Isolated Carpometacarpal Dislocation Without Associated Fracture: A Case Report of High-Energy Wrist Trauma
Mohammed S Al Saleem, Fatimah ALthabit, Arwa H AlOnayzan, Khadijah Alruwaili, Adia Almutairi

TL;DR
A rare case of wrist trauma with carpometacarpal joint dislocation and no fractures is reported, highlighting the importance of early diagnosis and surgery for recovery.
Contribution
This case report adds to the limited literature on isolated CMC dislocations without fractures, emphasizing clinical management and successful outcomes.
Findings
The patient had dorsal dislocation of multiple CMC joints without metacarpal fractures following high-energy trauma.
Emergency reduction resolved absent pulses and numbness, and CT angiography confirmed no arterial injury.
At four months post-treatment, the patient regained full wrist and finger motion and normal grip strength.
Abstract
Carpometacarpal (CMC) joint dislocations without fractures are rare and often missed due to subtle clinical and radiographic signs. We report a case of a 28-year-old male patient involved in a motorbike rollover who sustained open comminuted radius and ulna fractures, an ulnar styloid fracture, and dorsal dislocation of multiple CMC joints without metacarpal fractures. He presented with absent distal pulses and finger numbness, which resolved after emergency reduction. CT angiography ruled out arterial injury. He underwent internal fixation of forearm fractures and Kirschner wire stabilization of CMC joints. At four months, he achieved full wrist and finger motion, normal grip strength, and no instability. Early diagnosis and timely surgical intervention were key to recovery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3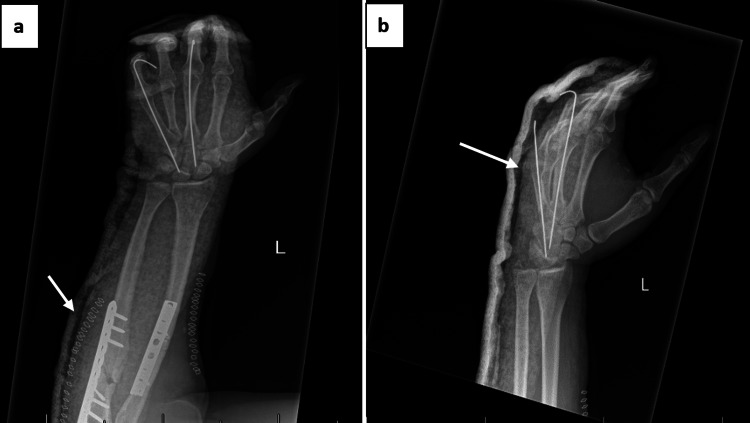 Figure 4
Figure 4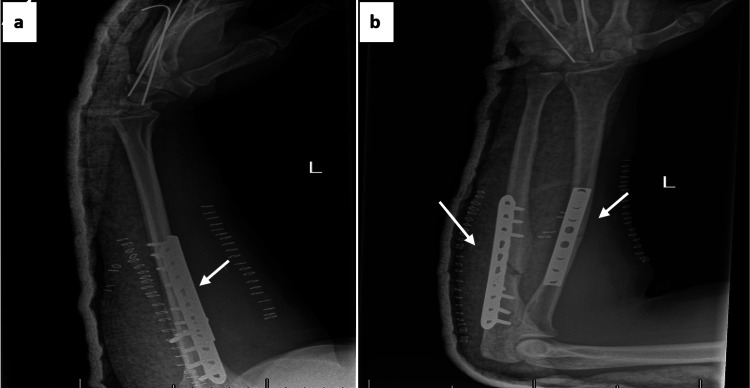 Figure 5
Figure 5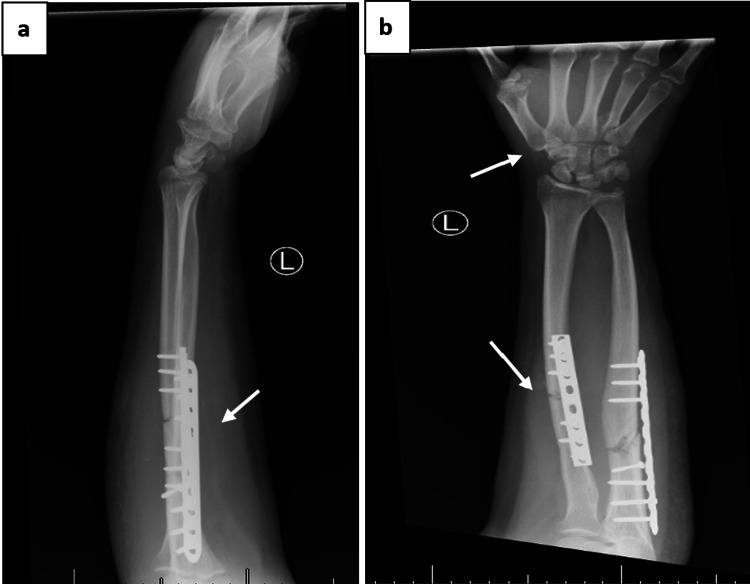 Figure 6
Figure 6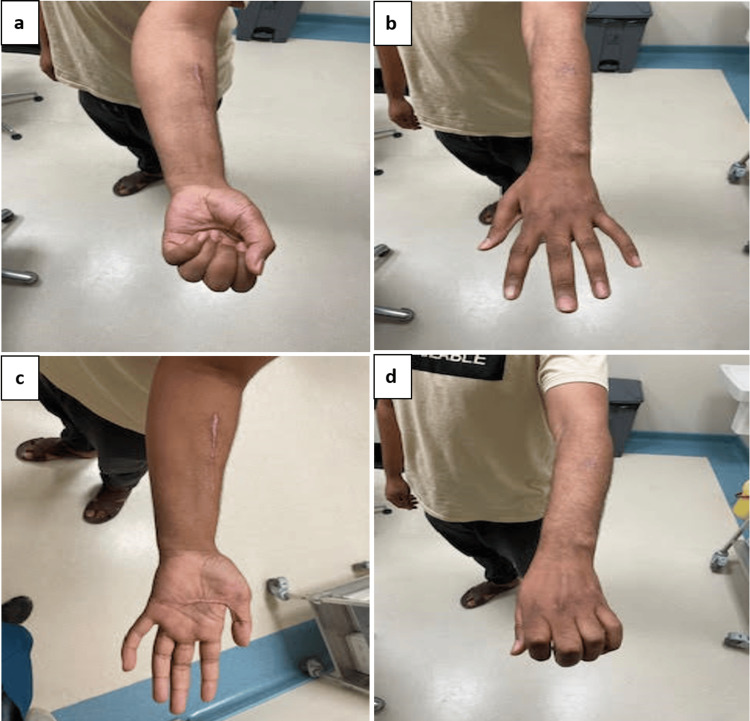 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Elbow and Forearm Trauma Treatment · Traumatic Ocular and Foreign Body Injuries
Introduction
