Daratumumab for CD20 − CD38 + Relapsed/Refractory Diffuse Large B‐Cell Lymphoma
ZeTong Hong, ZhaoYang Hong, YaXian Ma, Qing Yin, Min Liu, Wei Huang, KuangGuo Zhou, Dan Li, TongJuan Li, Miao Zheng

TL;DR
Daratumumab combination therapy shows promise for treating CD20−CD38+ relapsed/refractory diffuse large B-cell lymphoma and may help bridge to CAR-T therapy.
Contribution
Demonstrates Daratumumab's potential as an effective treatment and bridge to CAR-T in CD20−CD38+ R/R DLBCL patients.
Findings
Four CD20−CD38+ R/R DLBCL patients showed remission with Daratumumab combination therapy.
1-year OS rate was 75%, with moderate and reversible adverse effects.
Daratumumab therapy successfully transitioned two patients to CAR-T therapy.
Abstract
Patients with R/R DLBCL (relapsed/refractory diffuse large B‐cell lymphoma) treated with rituximab‐based regimens often have a reduction in the expression level of CD20. Replacement of target proteins for new targeted chemotherapy has become a popular direction for the treatment of R/R DLBCL. To investigate whether Daratumumab can be an effective alternative to targeted agents as monotherapy or combination chemotherapy in patients with CD20‐CD38+ R/R DLBCL who have failed to respond to CD20 monoclonal antibody treatment and its adjuvant effect on subsequent CAR‐T (chimeric antigen receptor T‐cell immunotherapy). A total of four CD20‐CD38+ R/R DLBCL patients treated with multiple lines of Daratumumab‐based combination chemotherapy were retrospectively collected. For eligible patients, CAR‐T therapy was used afterwards. Also, the authors successfully constructed allografted tumour models…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
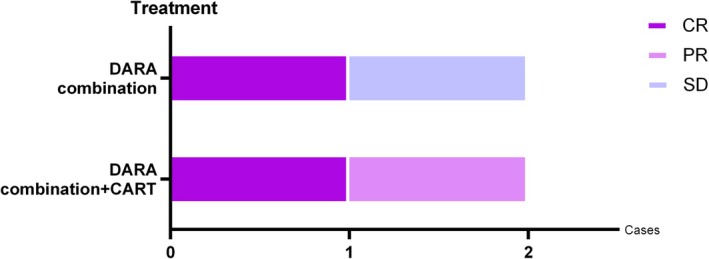 FIGURE 1
FIGURE 1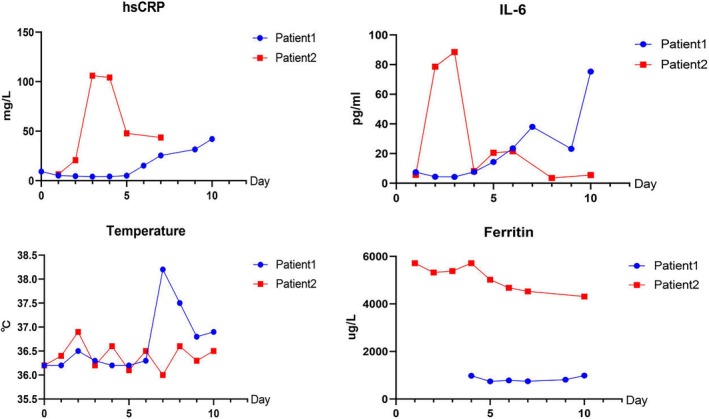 FIGURE 2
FIGURE 2| Baseline characteristics | |
|---|---|
| Characteristic | |
| Number | 4 |
| Gender | |
| Male | 1 (25%) |
| Female | 3 (75%) |
| Age | |
| Median | 50.5 |
| < 60 no. (%) | 3 (75%) |
| ≥ 60 years no. (%) | 1 (25%) |
| Ann Arbor stage | |
| I–II | 0 (0%) |
| III–IV | 4 (100%) |
| IPI | |
| 0–1 | 0 (0%) |
| 2–4 | 4 (100%) |
| Prior therapies | |
| Median (range) lines | 4 |
| Preline therapies > 3 | 4 (100%) |
| Involvement outside of lymphnodes | |
| No | 0 (0%) |
| Yes | 4 (100%) |
| Pretreatment disease burden | |
| Bone marrow involvement | 4 (100%) |
| Double hit | 1 (25%) |
| HSCT pretherapy | 1 (25%) |
| No. | Targets evaluation | Treatment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CD20 | CD19 | CD38 | CD22 | Dara cycles | Combination drug | CART therapy | CD19 (*10^6/kg) | CD22 (*10^6/kg) | CRS level | |
| No. 1 | − | + | + | + | 3 | Orelabrutinib, Selinexor | Yes | 2.5 | 0.5 | 1 |
| No. 2 | − | + | + | + | 4 | Venetoclax, Gemox | Yes | 0.5 | / | 1 |
| No. 3 | − | + | + | + | 3 | Orelabrutinib | No | / | / | / |
| No. 4 | − | + | + | − | 5 | Cytarabine, ICE, DA‐EPOCH | No | / | / | / |
- —Natural Science Foundation of Hubei Province10.13039/501100003819
- —National Natural Science Foundation of China10.13039/501100001809
- —Beijing Xisike Clinical Oncology Research Foundation10.13039/100018904
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Silicon Carbide Semiconductor Technologies · Lymphoma Diagnosis and Treatment
Introduction
1
