Disseminated rhino-orbital-cerebral mucormycosis in Philadelphia chromosome-positive mixed phenotype acute leukemia: a case report and literature review
Yao Zhou, Meijuan He, Qiu Zhang, Jia Yao, Zheng Wang, Baoan Chen, Jiamin Guo, Fengming Gao, Zefa Liu

TL;DR
A rare case of a severe fungal infection in a leukemia patient highlights the need for better antifungal prevention and early diagnosis.
Contribution
First reported case of ROCM in a patient with Philadelphia chromosome-positive mixed phenotype acute leukemia.
Findings
ROCM was confirmed in a Ph+ MPAL patient despite voriconazole use.
Liposomal amphotericin B effectively controlled the infection.
Voriconazole may not prevent Mucorales infections in immunocompromised patients.
Abstract
Rhino-orbital-cerebral mucormycosis (ROCM) is a rapidly progressing and life-threatening fungal infection caused by fungi in the order Mucorales. It predominantly affects immunocompromised individuals, such as those undergoing chemotherapy for hematological malignancies. Despite its high mortality rate, ROCM remains underrecognized, and its clinical features in patients with Philadelphia chromosome-positive (Ph+) mixed phenotype acute leukemia (MPAL) are rarely reported. This report describes a 48-year-old female who presented with a one-week history of fever without localized pain and was diagnosed with Ph+ MPAL by laboratory blood tests and comprehensive bone marrow examination. She was treated with imatinib and received acute lymphoblastic leukemia (ALL)-like chemotherapy, and used voriconazole to prevent fungal infections. On day 9 of admission, the patient developed fever and skin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
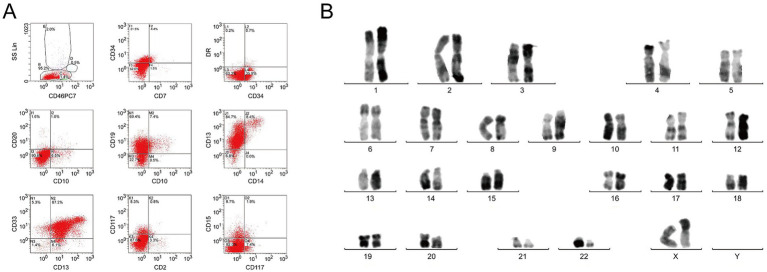 Figure 1
Figure 1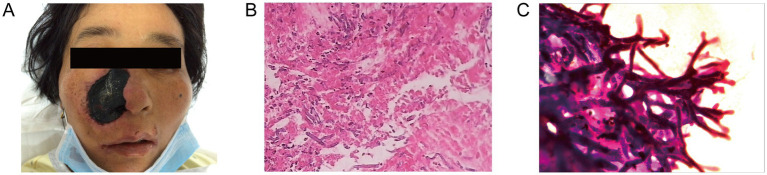 Figure 2
Figure 2| Time | Clinical features | Biology results | Therapy strategies |
|---|---|---|---|
| Day 1 | Fever | CRP 112.6 mg/L | Hefoperazone/sulbactam 9 g/day IV and hydroxyurea 3 g/day p.o. |
| Day 3 | Bone marrow pathology and fever | MPAL, WBC 136.8 × 109/L | Cyclophos-phamide 0.4 g/day IV, dexamethasone 10 mg/day I, and voriconazole 4 mg/kg, q12h IV |
| Day 6 | Bone marrow pathology and fever | Ph + MPAL, WBC 73.2 × 109/L | Imatinib 400 mg/day, vincristine 2 mg/qwx4, daunorubicin 30 mg/m2 day 1–3, prednisone 60 mg/m2 day 1–28 |
| Day 9 | Fever again, skin lesions on the nasal | WBC 2.51 × 109/L, ANC 0.1 × 109/L, CRP 57.81 mg/L, CT of the chest (−) | Imipenem and cilastatin sodium 1.0 q6hIV, vancomycin 2.0 q12h, voriconazole 4 mg/kg q12h IV |
| Day 15 | Skin lesions expand | Pathology shows mucormycosis, wound secretion culture shows Rhizomucor, (1,3)-β-D-glucan assay (−), galactomannan test (−) | L-AmB at 3 mg/kg qdIV, imipenem and cilastatin sodium 1.0 q6hIV |
| Day 18 | Persistence of fever | WBC 0.30 × 109/L, ANC 0.1 × 109/L | Granulocyte-colony stimulating factor 150 μg bid subcutaneous |