Isolated dislocations of the carpometacarpal (CMC) joints are uncommon, comprising less than 1% of all hand and wrist injuries [1]. They are typically the result of high-energy trauma, such as motor vehicle accidents or falls from significant height. Among these, dislocations of the ulnar-side joints, particularly the fourth and fifth CMC joints, are most frequent, often occurring dorsally due to the strong volar ligamentous support [2]. These injuries are frequently overlooked in the acute setting, especially when accompanied by more apparent or urgent trauma, as clinical signs may be subtle and conventional wrist radiographs can fail to detect the dislocation due to overlapping osseous anatomy [1,2]
Accurate and timely diagnosis requires a high index of suspicion, supplemented by appropriate imaging. While standard dorsopalmar, lateral, and oblique radiographs are essential for initial assessment, computed tomography (CT) remains the gold standard for confirming dislocations, identifying subtle fractures, and aiding surgical planning [3]. Missed or delayed diagnosis may lead to poor outcomes, including chronic pain, grip weakness, joint instability, tendon irritation, and early-onset post-traumatic arthritis [2,3].
Management depends on the severity and timing of the injury. While acute, isolated CMC dislocations may be treated with closed reduction, post-reduction instability is common, often requiring percutaneous Kirschner wire (K-wire) stabilization [4]. In complex injuries, such as open dislocations, those with associated fractures, or delayed presentations, open reduction and internal fixation (ORIF) is typically indicated to restore anatomical alignment, decompress neurovascular and soft tissue structures, and enable early mobilization [5].
The purpose of this study is to highlight a rare and clinically important case of isolated CMC dislocation without metacarpal fractures, combined with open forearm fractures in a young man following high-energy trauma. This case underscores the need for early recognition, advanced imaging, and timely surgical management, contributing valuable insight to the limited literature on complex CMC injuries.