Diffuse large B‐cell lymphoma is a highly aggressive non‐Hodgkin lymphoma. At present, the standard first‐line treatment is Rituximab targeting CD20. About 30%–40% of patients will progress to R/R DLBCL, among which 60% have a downregulation in CD20 with insensitivity to rituximab treatment. Salvage treatment includes replacement of chemotherapy (DA‐EPOACH, etc.) or HSCT (Haematopoietic Stem‐Cell Transplantation). The prognosis of patients is still poor: the 3‐year OS rate is 38%–50%, the 3‐year PFS rate is 29%–37%. Therefore, for R/R DLBCL with downregulation of CD20, the replacement of therapeutic targets has become a major direction of clinical research. At present, Polatuzumab targeting CD79b, Tafasitamab targeting CD19 [1] and Daratumumab targeting CD38 have entered clinical trials [2].
CD38 is a glycoprotein located on the cell membrane. It has been reported that the expression of CD38 in most malignant blood tumour cells is much higher than in normal cells, including WM, ALL, AML and various types of B‐cell lymphomas [2, 3, 4, 5, 6, 7]. Importantly, CD38 is not expressed by multipotent haematopoietic stem cells, which are essential for long‐term bone marrow recovery [8]. These make CD38 an attractiv.e therapeutic target for R/R DLBCL.
Daratumumab is a CD38 monoclonal antibody approved as regimens for patients with MM who have received at least three previous therapies [9]. Daratumumab induced tumour cell apoptosis through a variety of mechanisms, including complement‐dependent cytotoxicity, antibody‐dependent cell‐mediated cytotoxicity, antibody‐dependent cell phagocytosis and Fcγ receptor‐mediated apoptosis induced by the direct cytotoxicity [10], directly killing tumour cells by activating complement proteins, NK cells and macrophages, as well as by cross‐linking [11]. Daratumumab also abolished the highly immunosuppressive subsets of CD38^+^ Tregs, CD38^+^ MDSC and CD38 regulatory B cells (B‐reg) [12].
Many studies have shown that Daratumumab can effectively inhibit the growth of B cell tumours. CD38‐CAR‐T cells could significantly inhibit the growth of CD38‐overexpressing MCL cells in an in vitro model and transplanted tumour cells in mice [13]. Another preclinical experiment [14] showed that injection of Daratumumab into an in vitro model of DLBCL tumours resulted in significant tumour growth control. Therefore, Daratumumab may have a positive therapeutic impact on CD20^−^ R/R DLBCL. In addition, Daratumumab depleted the highly immunosuppressive subset of CD38^+^ Tregs, suggesting that Daratumumab may facilitate the proliferation of CAR‐T cells in vivo and play an auxiliary role in CAR‐T treatment.
However, the clinical data on Daratumumab therapy in patients with R/R DLBCL remain limited. Therefore, we evaluated the safety and efficacy of Daratumumab in four patients with R/R CD20^−^CD38^+^DLBCL, to explore the new treatment method for the disease.
Material and Methods
2
We collected data from patients treated with Daratumumab for R/R CD20^−^CD38^+^ DLBCL admitted to Wuhan Tongji Hospital between July 2021 and December 2023. They had been treated with at least three lines of chemotherapy (Details of pretime regimens are provided in Appendix C).
The efficacy and adverse reactions of the patients were observed (based on 2014 Lugano standard). Some patients received Daratumumab combined with CAR‐T therapy. The efficacy in these patients was also observed to evaluate the auxiliary effect of Daratumumab on CAR‐T therapy.
Four patients were enrolled in this study; baseline characteristics are shown in Table 1. Patients had been treated with multiple lines of chemotherapy, including rituximab‐based regimens, HSCT and multiple targets for CAR‐T treatment (CD19, CD22, CD79b, CD20). After relapse, the results of flow cytometry showed that the tumour cells were down‐regulated in the expression of targets such as CD20, and CD38 was strongly positive.