| Day 23 | Bone marrow pathology and persistence of fever | WBC 4.47 × 109/L, ANC 3.5 × 109/L, complete remission | Discharge home |
| Case reports | Age and sex | Type of disease | Surgical debridement | Therapeutic drugs | Effective remission of the infection |
|---|---|---|---|---|---|
| Ding et al. ( | 46/F | AML | Yes | AmB | No |
| Yamamoto et al. ( | 42/M | AML | Yes | L-AmB, micafungin | Yes |
| Popa et al. ( | 7/F | ALL | Yes | AmB | Yes |
| Yang et al. ( | 1/M | ALL | No | AmB, posaconazole | No |
| Yeung et al. ( | 57/M | AML M5a | No | L-AmB, imipenem, amikacin | No |
| Samanta et al. ( | 8/M | ALL | Yes | L-AmB | Yes |
| Siriwardena et al. ( | 35/F | AML | Yes | L-AmB | No |
| Siriwardena et al. ( | 29/F | AML | Yes | L-AmB, antibiotics | Yes |
| Siriwardena et al. ( | 42/M | AML | Yes | L-AmB | No |
| Hu et al. ( | 1/M | ALL | No | L-AmB, voriconazole | No |
| Ojeda-Diezbarroso et al. ( | 12/F | ALL | Yes | L-AmB, posaconazole | Yes |
| Uraguchi et al. ( | 70/M | AML M5b | Yes | L-AmB, antibiotics | No |
| Wehl et al. ( | 1/M | ALL | No | L-AmB, antibiotics | No |
| Mutchnick et al. ( | 2/M | ALL | Yes | AmB, posaconazole, micafungin | Yes |
| Dworsky et al. ( | 17/F | BCP-ALL | Yes | L-AmB, micafungin | Yes |
| Gumral et al. ( | 40/M | ALL | Yes | L-AmB | Yes |
| Raj et al. ( | 55/M | APL | Yes | L-AmB | Yes |
| Sigera et al. ( | 19/M | B-ALL | Yes | L-AmB | No |
| Lerchenmüller et al. ( | 28/M | ALL | Yes | L-AmB | Yes |
| Cofré et al. ( | 2/F | ALL | Yes | AmB | Yes |
| Ammon et al. ( | 24/F | AML | No | AmB, flucytosine | Yes |
| Jacobs et al. ( | 35/F | AML | No | AmB | No |
| Jacobs et al. ( | 17/M | ALL | No | AmB, echinocandin FK463 | Yes |
| Parkyn et al. ( | 3/M | BCP-ALL | No | L-AmB | Yes |
| Andreani et al. ( | 59/M | sAML | Yes | L-AmB, isavuconazole | Yes |
| Funada et al. ( | 21/M | BCP-ALL | No | AmB | Yes |
| Brusis and Rister ( | 12/M | ALL | Yes | AmB | Yes |
- —National Natural Science Foundation of China10.13039/501100001809
- —Open Project of Jiangsu Biobank of Clinical Resources
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Acute Lymphoblastic Leukemia research
Introduction
1
Mucormycosis is a globally invasive fungal infection caused by members of the genera Mucor, Rhizopus, Rhizomucor, and Lichtheimia (formerly Absidia) in the order Mucorales (1). Mucormycosis rarely occurs in immunocompetent individuals but frequently occurs in immunocompromised patients (2). The incidence of mucormycosis has been increasing over the past decade, especially since the onset of COVID-19, and the condition is fatal in most patients (3, 4). Mucormycosis can present in different forms, including pulmonary, cutaneous, rhino-orbito-cerebral, gastrointestinal, and disseminated types (5). In the clinical situations, diabetes mellitus has evolved as a major risk factor for mucormycosis, while in more recent years, underlying malignancy has emerged as a critical risk factor due to the increasing number of patients undergoing chemotherapy or cancer immunotherapy (6–8).
