The Role of Mechanical Economy and Efficiency as Key Drivers of Cardiac Rehabilitation Exercise Performance Improvement in a Patient With Heart Failure and an Implanted CRT‐D: A Case Report and Literature Review
Javier Loureiro Diaz, Praveen Jayaprabha Surendran, Prasobh Jacob, Salma Chbib, Amine Ghram, Liam David Foster, Omar Ibrahim

TL;DR
A heart failure patient showed significant improvements in mechanical efficiency during cardiac rehab, beyond what traditional measures like oxygen consumption suggest.
Contribution
This case report highlights the importance of measuring mechanical economy and efficiency in assessing cardiac rehabilitation outcomes in heart failure patients.
Findings
Peak workload improved by 61% while peak oxygen consumption increased only by 9%.
Mechanical economy and efficiency improved significantly at all physiological thresholds.
Improvements in mechanical efficiency reveal greater external work for metabolic cost in heart failure patients.
Abstract
Heart failure with reduced ejection fraction leads to exercise intolerance due to central and peripheral dysfunction. Improvements in exercise performance are not fully captured by traditional measures like peak oxygen consumption alone. A 57‐year‐old male with a complex cardiac medical history of hypertrophic cardiomyopathy with left ventricle non‐compaction, Wolff‐Parkinson‐White syndrome, transient ischemic stroke, and heart failure with reduced ejection fraction with an implanted cardiac resynchronization therapy defibrillator underwent cardiac rehabilitation. Cardiopulmonary exercise testing revealed a non‐proportional improvement in peak oxygen consumption (0.3 METs, 9%) versus peak workload (48 W, 61%). Gross mechanical economy and efficiency improved at all physiological thresholds: at ventilatory threshold by 11%, at respiratory compensation point by 60% and 41%, and at peak…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
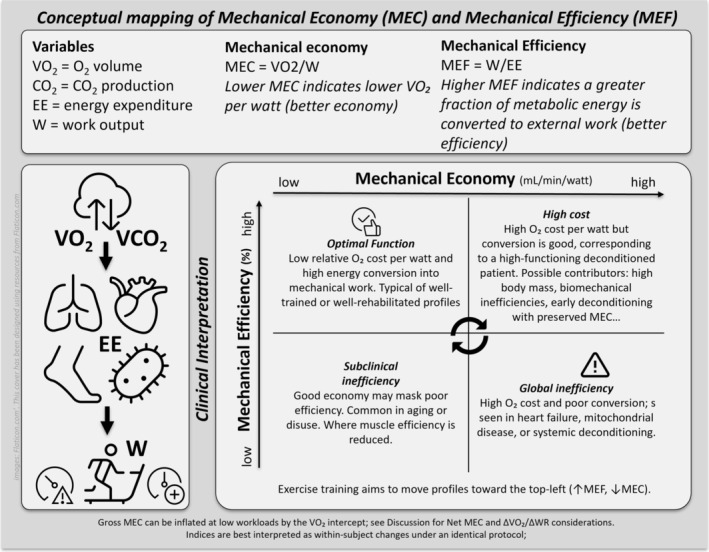 FIGURE 1
FIGURE 1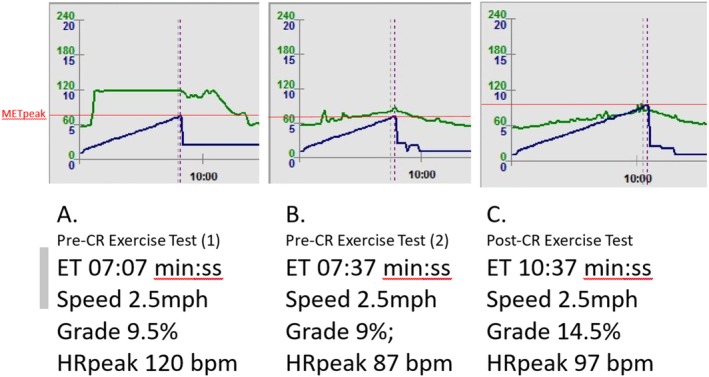 FIGURE 2
FIGURE 2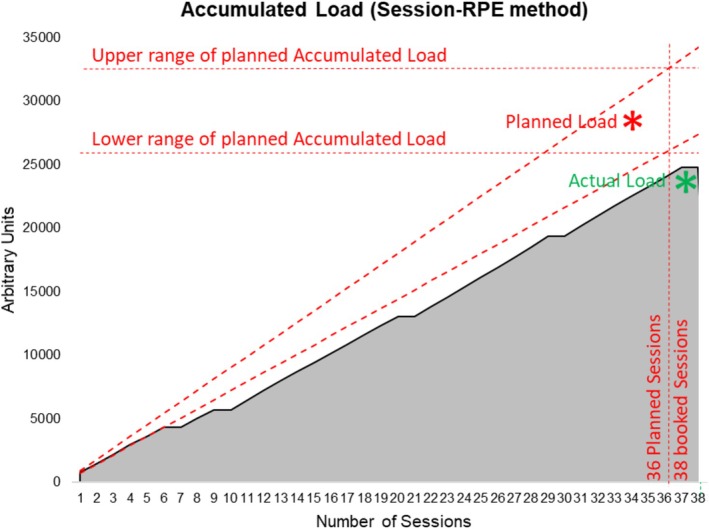 FIGURE 3
FIGURE 3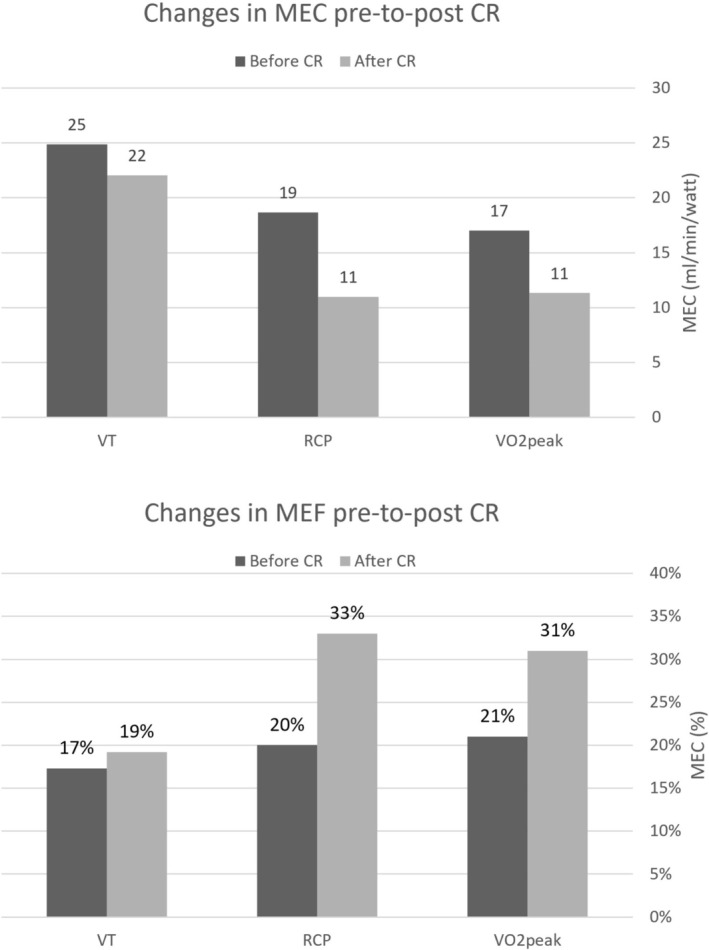 FIGURE 4
