Roxadustat for the Treatment of Early Post-Transplantation Anemia
Louis Guenal, Philippe Gatault, Hélène Longuet, Lucie Maigret, Claire Ferran, Leïla Larbi, Alexandre Fillon, Jean-Michel Halimi, Matthias Büchler, Juliette Gueguen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
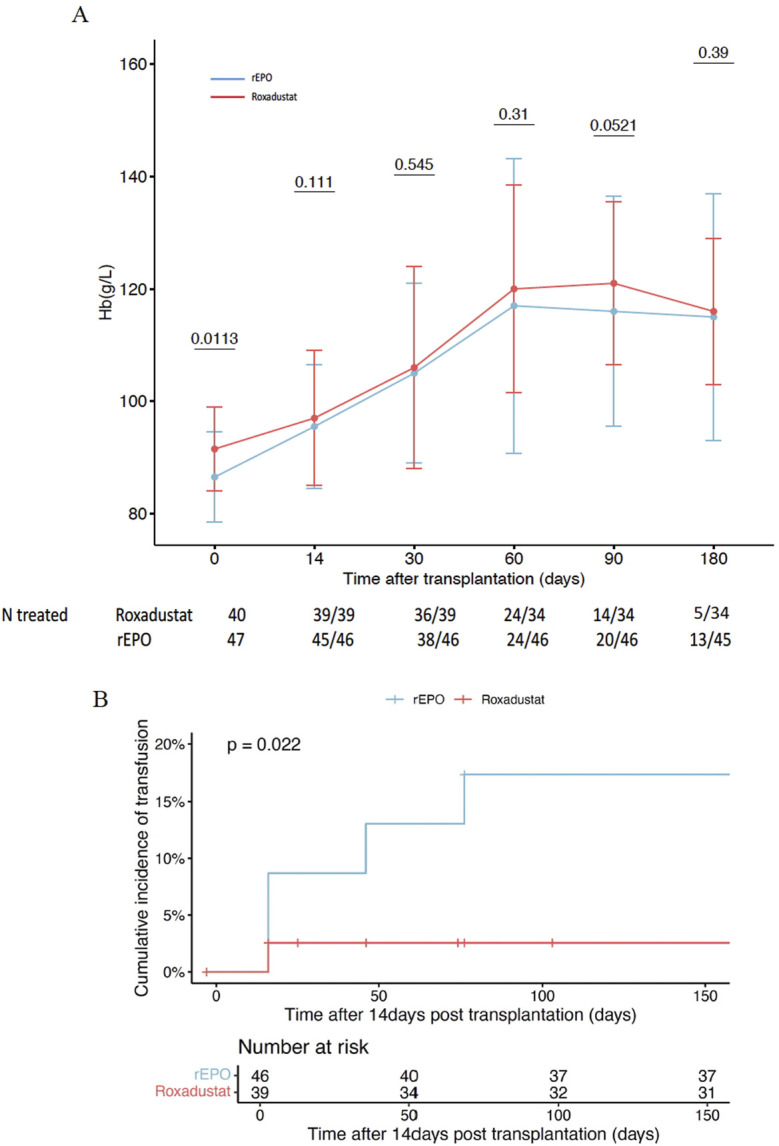 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsErythropoietin and Anemia Treatment · Renal Transplantation Outcomes and Treatments · Hemoglobinopathies and Related Disorders
Dear Editors,
Early post-transplantation anemia (ePTA) is common in kidney transplant recipients (KTRs) and contributes to cardiovascular events, reduced quality of life, and overall mortality [1, 2]. Early PTA is driven by pre-transplant hemoglobin (Hb), preexisting deficiency (iron, folate, vitamin B12), intraoperative bleeding, inflammation, and delayed graft function [1]. Aside from blood transfusions, which should be avoided regarding the risk of developing HLA antibodies, the standard treatment for ePTA includes iron and vitamin supplementation, along with the use of recombinant erythropoietin (rEPO) [3, 4]. However, the efficacy of rEPO in ePTA remains uncertain, frequently observed in case of absolute or functional iron deficiency [1, 4, 5].