A number of retrospective studies have shown that mucormycosis accounts for only a small proportion of breakthrough invasive fungal infection in patients with hematological malignancies (9). According to the SEIFEM study, mucormycosis is present in only 0.1% of patients with hematological malignancies (10), with pulmonary mucormycosis being the most common (11, 12). Biopsy is the preferred method for mucormycosis diagnosis but may not be an option in the early course of the disease, resulting in delayed diagnosis and missed opportunities for timely treatment (13). Antifungal therapy is usually used clinically, but it is usually difficult to treat infections effectively by drugs. Combined surgical debridement can improve the treatment effect and patient survival rate (14, 15).
Herein, we report a case of Philadelphia chromosome-positive (Ph+) mixed phenotype acute leukemia (MPAL) combined with rhino-orbital-cerebral mucormycosis (ROCM) infection, with the timely use of liposomal amphotericin B (L-AmB) to treat and control the infection. Highlighting the importance of early diagnosis and treatment of mucormycosis, it also provides important insights into the selection of prophylactic therapy for patients with hematological malignancies.
Case description
2
A 48-year-old woman who presented with fever in the absence of pain for 1 week was admitted to People’s Hospital of Xinghua City (Jiangsu Province, China). Physical examination was negative. Blood routine test demonstrated a white blood cell count (WBC) of 180.7 (4.0–10.0) × 10^9^/L; hemoglobin of 123 (110–150) g/L and platelets of 53 (100–300) × 10^9^/L. Bone marrow biopsy showed hypercellularity with 83.5% blast cells. Eosinophilia was not evident in either peripheral blood or bone marrow. Flow cytometry analysis showed that the blast cells, which accounted for 95.2% of bone marrow karyocytes, were strongly positive for CD34, CD19, CD13, CD33, CD11b, CD64, myeloperoxidase, and CD79a (Figure 1A). According to the World Health Organization (WHO) 2022 criteria, the patient was diagnosed with MPAL with co-expression of myeloid and B lymphoid lineage antigen. The chromosomal analysis of bone marrow cells revealed t(9;22) (q34;q11) translocation (Figure 1B). Molecular genetics showed BCR/ABL (e1a2) fusion gene, thereby confirming the diagnosis of Ph+ MPAL.
Immunophenotype and karyotype characteristics of bone marrow specimens. (A) Representative flow cytometry histograms demonstrate the expression of CD34, CD19, CD13, CD33, CD 11b, CD64, and CD79a. (B) G-banding karyotype of the BM cells demonstrates t(9;22) (q34;q11).
The timeline of diagnosis and treatment is shown in Table 1. On the 6th day of admission, the patient was treated with imatinib (400 mg/day) and acute lymphoblastic leukemia (ALL)-like chemotherapy (VDP regimen: vincristine 2 mg/qwx4; daunorubicin 30 mg/m^2^, day 1–3; prednisone 60 mg/m^2^, day 1–28). Also, preventive treatment was given with voriconazole (4 mg/kg, q12h).
On day 9 after admission, the patient’s body temperature reached 38.6 °C, and developed skin lesions on the right nasal area. The skin lesions spread rapidly to the entire right nasal area after 6 days (Figure 2A). Blood routine test demonstrated WBC 2.51 × 10^9^/L, hemoglobin 80.2 g/L, platelets 18 × 10^9^/L, and absolute neutrophil count (ANC) of 0.1 × 10^9^/L. C-reactive protein (57.81 mg/L) and procalcitonin (0.13 ng/mL) were both elevated. Chest computed tomography (CT) examination was negative, and serum (1,3)-β-D-glucan, galactomannan tests, and blood culture examinations were negative. Skin biopsy revealed hyphae consistent with mucormycosis. Wound secretion culture was positive for Rhizomucor species (Figures 2B,C). After the diagnosis of mucormycosis, according to the guidelines of the Infectious Diseases Society of America (IDSA), we administered L-AmB at 3 mg/kg/day and successfully controlled the infection. On the 23rd day of admission, the patient achieved complete remission of the infection.
Characterization of infected tissues. (A) Initial clinical presentation on the whole right nasal. The skin lesion area is approximately 4 cm × 3 cm. Pathological section of necrotic tissue of right nasal cavity. Hematoxylin and eosin-stained sections show an angioinvasive growth of mucormycosis at a magnification of ×100 (B) and ×400 (C).