FIGURE 4| Variable | Before‐CR | After‐CR | Net change | Delta change (%) | |
|---|---|---|---|---|---|
| Ventilatory threshold | VT | 10.9 | 12 | 1.10 | 10.1 |
| VT workload [W] [watts] | 35 | 44 | 9.00 | 25.7 | |
| VT Power‐to‐weight ratio [watts/kg] | 0.50 | 0.62 | 0.12 | 24 | |
| VT Mechanical efficiency (W/EE) | 17.3% | 19.2% | 0.02 | 10.9 | |
| VT Mechanical economy ( | 24.89 | 22.07 | −2.82 | −11.3 | |
| Respiratory compensation point | RCP | 14.2 | 16 | 1.80 | 12.7 |
| RCP workload [W] [watts] | 61 | 118 | 57.00 | 93.4 | |
| RCP power‐to‐weight ratio [watts/kg] | 0.87 | 1.66 | 0.79 | 90 | |
| RCP Mechanical efficiency (W/EE) | 20% | 33% | 0.12 | 60.7 | |
| RCP Mechanical economy ( | 18.67 | 11.00 | −7.67 | −41.1 | |
|
| Peak exercise time [s] | 457.00 | 638.00 | 181.00 | 39.6 |
|
| 16.6 | 17.6 | 1.00 | 6.0 | |
| Peak % | 52% | 56% | 0.04 | 7.7 | |
| Peak workload (W) [watts] | 78 | 126 | 48.00 | 61.5 | |
| Peak power‐to‐weight ratio [watts/kg] | 1.11 | 1.77 | 0.66 | 59 | |
| RER | 1.08 | 1.10 | 0.02 | 1.9 | |
| Peak mechanical efficiency (W/EE) | 21% | 31% | 0.10 | 47.3 | |
| Peak mechanical economy ( | 17.03 | 11.33 | −5.70 | −33.5 |
- —Universidade da Coruña10.13039/501100014597
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiovascular Function and Risk Factors · Cardiovascular and exercise physiology
Summary
- Mechanical economy and mechanical efficiency offer a plausible hypothesis to the discrepancy between peak workload change and the change in peak oxygen consumption pre‐to‐post cardiac rehabilitation in heart failure patients.
- Both assess indirectly physiological changes from exercise interventions that may not be captured by traditional parameters such as peak oxygen consumption alone.
Introduction
1
Heart failure with reduced ejection fraction (HFrEF) is characterized by a reduced ability of the heart to pump blood effectively, leading to exercise intolerance [1]. Peripheral changes due to poor perfusion among other factors result in a reduction in skeletal muscle mass and contractile function, and an increased oxygen cost of force generation, leading to early fatigue and exercise intolerance [1, 2, 3]. Overall, HFrEF results in decreased quality of life, increased hospital readmissions, and increased morbidity and mortality [1, 2, 4, 5].
