighter skin tones (median skin tone category 1–2).
Abstract
Cutaneous manifestations of systemic autoimmune rheumatic disease–interstitial lung disease (SARD-ILD) are clinically useful diagnostic features that can support early diagnosis and management. However, medical education resources often lack diversity in representing skin tones, which lead to inequities in healthcare delivery. Our study aimed to quantify the proportion of skin tones represented in medical literature that depict cutaneous features relevant to SARD-ILD. A structured search of medical resources was conducted with the support of North Bristol NHS Trust Library and Knowledge Service. We systemically reviewed images of cutaneous signs associated with SSc, DM and vasculitis. Images that did not depict these conditions were excluded. Each image was assigned a Monk Skin Tone (MST) Scale score (1–10). A chi-square goodness-of-fit analysis was used to establish whether the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
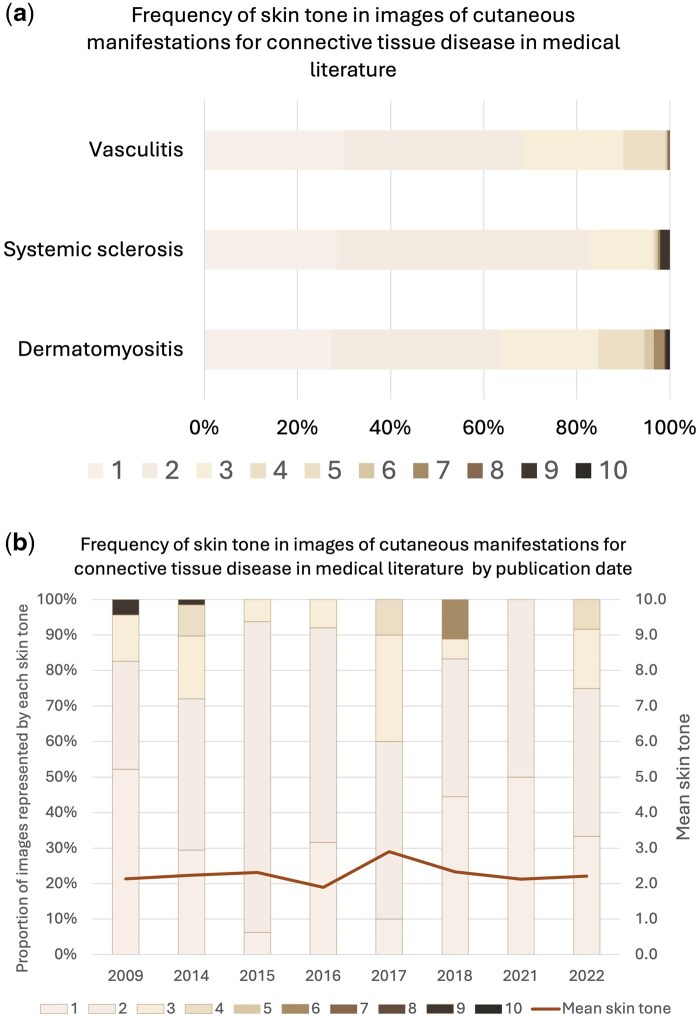 Figure 1
Figure 1| Clinical sign | Frequency ( |
|---|---|
| Active Raynaud’s syndrome | 58 |
| Calcinosis/calcinosis cutis | 38 |
| Digital ulcers/ischaemia | 30 |
| Erythema nodosum | 12 |
| Gottron’s papules | 183 |
| Heliotropic rash | 80 |
| Livedo reticularis | 25 |
| Mechanic’s hands | 33 |
| Microstomia | 4 |
| Nailfold capillary dilatation | 26 |
| Palmar erythema | 20 |
| Palmer papules | 5 |
| Periungual overgrowth | 12 |
| Puffy fingers | 15 |
| Reverse Gottron’s sign | 11 |
| Sclerodactyly | 23 |
| Shawl/V/Holster sign | 48 |
| Splinter haemorrhages | 10 |
| Telangiectasia | 26 |
| Vasculitic purpuric rash/purpura | 82 |
| Vasculitis cutaneous ulceration/nodules | 49 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Dermatological and COVID-19 studies · Inflammatory Myopathies and Dermatomyositis
Introduction
Interstitial lung disease (ILD) encompasses a heterogeneous group of diseases that cause varying degrees of fibrosis and inflammation within the lungs with significant impact upon quality of life. Approximately 30% of ILDs are secondary to a systemic autoimmune rheumatic disease–interstitial lung disease (SARD-ILD) [1]. Recognition of cutaneous manifestations of SARD is essential in differentiating SARD-ILD from other causes of ILD, directly influencing diagnostic pathways, treatment strategies, and prognostic assessments.