We suggested bone marrow transplantation as the best option for her treatment, but she refused. The patient died of intracranial hemorrhage after 1 year.
Literature review
3
Because no cases of MPAL infection with mucormycosis have been reported, we searched PubMed using the terms “rhinocerebral mucormycosis,” “acute leukemia” and “case report” and found 44 articles published between 1982 and June 2025. There were 24 eligible case reports, which included complete information on a total of 27 patients (16–39). Information on age, sex, disease type, treatment, and clinical outcomes was collected for these patients (Table 2).
The patients, 18 males and 9 females, were mainly young and middle-aged, with a median age of 21 years (age range: 1–70 years). All patients were treated with amphotericin B (AmB) or L-AmB, and 48% were also treated with other microbicides. Surgical resection proved highly effective in controlling mucormycosis, with only 44% of non-surgical patients successfully controlled the infection, compared with 72% of surgical patients. In our case, the patients’ symptoms were effectively relieved by drug therapy alone. This encouraging result might be attributed to the timely diagnosis of Mucorales infection and the implementation of effective antifungal strategies.
This encouraging result may be attributed to the timely diagnosis at the early stage of Mucor infection.
Discussion
4
In 2022, the WHO classification was updated, but the main criteria for MPAL remained unchanged, except for cases defined by myeloperoxidase alone for the myeloid lineage. A new subcategory of BCR/ABL1-positive MPAL was introduced (40). In this case, the patient’s heightened susceptibility to invasive fungal infections likely arises from a confluence of immune impairments directly linked to both the disease biology and its treatment (41). Specifically relevant to this Ph+ MPAL case, the BCR-ABL1-driven tyrosine kinase activity is known to disrupt neutrophil functional capacities, including chemotaxis, oxidative burst, and phagocytosis (42, 43). Furthermore, the leukemic blasts in MPAL exhibit aberrant differentiation that disrupts normal hematopoiesis, leading to both quantitative and qualitative defects in innate immune cells (44). This intrinsic immune compromise is further exacerbated by intensive induction chemotherapy, particularly anthracycline-based regimens. Anthracyclines (such as daunorubicin) not only cause profound myelosuppression but also induce mucosal barrier injury and impair tissue-resident macrophage function, creating a permissive environment for fungal invasion (45, 46). The combination of these factors—the underlying immune dysfunction from BCR-ABL1 signaling, treatment-related immunosuppression, and mucosal barrier breakdown—creates a perfect storm for opportunistic fungal infections, necessitating robust antifungal prophylaxis strategies.
In hematological oncology regimens, voriconazole is a widely used empirical prophylactic broad-spectrum fungicide that potently inhibits Candida, Aspergillus, Scedosporium, and Fusarium, reducing the risk of invasive fungal infection in immunocompromised patients (47). However, there is evidence that voriconazole inhibition of Aspergillus creates a favourable environment for Mucorales (12, 22), associated with increased mucormycosis, and animal studies have suggested that exposure to voriconazole enhances Mucorales virulence (48). Our case provides a notable exception to the conventional management paradigm of ROCM, which emphasizes the necessity of combined surgical and medical therapy. The successful control of infection with L-AmB monotherapy, in contrast to the high surgical intervention rate observed in the literature review, warrants further analysis. We postulate that this favorable outcome is attributable not merely to the “timely adjustment” of antifungal therapy, but more fundamentally to the exceptionally early stage and superficial localization of the infection at the time of diagnosis. The patient’s initial presentation was limited to cutaneous involvement on the nasal dorsum without clinical or radiological evidence of sinusitis, osteomyelitis, or orbital/central nervous system invasion—a finding corroborated by the negative chest CT. This confined disease extent stands in stark contrast to most reported cases of ROCM in leukemic patients, which typically present with advanced sino-orbital or cerebral involvement necessitating aggressive debridement to remove necrotic, avascular tissue and reduce the fungal burden. According to the IDSA guidelines, L-AmB is strongly recommended as first-line treatment, while intravenous isavuconazole or the delayed-release posaconazole tablets are moderately recommended (49). Among them, posaconazole has emerged as the prophylactic agent of choice due to its reliable activity against Mucorales.