All patients underwent immunohistochemical analysis of tumour cells before the treatment; details are provided in Appendix A. Results showed that all patients had loss or mutation of CD20 and other targets before medication, which may not be effective for CD20‐containing monoclonal antibody. Although CD19 and CD22 are weakly positive in some patients, their expression rate is much lower than that of the CD38 antigen on the surface of the sample tumour. Therefore, CD38 monoclonal antibody is a good option.
Patients 1 and 2 were applied to Daratumumab combination chemotherapy and CAR‐T treatment; patients 3 and 4 were applied to Daratumumab combination chemotherapy only (without CAR‐T treatment). Details of treatment regimens are provided in Table 2.
All patients received Daratumumab 16 mg/kg by intravenous infusion weekly, with Dexamethasone 15 mg 1 h before administration, promethazine 25 mg and loxoprofen sodium tablets 30 mg 30 min before administration.
Follow‐up was conducted until January 2024. Due to the small sample size, we directly calculated 1‐year PFS (progression‐free survival, the time from the start of treatment to tumour progression or last follow‐up), 1‐year OS (overall survival, the time from the start of treatment to the patient's death or last follow‐up) and mOS (median overall survival) according to patients' data.
Results
3
Efficacy
3.1
Specific efficacy is shown in Figure 1. All four patients achieved varying degrees of remission (CR, n = 2; PR, n = 1; SD, n = 1), with an ORR (overall response rate) of 75% and a CBR (clinical benefit rate) of 100%. The 1‐year OS rate was 75%, the 1‐year PFS rate was 50% and mOS was 12 months.
All four patients achieved varying degrees of remission (CR, n = 2; PR, n = 1; SD, n = 1), with an ORR rate of 75% and a CBR rate of 100%.
In patients 1–2 (treated with Daratumumab combination chemotherapy and CAR‐T treatment), Daratumumab resulted in disease stabilisation and successful transition to CAR‐T, with tumour burden release after the full treatment (CR, n = 1; PR, n = 1).
In patient 3–4 (treated with Daratumumab combination chemotherapy only), Daratumumab achieved significant tumour control, 2 patients had clinical benefits (CR, n = 1; SD, n = 1).
TEAEs
3.2
About the TEAEs, no patients died during treatment. During the treatment in this study, patients experienced the following adverse effects: Anaemia (4/4), neutropenia (4/4), thrombocytopenia (4/4), fever (1/4), infusion‐related reactions (1/4) and upper respiratory tract infection (1/4). Details are provided in Appendix B.
Two patients were treated with Daratumumab‐containing regimens, and all successfully transitioned to CAR‐T with grade 1 CRS. Detailed data related to CRS in these patients were provided in Figure 2.
Patients 1 and 2 developed grade 1 CRS during the subsequent bridging CAR‐T therapy.
Additional Animal Experiment
3.3
In addition, for the case (Patient 2) involved in this paper, authors Huang Wei, Zhou Kuangguo et al. conducted additional animal experiments [14].
Researchers purchased DLBCL cells with p53 mutations and high expression of CD38 and injected them into 5‐week‐old female NOD‐SCID mice, successfully constructing allografted tumour models in mice. The mice were divided at random into five groups: vehicle group; Daratumumab group, venetoclax group, Daratumumab combined with venetoclax group; and Daratumumab and venetoclax combined with other chemotherapy group. Different regimens of chemotherapy were then applied to each group, and tumour size, tumour weight and mouse body weight were monitored carefully throughout the experiments.
Results came out afterwards. The mice in the Daratumumab combined with venetoclax group had a strong inhibitory effect on tumour growth. In contrast, Daratumumab and venetoclax alone did not significantly inhibit tumour growth.
Discussion
4
Efficacy
4.1
This is the first case series report of the efficacy of Daratumumab‐contained regimens in patients with R/R DLBCL. Based on many relevant experiments worldwide, Daratumumab has a certain anti‐tumour effect on R/R DLBCL. In this study, the core goal of salvage therapy after relapse is to use new targets or to help patients transition to the subsequent CAR‐T therapy. From this point of view, our findings showed that Daratumumab was successful in accomplishing this goal, helping patients relieve tumour burden and successfully leading to the CAR‐T treatment.
A number of previous clinical trials have verified the positive effect of this therapy. In the experiments done by Vidal‐Crespo A. et al. [15], researchers injected the DLBCL tumour model constructed in vitro with Daratumumab combined with R‐CHOP therapy. Later, the tumour in the experimental group had a relatively significant shrinkage compared with the control group injected only with R‐CHOP. Such experiments indicated that Daratumumab combined with other cytotoxic drugs has a more significant anti‐tumour effect than the traditional R‐CHOP regimen in R/R NHL.
In this study, all patients treated with Daratumumab showed clinical benefit at the subsequent evaluation, indicating that Daratumumab combination chemotherapy has a considerable application prospect in the treatment of R/R DLBCL. The different therapeutic efficacy of each patient may be related to the different basic conditions and the different combination chemotherapy regimens used.