Case presentation
Clinical presentation and history
A 28-year-old medically free male was presented to the Emergency Department (ED) after a high-energy road traffic accident (RTA) involving a motorbike rollover. Upon arrival, he was conscious, alert, and fully oriented with a Glasgow Coma Scale (GCS) score of 15/15. He was hemodynamically stable, with a temperature of 37°C, a heart rate of 74 beats per minute, a respiratory rate of 22 breaths per minute, a blood pressure of 119/72 mmHg, and an oxygen saturation of 98% on room air.
Primary assessment confirmed an intact airway and spontaneous breathing. A large-bore intravenous cannula was inserted, and 500 mL of normal saline was administered after blood was sent for initial laboratory investigations. No signs of intra-abdominal injury were noted, and the pelvis was clinically stable.
Examination
Focused examination of the left forearm revealed an open, comminuted fracture with severe swelling and a visible wound on the volar aspect of the hand (Figure 1). The patient reported numbness in all fingers. Pre-reduction assessment showed absent distal radial and ulnar pulses. After gentle alignment in the ED, pulses remained impalpable but were confirmed by Doppler ultrasound.
Open volar wound with severe swelling and deformity of the hand on presentation
Investigations and procedure
Initial radiographs revealed diaphyseal comminuted fractures of the radius and ulna, an ulnar styloid fracture, and dorsal dislocation of the wrist joint (Figure 2). Additional views confirmed the presence of a dorsal carpometacarpal dislocation (Figure 3).
Initial radiographs: (a) lateral view showing comminuted fractures of the radius and ulna, (b) anteroposterior view demonstrating ulnar styloid fracture and wrist dislocation.
Additional X-ray views confirming left carpometacarpal (CMC) joint dislocation: (a) oblique view, (b) lateral view highlighting dorsal displacement
A CT angiogram demonstrated intact subclavian, axillary, and brachial arteries. The radial artery showed segmental attenuation without a cutoff; the ulnar artery was intact. Vascular surgery consultation concluded that no intervention was needed due to the absence of major arterial injury.
The patient underwent urgent ORIF of both radius and ulna using dynamic compression plates, along with percutaneous K-wire fixation of the dislocated carpometacarpal joints for stabilization (Figure 4). Final intraoperative X-rays confirmed appropriate reduction and hardware positioning (Figure 5).
Intraoperative images: (a) ORIF of radius and ulna using DCP, (b) K-wire fixation of carpometacarpal joints.ORIF: open reduction and internal fixation; DCP: dynamic compression plate; K-wire: Kirschner wire
Postoperative radiographs: (a) lateral view showing stable fixation of forearm fractures, (b) anteroposterior view confirming anatomical reduction and implant position
Postoperative management and follow-up
The patient was monitored postoperatively for neurovascular status, wound condition, and signs of infection. Pain management and intravenous antibiotics were administered according to hospital protocol. One month after surgery, the K-wires were removed, and the patient began a structured physiotherapy program focusing on wrist mobility and grip strength restoration. Post-K-wire removal radiographs are shown in Figure 6.
One-month follow-up after removal of K-wires: (a) lateral view showing stable fixation of radius and ulna with plates and screws, (b) Anteroposterior view confirming maintained alignment and absence of K-wires
At the four-month follow-up, the patient demonstrated a full range of motion in the wrist and fingers, normal grip strength, and no evidence of residual instability or pain. He was able to return to normal daily activities with no functional limitations. Clinical recovery is shown in Figure 7.
Clinical photos at four months demonstrating full recovery of wrist motion and hand function: (a) wrist flexion, (b) wrist extension, (c) forearm supination, (d) forearm pronation
Discussion
CMC joint dislocations are rare, accounting for less than 1% of all hand and wrist trauma cases [3]. Diagnosis is often delayed due to subtle clinical signs and the overlapping anatomy of carpal and metacarpal bases, which can obscure findings on standard radiographs [3]. In the present case, the diagnosis was not immediately apparent from initial plain films due to complex forearm fractures and extensive soft tissue swelling. However, a high index of clinical suspicion, combined with advanced imaging, confirmed the dorsal dislocation of multiple CMC joints. This supports current recommendations for obtaining three-view radiographs, dorsopalmar, lateral, and oblique, and utilizing CT when findings remain equivocal [6].