Exercise is a core component of cardiac rehabilitation (CR) and is a well‐established therapy for patients with HFrEF (Class 1‐A recommendation) [6, 7]. CR lowers the risk of readmission and mortality, and can improve symptoms and quality of life [2, 5]. These benefits are greatly attributed to the improvement in exercise capacity [5, 8].
Cardiac resynchronization therapy defibrillator (CRT‐D) is a cardiac implantable electronic device used in the treatment of cardiac arrhythmias. CRT‐D improves symptoms and health‐related quality of life [8], reduces the incidence of sudden cardiac death [9, 10], and lowers the risk of mortality and hospital readmission [11, 12, 13, 14] in patients with heart failure. Patients with CRT‐D engaged in CR may also experience improvements in exercise capacity, left ventricular dimensions, and ejection fraction measured by echocardiography [15].
Cardiopulmonary exercise testing (CPET) is the gold standard of measuring peak oxygen consumption (VO_2peak_) and assessing exercise performance [16]. It provides in‐depth information about the cardiopulmonary responses to exercise, the mechanisms of exercise limitation, and the effects of exercise training in patients with HFrEF [17, 18].
Mechanical economy (MEC) and mechanical efficiency (MEF) are both measures of how efficiently the human body converts metabolic energy into mechanical work (W) [19]. They are related but distinct concepts in exercise physiology (Figure 1). MEC is essentially the ratio of energy input needed during exercise (i.e., oxygen consumption) to produce external W. MEC can indirectly be inferred by the relationship VO_2_/W [20]. MEF is a measure of how efficiently the body can produce W for a given amount of energy expenditure (EE). EE can be derived from gas analysis during CPET [21, 22]. MEF (W/EE) is considered a measure of how effectively an individual converts EE into W [23]. A lower MEF may indicate a higher energy cost during exercise or that more energy is inefficiently used or wasted.