Roxadustat is an oral drug recently approved for treating anemia in chronic kidney disease (CKD). However, KTRs were excluded from clinical development studies [6, 7]. Roxadustat belongs to the class of hypoxia-inducible factor prolyl hydroxylase inhibitors (HIF-PHi). By modulating HIF, it exerts pleiotropic effects on the expression of genes involved in EPO synthesis, iron mobilization and inflammation, making it interesting for ePTA [8, 9]. We therefore implemented roxadustat as a routine treatment for ePTA instead of rEPO and report in this letter its efficacy and safety compared with rEPO used in the first month post transplantation.
We enrolled all consecutive patients receiving roxadustat for ePTA (defined as Hb <10g/dL during the first month after transplantation) and estimated glomerular filtration rate <60 mL/min/1.73 m^2^. Control group included all patients transplanted who received rEPO for ePTA during previous year. Data were retrieved from the ASTRE database, which prospectively collects data from KTRs (DR-2015-518). Additional data were adjudicated using medical records: Hb level, glomerular filtration rate, parathyroid hormone, blood transfusions, cardiovascular and thrombotic events, ferritin and transferrin saturation, C-reactive protein, date of treatment initiation, treatment dose and subsequent adjustments, and date of treatment discontinuation. Our protocol prioritizes correction of vitamin and iron deficiencies when indicated. Blood transfusions are performed in patients with Hb <7.5g/dL, or <9g/dL in the presence of symptoms or a history of vascular or cardiac stroke.
Roxadustat and rEPO were prescribed in accordance with the Summaries of Product Characteristics used for CKD. Roxadustat was started at 70 mg three times per week. Darbepoetin alfa was the single rEPO used, initiated at a dose of 0.45 μg/kg/week. In both groups, the dosage was increased in case of inefficacy at 1 month, the dosage was reduced or discontinued if Hb exceeded 12 g/dL or increased by more than 2 g/dL within 14 days. Efficacy was assessed by the proportion of patients achieving the target Hb level (>10 g/dL) and the need for blood transfusions beyond 2 weeks post-transplantation, to exclude the impact of perioperative bleeding. Safety was evaluated over the first 6 months, focusing on the incidence of severe adverse events, including vascular thrombosis, graft loss and major adverse cardiac events (4P-MACE).
Among 163 KTRs between May 2023 and July 2024, 46 received roxadustat for ePTA. Six patients were excluded (5 for early discontinuation of roxadustat unrelated treatment, 1 for concomitant use of rEPO). The prior year, 54 patients received rEPO for ePTA: 7 patients were excluded (5 for receiving fewer than 7 days of treatment, 1 for being under 18 years, 1 for bone marrow disease).
We observe that a greater proportion of patients in the roxadustat group achieved the target Hb of >10 g/dL at 3 months compared to the rEPO group (97% vs. 80% p = 0.04), which coincided with slightly higher Hb levels at that time point (Figure 1A). Moreover, a significantly higher number of patients treated with rEPO received transfusions beyond the first 2 weeks post-transplant (19.6% vs 2.6%, p = 0.02) (Figure 1B). At 6 months, 5 patients (15%) remained treated with roxadustat (28% in the rEPO group, p = 0.16), with a dose between 70 and 150 mg 3 times a week.
Globally, no difference was observed between both groups regarding safety outcomes. In the roxadustat group, 4 patients experienced thrombotic events (1 native kidney vein thrombosis, 2 lower limb deep vein thrombosis, and 1 arteriovenous fistula thrombosis); 2 patients experienced major cardiovascular events and 1 patient lost the graft due to severe artery stenosis leading to arterial thrombosis 6 months post-transplantation. In the rEPO group, 2 patients experienced thrombotic events (one lower limb deep vein thrombosis and one iliac vein thrombosis), no cardiovascular event nor graft loss was observed, 1 patient died from septic shock.