Prior research indicates that less than 5% of dermatological images in medical education literature feature darker skin tones [2]. Cutaneous manifestations in individuals with darker skin often present differently, making their underrepresentation problematic [3]. Reduced diagnostic confidence among clinicians and delayed diagnosis in dermatology clinics have been widely reported [4, 5]. Given that people of global majority have a higher incidence and greater morbidity associated with systemic inflammatory disease, failure to accurately depict these manifestations in educational materials may exacerbate existing health disparities [6–9].
This study aimed to quantify and assess representation of diverse skin tones in medical education resources that illustrate SARD-ILD-related cutaneous signs, specifically related to SSc, vasculitis and DM. Additionally, we examined whether any improvements in diversity had been made in educational materials over time.
Methods
The North Bristol NHS Trust Library and Knowledge Service identified educational resources comprising of subscribed electronic resources, print and e-books included in stock. A systematic search of these resources was performed (searches performed June 2024), and images depicting cutaneous manifestations of SSc, vasculitis and DM were selected (Supplementary Table S1, available at Rheumatology Advances in Practice online). Where electronic search was possible, the name of the sign was used in the search; in textbooks, a manual search of the literature was performed.
Monochrome images, poor-quality images or images of signs of relevance observed in patients with alternative aetiology (e.g. petechial rash in meningococcal disease) were excluded from analysis. Each suitable image was assigned a Monk Skin Tone (MST) Scale score [1–10], a validated scale where lower values indicate lighter skin tones [10].
Collected data were analysed by chi-square goodness-of-fit analysis using SPSS version 29 (IBM, USA). The chi-square goodness of fit expected uniform distribution of representation of skin tone. The study was registered with the local quality improvement department (QI10728) but did not require institutional ethics approval.
Results
A total of 16 e-resources and 26 textbooks were identified, with 8 and 14, respectively, containing relevant images (Supplementary Table S2, available at Rheumatology Advances in Practice online). Textbooks were published either in the UK (n = 9) or the USA (n = 5). Of the 790 images, 585 were from e-resources and 205 from textbooks and were published between 2009 and 2022. Notably, of the 790 images, 401 represented DM, 190 SSc and 199 vasculitis.
The breakdown of the number of images per clinical sign can be seen in Table 1.
Skin tone representation
A significant overrepresentation of lighter skin tones was observed across all clinical signs and disease cohorts (Fig. 1). The chi-square test confirmed a skew towards lighter MST categories, with darker skin tones (higher MST category) largely underrepresented, χ^2^(9) = 1506.8, P < 0.001. The standardized residuals identified that tones 1 and 2 were significantly over-represented (16.18 and 27.76, respectively).
Frequency of skin tone. (a) Frequency of skin tone representation in images of cutaneous manifestations for systemic autoimmune rheumatic disease (SARD) in medical literature. Colours represent the percentage of overall image count represented by each Monk Skin Tone. DM (n = 401), SSc (n = 190) and vasculitis (n = 199). (b) Frequency of skin tone in images of cutaneous manifestations of connective tissue disease in medical literature by publication date
Image representation by publication date
Of the textbooks analysed, the earliest publication year was 2009 and the most recent was 2022. The mean skin tone did not significantly change between 2009 and 2022 (mean MST category 2.3; S.D. ± 0.29).
Discussion
The study provides compelling evidence that educational resources continue to lack equitable representation of dermatological manifestations of SARD-ILD in darker skin tones, despite extensive literature advocating change since 2006 [11].
Whilst previous work has highlighted this issue, to our knowledge ours is the first study to demonstrate this shortcoming with respect to SARD-ILD. This may be of particular concern given the greater prevalence of many SARDs amongst people of global majority and racial disparities in outcomes [9].
This lack of diversity of skin tones in educational resources is likely to be multifactorial. The presumption that lighter skin demonstrates pathology more clearly may have led to selection bias by authors and publication bias amongst editors. Historically, technical challenges may be contributory; however, modern photographic advancements have allowed for more accurate documentation of cutaneous signs on darker skin tones [12, 13]. The feature of image stabilization in digital cameras has helped to maintain the definition of images capturing dermatological conditions without diminishing colour and degrading lesion margins. Furthermore, utilization of apposite digital camera settings aids in defining colour and limiting interference from the ambient light source [12].
With respect to geographical bias, many medical textbooks originate from regions where lighter skin is predominant, which may influence image selection. The textbooks that contributed the images to the data set were published in the UK and USA, countries in which white individuals account for the largest percentage of their populations: 81.7% and 75.3%, respectively. Despite this, these countries still contain significant populations with darker skin, and patients with darker skin and cutaneous manifestations of SARD-ILD will be present and could be selected for inclusion in relevant literature.