Conceptual mapping of mechanical economy (MEC) and mechanical efficiency (MEF) with clinical phenotypes and their clinical interpretation. EE, energy expenditure; MEC, mechanical economy (VO2/W; mL·min−1·W−1); MEF, mechanical efficiency (gross, W/EE × 100, %); VCO₂, carbon dioxide output; VO2, oxygen uptake; W, external work (Watts); ΔVO2/ΔWR, slope of oxygen uptake versus work‐rate (mL·min−1·W−1).
MEC and MEF are well‐described in the context of exercise physiology and sport performance; however, their integration into CR reports is limited. We applied both variables as primary outcome indicators after individualized rehabilitation to highlight their clinical utility in characterizing submaximal improvements and cardiorespiratory‐muscular adaptations. HFrEF‐related physiological changes can lead to a worsening of both MEC and MEF, resulting in early fatigue and exercise intolerance. Improving MEC and MEF can reduce the metabolic cost of exercise, allowing patients to perform more work with less oxygen cost and/or less EE [1, 20, 24]. This can lead to enhanced functional capacity, reduced symptoms, and improved quality of life [5, 25, 26]. The effects of CR exercise training on MEC and MEF in coronary artery disease patients have been studied [24], but MEC and MEF are underexplored in HFrEF.
This case report highlights MEC and MEF for the detection of physiological dysfunction and the assessment of physiological adaptations in response to training in a HFrEF patient with a CRT‐D in DDD mode during treadmill exercise. CARE guidelines were used to report this case.
Case History/Examination
2
A 57‐year‐old male with a history of HFrEF (left ventricular ejection fraction 28%), hypertension, smoker with an 18 pack‐year history, chronic kidney disease, and a prior transient ischemic stroke was referred for outpatient CR. His cardiac history included hypertrophic cardiomyopathy with left ventricle non‐compaction, Wolff‐Parkinson‐White syndrome treated with ablation, and an implantable cardioverter defibrillator, later upgraded to CRT‐D in DDDR rate responsive mode. The patient presented in New York Heart Association functional class II and reported total avoidance of physical activity due to concerns about exercise safety. His medical treatment included Amiodarone 200 mg, once daily; Bisoprolol 3.75 mg, once daily; Sacubitril/Valsartan 100 mg, bis in die; Furosemide 80 and 40 mg, bis in die; Spironolactone 25 mg, once daily; Atorvastatin 20 mg, once daily; Warfarin adjusted based on INR readings; Ferrous Fumarate 200 mg, once daily; Ergocalciferol 50,000 units, once weekly; and Pantoprazole 40 mg, once daily.
Differential Diagnosis
3
Treadmill exercise testing is the preferred testing modality in patients with rate response devices [27]. Initially, a 12‐lead electrocardiographically monitored treadmill ramp protocol was performed to assess heart rate response to exercise with CRT‐D in DDDR mode. CRT‐D was working too aggressively for the patient, with minimal change in heart rate response (Image A in Figure 2). The patient also reported exercise‐related fatigue and breathlessness out of proportion to the workload, despite optimal medical therapy.
Heart rate and increasing workload during exercise testing with CRT‐D on DDDR versus DDD mode. bpm, beats per minute; CR, cardiac rehabilitation; ET, exercise time; HRpeak, peak heart rate; MET, metabolic equivalent of task; min:ss; minutes and seconds; MPH, miles per hour.