As observed in the current case, ROCM infection usually originates from the paranasal sinuses, with bone destruction and subsequent invasion of the orbit, eye, and brain (50). Unilateral facial edema, proptosis, and palatal or palpebral fistula developing into necrosis may be observed. When invasive fungal infection is suspected, particularly in cases of ROCM involvement, a diagnostic paradigm shift is warranted. Rather than relying on serum biomarkers such as galactomannan testing, which demonstrates poor sensitivity for mucormycosis, immediate tissue-based diagnostic approaches should be prioritized (51). Early and aggressive tissue sampling for histopathological examination, coupled with molecular diagnostics and fungal culture, is crucial for several reasons: (1) it allows definitive identification of Mucorales through characteristic histological features (broad, pauciseptate hyphae with right-angle branching); (2) enables timely differentiation from other invasive molds like Aspergillus; and (3) provides material for antifungal susceptibility testing. This diagnostic strategy is particularly critical in Ph+ MPAL patients, where delayed diagnosis of mucormycosis carries catastrophic consequences due to their profound immunosuppression and the infection’s characteristically aggressive course. This case emphasizes the need for high clinical suspicion in immunocompromised patients.
Conclusion
5
Mucormycosis is a rare but life-threatening infection in immunocompromised patients, particularly those with hematological malignancies. Early diagnosis and prompt treatment with L-AmB are crucial for improving outcomes. This case underscores the importance of vigilant monitoring and tailored antifungal therapy in managing mucormycosis in Ph+ MPAL patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pham D Howard-Jones AR Sparks R Stefani M Sivalingam V Halliday CL. Epidemiology, modern diagnostics, and the management of Mucorales infections. J Fungi. (2023) 9:659. doi: 10.3390/jof 9060659, PMID: 37367595 PMC 10304757 · doi ↗ · pubmed ↗
- 2Hussain MK Ahmed S Khan A Siddiqui AJ Khatoon S Jahan S. Mucormycosis: a hidden mystery of fungal infection, possible diagnosis, treatment and development of new therapeutic agents. Eur J Med Chem. (2023) 246:115010. doi: 10.1016/j.ejmech.2022.115010, PMID: 36566630 PMC 9734071 · doi ↗ · pubmed ↗
- 3Sharma A Alam MA Dhoundiyal S Sharma PK. Review on mucormycosis: pathogenesis, epidemiology, microbiology and diagnosis. Infect Disord Drug Targets. (2024) 24:e 220823220209. doi: 10.2174/1871526523666230822154407, PMID: 37608614 · doi ↗ · pubmed ↗
- 4Lynch JP Fishbein MC Abtin F Zhanel GG. Part 1: Mucormycosis: prevalence, risk factors, clinical features, and diagnosis. Expert Rev Anti Infect Ther. (2023) 21:723–36. doi: 10.1080/14787210.2023.2220964, PMID: 37262298 · doi ↗ · pubmed ↗
- 5Jeong W Keighley C Wolfe R Lee WL Slavin MA Kong DCM. The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin Microbiol Infect. (2019) 25:26–34. doi: 10.1016/j.cmi.2018.07.011, PMID: 30036666 · doi ↗ · pubmed ↗
- 6Prakash H Chakrabarti A. Epidemiology of mucormycosis in India. Microorganisms. (2021) 9:523. doi: 10.3390/microorganisms 9030523, PMID: 33806386 PMC 8000977 · doi ↗ · pubmed ↗
- 7Hallur V Prakash H Sable M Preetam C Purushotham P Senapati R. Cunninghamella arunalokei a new species of Cunninghamella from India causing disease in an immunocompetent individual. J Fungi. (2021) 7:670. doi: 10.3390/jof 7080670, PMID: 34436209 PMC 8401845 · doi ↗ · pubmed ↗
- 8Alqarihi A Kontoyiannis DP Ibrahim AS. Mucormycosis in 2023: an update on pathogenesis and management. Front Cell Infect Microbiol. (2023) 13:1254919. doi: 10.3389/fcimb.2023.1254919, PMID: 37808914 PMC 10552646 · doi ↗ · pubmed ↗