The overrepresentation of lighter skin tones may contribute to diagnostic bias, delayed recognition, and misdiagnosis of cutaneous conditions in patients with darker skin [3, 14]. Research has shown that greater diversity in dermatological education materials improves clinician confidence and diagnostic accuracy, ultimately leading to earlier interventions and better patient outcomes [15].
The need for wider representation of darker skin tones amongst educational resources extends to patients with SARD. Despite awareness of this shortcoming dating back almost 20 years, there appears to have been insufficient progress to enhance representation in medical images over this period [11]. Our study underscores the urgent need for a systemic effort to increase the representation of diverse skin tones in medical education. A concerted effort is necessary to ensure wider representation of skin tones within educational resources, ensure ethical distribution and incorporate these into both the undergraduate and postgraduate medical curriculums. Clinicians and researchers should actively contribute images of dermatological conditions in people of global majority. Importantly, medical organizations should establish guidelines promoting equitable representation in visual medical resources. Future trials should also analyse whether diverse representation in educational resources influences diagnostic accuracy, treatment efficacy and patients’ outcomes, thereby addressing systemic disparities in research.
There are some limitations to the methodology used in the present study. The images were analysed by a single author, introducing the potential for bias. However, previous work has demonstrated a high intraclass correlation coefficient, hopefully minimizing the effect of single review [16]. Future work may consider using the consensus of a panel of clinicians or artificial intelligence to quantify skin tones. However, it is unlikely that subjective variation of skin tone assessment would have significantly altered the findings of this study, which are in keeping with previous findings. Furthermore, no specific sample size calculation was undertaken due to the paucity of pilot or feasibility data in this field.
There are other SARDs which have cutaneous manifestations, such as rheumatoid arthritis and Sjogren’s syndrome. While direct conclusions about these specific conditions cannot be drawn, the pronounced disparity observed in our study suggests that similar patterns are likely to exist in other SARDs.
A relative strength of this project is the structured resource search that incorporated the mainstream educational resources as identified by a large University Hospital library service. Additional work is required to establish whether addressing the shortfall in representation of darker skin tones within the medical literature improves diagnostic performance and outcomes.
This study has highlighted the need for educational resources to be more representative of the populations they serve. This will require significant effort and resources to redress the balance but may contribute to a reduction in healthcare inequality.
Supplementary Material
rkaf114_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mittoo S , Gelber AC, Christopher-Stine L et al Ascertainment of collagen vascular disease in patients presenting with interstitial lung disease. Respir Med 2009;103:1152–8.19304475 10.1016/j.rmed.2009.02.009 · doi ↗ · pubmed ↗
- 2Louie P , Wilkes R. Representations of race and skin tone in medical textbook imagery. Soc Sci Med 2018;202:38–42.29501717 10.1016/j.socscimed.2018.02.023 · doi ↗ · pubmed ↗
- 3Diao JA , Adamson AS. Representation and misdiagnosis of dark skin in a large-scale visual diagnostic challenge. J Am Acad Dermatol 2022;86:950–1.33812954 10.1016/j.jaad.2021.03.088 · doi ↗ · pubmed ↗
- 4Wu XC , Eide MJ, King J et al Racial and ethnic variations in incidence and survival of cutaneous melanoma in the United States, 1999-2006. J Am Acad Dermatol. 2011;65:S 26-37.22018064 10.1016/j.jaad.2011.05.034 · doi ↗ · pubmed ↗
- 5Serrano L , Ulschmid C, Szabo A, Roth G, Sokumbi O. Racial disparities of delay in diagnosis and dermatologic care for hidradenitis suppurativa. J Natl Med Assoc 2022;114:613–6.36511276 10.1016/j.jnma.2022.08.002 · doi ↗ · pubmed ↗
- 6Medsger TA , Dawson WN, Masi AT. The epidemiology of polymyositis. Am J Med 1970;48:715–23.5420557 10.1016/s 0002-9343(70)80006-7 · doi ↗ · pubmed ↗
- 7Hannah JPF , Odingo M. Incidence, prevalence & mortality in idiopathic inflammatory myopathies & associated interstitial lung disease in England: a national cohort using routinely collected administrative data. Ann Rheumatic Dis 2023;82(Suppl 1).
- 8Adegunsoye A , Freiheit E, White EN et al Evaluation of pulmonary fibrosis outcomes by race and ethnicity in US adults. JAMA Netw Open 2023;6:e 232427.36897590 10.1001/jamanetworkopen.2023.2427 PMC 10984340 · doi ↗ · pubmed ↗