This device's response can be mostly attributed to chronotropic incompetence and inappropriate sensor function for rate‐adaptive pacing (under or over responsive) [27]. If ventricular pacing is needed or desired, the device should be programmed to at least track the maximum sinus rate reached during exercise. However, there is still much controversy about the effectiveness of rate‐responsive devices, especially in patients diagnosed with heart failure. As no deleterious effects have been described, the rate response feature can probably be programmed on or off safely. Device interrogation showed minimal heart rate fluctuations during daily activity suggesting the rate‐responsive algorithm may have been insufficiently adapting to physiological needs or even contributing to dysynchrony. Following multidisciplinary discussion with the electrophysiology team, the CRT‐D was reprogrammed to DDD mode to allow for the patient's own intrinsic increase in heart rate to meet the exercise demand. The aim was to optimize ventricular synchrony by maintaining a consistent, optimal delay between sensed or paced atrial and ventricular events, minimizing beats that disrupt effective resynchronization and cardiac output under controlled pacing conditions. This approach is especially relevant in heart failure patients where electromechanical synchrony is critical for both ventricles to be reliably paced together for functional recovery and exercise tolerance.
The patient was scheduled for a follow‐up CPET with the CRT‐D on DDD mode. Heart rate response was reduced, but it progressively and continuously increased with workload (Image B in Figure 2). VO_2peak_ was measured at 15.0 mL/min/kg (47% of age‐predicted) [19] equivalent to 4.3 Metabolic Equivalent of Task (MET) [28].
The patient was stratified as high‐risk for cardiac events during exercise according to the American Association of Cardiovascular Prevention and Rehabilitation [29]. The exercise intervention was programmed based on the CPET results and available guidelines [30, 31]. Exercise targets for heart rate and rate of perceived exertion (RPE) were set based on the ventilatory threshold and the respiratory compensation point (Table 1).
Progressive overload is a staple of the training process [26, 32]. We evaluated all patients' subjective and objective responses to each workload after each rehabilitation day to confirm they were within prescribed ranges [33]. If needed, the clinical team revised the exercise target heart rate and RPE, and external workloads were adjusted to bring both within prescribed range in the next session. The patient attended 33 outpatient hospital‐based CR exercise sessions with 87% completed as planned. Exercise target heart rate and Session‐RPE targets were met on 94% of sessions. All sessions lasted for the planned duration. Average exercise frequency was 2.6 sessions/week. Exercise training volume quantification was based on the Session‐RPE method [33, 34, 35]. Median daily exercise volume was 720 arbitrary units, and total accumulated training volume was 23,280 arbitrary units (Figure 3).
Accumulated load of supervised exercise training across cardiac rehabilitation based on the session‐RPE method.
Conclussion and Results
4
Pre‐to‐post CR, there was a +9% change in VO_2peak_ (1 mL/kg/min, 0.3 MET) and a 61% change in W peak (48 W) (Table 1). These can be explained by the improvements in MEC and MEF as underlying physiological determinants of VO_2peak_ (Figures 1 and 4). These results highlight the role of peripheral adaptations as a significant driver of exercise performance in patients with HFrEF and CRT‐D, which is clinically relevant and consistent with the evidence. By understanding the concepts of MEC and MEF, clinicians can gain a more accurate assessment of an individual's ability to convert metabolic energy into mechanical work, offering a plausible hypothesis for the commonly seen discrepancy between VO_2peak_ and W peak changes. Incorporating MEC and MEF into clinical assessments can guide the development of more targeted interventions in patients with HFrEF with a CRT‐D, and therefore MEC and MEF should be routinely measured and reported for assessing rehabilitation outcomes.
Mechanical economy and mechanical efficiency changes during cardiopulmonary exercise testing ventilatory thresholds before and after cardiac rehabilitation. CR, cardiac rehabilitation; MEC, mechanical economy; MEF, mechanical efficiency; RCP, respiratory compensation point; VO2, oxygen consumption; VT, ventilatory threshold.
Discussion
5
VO_2peak_ reflects the maximal capacity of the cardiopulmonary system to transport and utilize oxygen during exercise [36]. Absolute VO_2peak_ was minimally improved by 0.3 MET (+9%). In HFrEF, VO_2peak_ is a strong predictor of mortality, and there is a mortality reduction of 19% with every +1 MET [37]. Every 6% increase in VO_2peak_, adjusted for other significant predictors, has also been associated in heart failure with a 5% lower risk of time to all‐cause mortality or all‐cause hospitalization; a 4% lower risk of cardiovascular mortality or cardiovascular hospitalization; and an 8% lower risk of heart failure‐related mortality or hospitalization.