To our knowledge, we report the first European cohort study evaluating the efficacy and safety of roxadustat for the treatment of ePTA in KTRs. In contrast to randomized controlled trials conducted in patients with CKD which demonstrated non-inferiority of roxadustat compared to rEPO, our findings suggest that roxadustat may be more effective during the early post-transplantation period. At 3 months, 97% of patients in roxadustat group achieved the targeted Hb level, maintained at 6 months, with less need for transfusions compared to patients treated with rEPO. While the treatment was generally well tolerated, we call for particular caution regarding thrombotic risk, especially during the first 3 months following initiation. Although no statistically significant difference was observed, we suspect high level or a rapid increase of Hb to be a favoring factor of thrombosis. These adverse events are aligned with the European Medicines Agency’s recommendations for cautious use of roxadustat due to potential cardiovascular and thrombotic risks. These findings underscore the importance of closely monitoring Hb levels, especially at initiation and after each dose adjustment. Of note, 6/36 patients, who presented with persistently impaired graft function, were still receiving roxadustat at 6 months. This observation illustrates that some individuals may have a long-term indication for anemia treatment. It raises the question of long-term safety of roxadustat, particularly concerning its potential pro-angiogenic effects -through VEGF upregulation-in a population with an increased cancer risk. Nevertheless, randomized trials have not demonstrated an increased incidence of cancers, in line with findings from preclinical models [10]. This may be due to an incomplete activation of the HIF pathway, insufficient to trigger the VEGF gene expression and to the inhibition of tumor growth by modifying the microtumoral environment, as suggested by in vitro studies. In our opinion, this theorical risk should warrant vigilant monitoring rather than leading to the exclusion of KTRs.
In conclusion, our study suggests that the use of roxadustat may be more effective than rEPO in the management of ePTA in KTRs. However, its benefit-risk profile warrants further investigations in a randomized controlled trial.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chienwichai K Phirom S Wuttiputhanun T Leelahavanichkul A Townamchai N Avihingsanon Y A Systematic Review and meta-analysis of Factors Contributing to Post-kidney Transplant Anemia and the Effect of erythropoietin-stimulating Agents. Syst Rev (2024) 13(1):278. 10.1186/s 13643-024-02709-8 39533400 PMC 11556001 · doi ↗ · pubmed ↗
- 2Rigatto C Parfrey P Foley R Negrijn C Tribula C Jeffery J. Congestive Heart Failure in Renal Transplant Recipients: Risk Factors, Outcomes, and Relationship with Ischemic Heart Disease. J Am Soc Nephrol JASN (2002) 13(4):1084–90. 10.1681/ASN.V 1341084 11912270 · doi ↗ · pubmed ↗
- 3Ferrandiz I Congy-Jolivet N Bello AD Debiol B Trébern-Launay K Esposito L Impact of Early Blood Transfusion After Kidney Transplantation on the Incidence of Donor-specific Anti-HLA Antibodies. Am J Transpl (2016) 16(9):2661–9. 10.1111/ajt.13795 26998676 · doi ↗ · pubmed ↗
- 4Portoles J Crespo M Martínez BM Martínez Morales E Calatayud Aristoy E Mora Lopez P Post-Transplant Renal Anemia: A Call to Action from a National Study in Routine Clinical Practice. Clin Kidney J (2024) 17(10):sfae 269. 10.1093/ckj/sfae 269 39372236 PMC 11450472 · doi ↗ · pubmed ↗
- 5Jiménez C González E Marqués M Galeano C Andrés A Calvo N The Impact of Darbepoetin Alfa in Early Post-transplant Anaemia Management: Retrospective Exploratory Study. Nefrol Engl Ed (2013) 33(1):107–15. 10.3265/Nefrologia.pre 2012.Oct.11473 23364633 · doi ↗ · pubmed ↗
- 6Chen N Hao C Peng X Lin H Yin A Hao L Roxadustat for Anemia in Patients with Kidney Disease Not Receiving Dialysis. N Engl J Med (2019) 381(11):1001–10. 10.1056/NEJ Moa 1813599 31340089 · doi ↗ · pubmed ↗
- 7Barratt J Andric B Tataradze A Schömig M Reusch M Valluri U Roxadustat for the Treatment of Anaemia in Chronic Kidney Disease Patients Not on Dialysis: A Phase 3, Randomized, Open-Label, Active-Controlled Study (DOLOMITES). Nephrol Dial Transpl Off Publ Eur Dial Transpl Assoc - Eur Ren Assoc. (2021) 36(9):1616–28. 10.1093/ndt/gfab 191 34077510 PMC 8396401 · doi ↗ · pubmed ↗
- 8Li H Hu SM Li YM Ciancio G Tadros NN Tao Y Beneficial Effect of Roxadustat on Early Posttransplant Anemia and Iron Utilization in Kidney Transplant Recipients: A Retrospective Comparative Cohort Study. Ann Transl Med (2022) 10(24):1360. 10.21037/atm-22-5897 36660711 PMC 9843359 · doi ↗ · pubmed ↗