Management of CMC dislocations is influenced by the timing of presentation and joint stability after reduction. While closed reduction may be successful in early, uncomplicated dislocations, open reduction is often required in cases of open injuries, fracture-dislocations, or delayed presentation due to interposed soft tissue, bony fragments, or severe edema [7]. In this report, the patient presented acutely with open comminuted fractures of the radius and ulna, along with CMC dislocation, necessitating open surgical intervention to achieve adequate reduction and stabilization.
Post-reduction instability is common in complex CMC dislocations and frequently requires temporary internal fixation. In this case, the extent of injury and associated soft tissue damage resulted in instability following reduction, which was managed with percutaneous K-wire fixation to maintain anatomical alignment. This approach is consistent with evidence suggesting that K-wire stabilization is indicated when joint congruity cannot be reliably maintained by closed means [8]. This case also contrasts with reports of isolated CMC dislocations successfully treated with splint immobilization [9], highlighting the need to individualize treatment based on injury complexity.
The mechanism of injury in this case, a high-energy motorbike rollover, is relatively uncommon in published series. A large retrospective study involving 4,751 patients reported punching as the most common cause of CMC dislocation (73%), followed by blunt trauma (18%) and road traffic accidents (9%) [9]. Additionally, several patients in that study were misdiagnosed initially and presented in a delayed fashion. In contrast, early recognition and coordinated surgical management in the present case may have contributed to the favorable functional outcome.
Despite the potential for complications such as tendon adhesions, stiffness, post-traumatic arthritis, and complex regional pain syndrome, many patients recover well following prompt intervention and structured rehabilitation [10,11]. In the current case, the patient regained full wrist and hand function by four months postoperatively, with no residual pain, weakness, or instability. This outcome is consistent with previous reports demonstrating excellent functional recovery when anatomical reduction is achieved and early rehabilitation is implemented [12].
Conclusions
Isolated CMC dislocation without metacarpal fracture is a rare and easily missed injury. This case highlights the value of early recognition, advanced imaging, and timely surgical management. ORIF and K-wire stabilization resulted in excellent functional recovery, emphasizing the importance of individualized treatment in complex hand trauma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isolated volar dislocation of the fifth carpometacarpal joint Ochsner J Desai B Nammour M Warren M Sumarriva G Sisco-Wise L 2152182020203261247910.31486/toj.18.0151 PMC 7310188 · doi ↗ · pubmed ↗
- 2Management of acute and chronic thumb CMC joint dislocations Hand Clin Weeks D Donato D 2692793820223546594410.1016/j.hcl.2022.01.003 · doi ↗ · pubmed ↗
- 3Carpometacarpal joint fracture dislocation of second to fifth finger Clin Orthop Surg Pundkare GT Patil AM 430435720152664062410.4055/cios.2015.7.4.430PMC 4667109 · doi ↗ · pubmed ↗
- 4Rare carpometacarpal dislocations Orthop Traumatol Surg Res Lefere M Dallaudière B Omoumi P Cyteval C Larbi A 81381610220162721050610.1016/j.otsr.2016.04.003 · doi ↗ · pubmed ↗
- 5Plate versus Kirschner wire fixation in treatment of fourth and fifth carpometacarpal fracture-dislocations: a retrospective cohort study Int J Surg Bao B Zhu H Zheng X 2932965220182953082510.1016/j.ijsu.2018.01.052 · doi ↗ · pubmed ↗
- 6Carpometacarpal dislocation of the third to fifth fingers and an associated fracture of the hamate in a military paratrooper Case Rep Orthop 6 2020 Kalinterakis G Antonogiannakis E Abdi A 2861604202020203269553810.1155/2020/2861604 PMC 7350069 · doi ↗ · pubmed ↗
- 7Carpometacarpal joint dislocations: management and long-term outcomes at a specialized hand surgery center in Latin America Plast Surg (Oakv) Telich-Tarriba JE Guevara-Valmaña OI Navarro-Barquín DF Victor-Baldin A 2102142820203321503510.1177/2292550320933690 PMC 7644835 · doi ↗ · pubmed ↗
- 8Conservative treatment of carpometacarpal dislocation of the three last fingers Case Rep Emerg Med Jumeau H Lechien P Dupriez F 4962021201620162770381710.1155/2016/4962021 PMC 5039287 · doi ↗ · pubmed ↗