W peak was disproportionately increased (+61%) pre–post CR when compared to VO_2peak_ (+9%) (Table 1). This apparently disproportionate increase is not uncommon after CR. Although there is a correlation between VO_2peak_ and W peak, the relationship between both can vary depending on the individual and the exercise test protocol. Overall effect sizes for all physiological determinants of exercise performance have not been determined. It is therefore not possible to attribute a conversion rate between a percentage or unit increment in VO_2peak_ and an increase in W peak.
Patients diagnosed with HFrEF typically have reduced systolic volume and a reduced ability to increase their heart rate [38]. This limits their ability to increase cardiac output during exercise. Oxygen pulse (oxygen consumption divided by heart rate) is a limited surrogate measure of the systolic volume and a sensitive marker of abnormalities in the cardiovascular system [16, 39]. Systolic volume can improve with exercise by improving cardiac filling and reducing afterload through improvements in peripheral vascular resistance. Improved vasodilation is critical in patients with HFrEF, as it allows for greater blood flow to the working muscles and improved oxygen delivery. Exercise training can induce this adaptation by improving endothelial function and reducing vascular resistance. It may also improve cardiac contractility, allowing greater force generation by improving calcium handling and increasing the sensitivity of the contractile proteins to calcium [40]. In this case report, oxygen pulse increased by 6%, heart rate peak increased by 11%, and chronotropic index increased by 43% to reach normal range [41].
Peripheral dysfunction can be caused by decreased mitochondrial density, altered fiber type, impaired oxygen delivery, increased oxidative stress, and overall, a decreased contractile efficiency and increased oxygen cost of force generation. Exercise training can improve peripheral function by inducing favorable adaptations in all these factors, leading to improved oxygen extraction and utilization during exercise. This results in increased exercise capacity, more efficient use of energy resources, and decreased fatigue. These adaptations can be indirectly assessed through MEC and MEF during CPET [42].
MEC and MEF during cycling are more uniform between individuals when compared to treadmill exercise [19, 30, 31]. MEF during treadmill is known to vary more significantly due to differences in gait patterns, body weight, and metabolic condition. Despite this variability, treadmill testing was selected over cycling in this case report to accommodate the patient's CRT‐D pacing mode, which is more reliably assessed during upright exercise.
Measuring Mechanical Efficiency During Treadmill Exercise
5.1
MEF can be measured as the ratio of W to EE, expressed as a percentage. EE was computed using the formula [43] E = (4.94 × RER + 16.04) × (VO_2net_, in mL/min) × 60–1. Net oxygen uptake was determined by subtracting resting VO_2_ from total VO_2_. MEF was calculated in net terms using the following formula [44]: MEF = (W/EE) × 100 − 1.
To calculate W in watts on a treadmill exercise, it is necessary to account for the force exerted by the person, dependent on the velocity at which they are moving, as well as how much of the force is being used to overcome the elevation (expressed either as a percentage slope or converted to an angle) and the gravitational constant (9.81 m/s^2^). This force is primarily determined by the person's weight acting against gravity due to the treadmill's incline, calculated using F = m·g·sin(θ), where m is the patient's mass, g is the gravitational constant, and sin(θ) is the incline angle of the treadmill. Additionally, to the power required to overcome the incline, the horizontal component of treadmill walking should also account for some energy expended to maintain forward motion. This could be factored into the equation by adding a small rolling resistance coefficient, which, for activities like walking on a treadmill, is considered negligible. These equations theoretically provide a broad explanation of how metabolic energy is efficiently converted into mechanical work within the human biomechanical system.
Measuring Mechanical Economy During Treadmill Exercise
5.2
MEC can be derived during a CPET as the ratio VO_2_/W. It provides a simple surrogate way to quantify how an individual is using oxygen to produce power. A lower VO_2_/W ratio may indicate that the individual can produce more W for a given amount of oxygen consumed, suggesting better MEC. Nonetheless, there are some limitations for the use of VO_2_/W, as it is an indirect measure best used for analyzing constant workload steady‐state exercise. VO_2_/W infers MEC based on metabolic and mechanical parameters, but gait, muscle fiber type, and training status can affect the relationship between VO_2_ and W.
In the present report, MEC is expressed as the gross point estimate of oxygen cost (VO_2_/W). Because gross VO_2_/W includes the resting or unloaded oxygen uptake, gross MEC may overestimate oxygen cost at low workloads. Alternative approaches in MEC calculations in cycling literature include net MEC, defined as (VO_2_ − VO_2__0‐W)/W, and the ΔVO_2_/ΔWR slope. This slope is calculated across the sub‐threshold linear portion of the test, describing the gain of VO_2_ with respect to work rate, and is less sensitive to early and late stage nonlinearity [19]. These alternatives may reduce intercept bias. When interpreting the gross VO_2_/W ratios, it should be noted that net MEC or ΔVO_2_/ΔW may also yield lower absolute MEC values, although the directional inference in this case would be unchanged. Treadmill test MEC and MEF exhibit greater inter‐individual variability than cycling due to gait and body mass, and results can depend on speed, grade, and stage structure [19, 20]. Indices in this report are best interpreted as within‐subject change under an identical protocol.
Measuring Mechanical Efficiency and Economy at Ventilatory Thresholds
5.3
We assessed MEC and MEF at the first ventilatory threshold, the respiratory compensation point, and VO_2peak_ (Table 1). The percentage change in MEC and MEF pre‐ to post‐intervention was calculated using the formula: for example: [(Efficiency post − Efficiency pre)/Efficiency pre] × 100 and presented as a percentage. MEC and MEF demonstrated improvement at all points (Table 1, Figure 4). The magnitude of change is in line with previously reported data [25, 42, 45]. MEF improved more than MEC, consistent with a dominant peripheral adaptation [17, 24].
While genetic factors undoubtedly play a significant role, exercise training quality and quantity can influence various aspects such as shifting muscle fiber type, better substrate utilization due to increased cardiorespiratory efficiency (related to VO_2max_, heart rate, and minute ventilation), biomechanical efficiency (kinematics, kinetics, flexibility), and neuromuscular efficiency (including neural signaling, motor programming, force production, and muscle tendon stiffness) [20]. In addition, other factors such as muscle mass, fiber type composition, and neuromuscular adaptations could contribute to MEC and MEF improvements. Previous studies in HFrEF have documented increases in muscle mass and shifts towards more oxidative muscle fibers following exercise training [25]. Sympathetic nerve activity targeting skeletal muscle vasculature is also lower after exercise training; therefore, increasing muscle blood flow during exercise. These changes enhance oxygen extraction and utilization at the muscular level, thereby improving exercise capacity. Future research should incorporate direct measurements of muscle morphology and function to better elucidate the mechanisms underlying MEC and MEF improvements [46, 47].
Medications play a crucial role in managing HFrEF and can significantly influence exercise capacity and performance [48]. There were no changes in the patient's medication, including beta‐blockers, which are known to affect heart rate and exercise tolerance. However, the potential impact of medications on the observed outcomes should be considered when interpreting the results.
Considering this single case report, it is not possible to generalize its findings, establish a cause‐effect relationship, nor to determine the magnitude of the effects. Future research should aim to address these limitations by including larger, more diverse samples to provide a more robust understanding of the effects of exercise on MEC and MEF.
Although the VO_2_‐W relationship during cycle ramp tests is well described, reference ranges for treadmill‐based gross and net MEC and MEF at defined physiological anchors are sparse and method dependent. Differences in modality, protocol, and analysis windows limit cross‐study comparisons. Future work would benefit from standardized treadmill reporting of gross and net MEC and ΔVO_2_/ΔWR, alongside MEF. Studies comparing treadmill versus cycling could further clarify the role of modality‐specific adaptations. Extended follow‐up periods would allow for investigating the long‐term sustainability of the adaptations. Randomized controlled trials with larger samples would be valuable in establishing a clearer cause‐effect relationship between MEC, MEF, and functional capacity in HFrEF. Future work should incorporate echocardiographic and device interrogation data to strengthen the mechanistic interpretation of results.
The findings of this report have high applicability for the clinician when assessing functional capacity changes in HFrEF. This report makes a significant contribution by assessing MEC and MEF as clinically relevant parameters in clinical exercise physiology. This case serves as a methodological foundation for a prospective series to evaluate MEC and MEF in a broader cohort of patients with HFrEF and CRT‐D undergoing CR.
Author Contributions
Javier Loureiro Diaz: conceptualization, data curation, investigation, methodology, project administration, writing – original draft, writing – review and editing. Praveen Jayaprabha Surendran: conceptualization, investigation, writing – original draft, writing – review and editing. Prasobh Jacob: conceptualization, investigation, writing – original draft, writing – review and editing. Salma Chbib: investigation, writing – original draft, writing – review and editing. Amine Ghram: writing – review and editing. Liam David Foster: investigation. Omar Ibrahim: investigation, writing – review and editing.
Ethics Statement
Patient consent was obtained, and the case report was approved by Hamad Medical Corporation Medical Research Council (MRC) protocol ID MRC‐04‐23‐344.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor‐in‐Chief of this journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. G. Del Buono , R. Arena , B. A. Borlaug , et al., “Exercise Intolerance in Patients With Heart Failure,” Journal of the American College of Cardiology 73, no. 17 (2019): 2209–2225, 10.1016/j.jacc.2019.01.072.31047010 · doi ↗ · pubmed ↗
- 2T. Lan , Y. H. Liao , J. Zhang , et al., “Mortality and Readmission Rates After Heart Failure: A Systematic Review and Meta‐Analysis,” Therapeutics and Clinical Risk Management 17 (2021): 1307–1320, 10.2147/TCRM.S 340587.34908840 PMC 8665875 · doi ↗ · pubmed ↗
- 3J. Mc Coy , M. Bates , C. Eggett , et al., “Pathophysiology of Exercise Intolerance in Chronic Diseases: The Role of Diminished Cardiac Performance in Mitochondrial and Heart Failure Patients,” Open Heart 4, no. 2 (2017): e 000632, 10.1136/openhrt-2017-000632.28878952 PMC 5574430 · doi ↗ · pubmed ↗
- 4X. Chen , Y. Xin , W. Hu , Y. Zhao , Z. Zhang , and Y. Zhou , “Quality of Life and Outcomes in Heart Failure Patients With Ejection Fractions in Different Ranges,” P Lo S One 14, no. 6 (2019): e 0218983, 10.1371/journal.pone.0218983.31247042 PMC 6597164 · doi ↗ · pubmed ↗
- 5L. Long , I. R. Mordi , C. Bridges , et al., “Exercise‐Based Cardiac Rehabilitation for Adults With Heart Failure,” Cochrane Database of Systematic Reviews 1, no. 1 (2019): CD 003331, 10.1002/14651858.CD 003331.pub 5.30695817 PMC 6492482 · doi ↗ · pubmed ↗
- 6P. Ponikowski , A. A. Voors , S. D. Anker , et al., “2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)developed With the Special Contribution of the Heart Failure Association (HFA) of the ESC,” European Journal of Heart Failure 18 (2016): 891–975.27207191 10.1002/ejhf.592 · doi ↗ · pubmed ↗
- 7C. W. Yancy , M. Jessup , B. Bozkurt , et al., “2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America,” Circulation 136, no. 6 (2017): e 137–e 161, 10.1161/CIR.0000000000000509.28455343 · doi ↗ · pubmed ↗
- 8L. Ye , S. Wang , and L. Wang , “Efficacy and Safety of Exercise Rehabilitation for Heart Failure Patients With Cardiac Resynchronization Therapy: A Systematic Review and Meta‐Analysis,” Frontiers in Physiology 11 (2020): 980, 10.3389/fphys.2020.00980.32973547 PMC 7472379 · doi ↗ · pubmed ↗