There had been a phase II clinical trial of Daratumumab monotherapy in R/R NHL, using Daratumumab monotherapy to treat FL, MCL and DLBCL. The study met the predefined futility criteria. The possible reason is the difference between MM and NHL's tumour microenvironment. In addition, it may be attributed to the higher and more even CD38 expression rate on MM cells [2], resulting in the less significant effect of Daratumumab monotherapy in NHL than in MM. While using Daratumumab combination therapy, Daratumumab serves as a monoclonal antibody rather than serves as an ADC, which is the reason Daratumumab combination therapy had better efficacy than monotherapy.
Daratumumab also has a certain adjuvant effect on CAR‐T treatment. Daratumumab‐containing regimens can be used to bridge CAR‐T without compromising CAR‐T cell expansion or efficacy (Figure 2). In this case, all two patients successfully transitioned to CAR‐T therapy. Patient 1 and Patient 2 had a fairly positive response to subsequent CAR‐T therapy, and both patients smoothly tolerated CAR‐T therapy and had tumour remission. Relevant in vitro experiments have provided strong evidence for this. Jakub Krejcik et al. noted that CD38‐expressing immunosuppressive regulatory T and B cells and myeloid‐derived suppressor cells were sensitive to Daratumumab treatment; also, cytotoxic T‐cell number, activation and clonality increased after Daratumumab treatment in heavily pretreated relapsed and refractory MM. They described previously unknown immunomodulatory effects of Daratumumab through the reduction of CD38+ immunosuppressive cellular populations and concomitant induction of helper and cytotoxic T‐cell expansion, production of IFN‐γ in response to viral peptides and increased TCR clonality, indicating an improved adaptive immune response [12]. From this point of view, Daratumumab‐containing therapy may be complementary to CAR‐T therapy.
The small sample size is one of the shortcomings of this experiment. Additionally, due to the varying initial treatment plans for the patients, the selected combined chemotherapy drugs were not uniform, which is also a limitation of this study. In the future, we may verify our conclusions through prospective studies with larger sample sizes and more systematic and standardised approaches.
TEAEs
4.2
Safety is another advantage of the Daratumumab chemotherapy. The Daratumumab‐containing regimen showed a good safety profile in all patients; no patients died during the treatment.
Daratumumab has been shown to be safe in previous studies of MM, with few AEs associated with severe pancytopenia. In a phase 1/2 trial of Daratumumab, Lenalidomide and Dexamethasone in MM, no dose‐limiting toxicity was observed at the dose of 16 mg/Kg, and in subsequent treatments, Neutropenia was the most frequently reported (78.1%) grade 3/4 TEAE and was considered to be lenalidomide‐related [16]. It is noted that the patients have received multiple lines of chemotherapy previously; their basic state is extremely poor, and Daratumumab is used in combination with other chemotherapy drugs, which causes different AEs from Daratumumab monotherapy, all of which need to be comprehensively considered.
In a study of Daratumumab monotherapy in R/R NHL, the most common grade 3/4 AEs were anaemia, neutropenia and thrombocytopenia [1].
No specific AEs were observed in this study, and the AEs that occurred were easy to control, which led us to believe that the relevant treatment regimen was safe to a certain extent.
Conclusion
5
Above all, we can say that Daratumumab combination chemotherapy had a positive effect on four patients with R/R DLBCL and helped two patients to successfully bridge CAR‐T therapy. Overall, these cases demonstrated a good application prospect of Daratumumab in the treatment of CD20^−^CD38^+^ R/R DLBCL and helped bridge CAR‐T therapy.
Author Contributions
ZeTong Hong: conceptualization (lead), data curation (lead), formal analysis (equal), funding acquisition (equal), investigation (equal), methodology (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing – original draft (lead), writing – review and editing (lead). ZhaoYang Hong: conceptualization (lead), data curation (lead), formal analysis (equal), funding acquisition (equal), investigation (equal), methodology (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing – original draft (lead), writing – review and editing (lead). YaXian Ma: formal analysis (equal), funding acquisition (equal), investigation (equal), methodology (equal), project administration (equal), resources (equal), software (equal). Qing Yin: formal analysis (equal), investigation (equal), methodology (equal), project administration (equal). Min Liu: formal analysis (equal), resources (equal), software (equal), supervision (equal). Wei Huang: supervision (equal), validation (equal), visualization (equal). KuangGuo Zhou: investigation (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal). Dan Li: formal analysis (equal), resources (equal), software (equal), supervision (equal). TongJuan Li: conceptualization (equal), data curation (equal), formal analysis (equal), funding acquisition (equal), investigation (equal), methodology (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal). Miao Zheng: conceptualization (equal), data curation (equal), formal analysis (equal), funding acquisition (equal), investigation (equal), methodology (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethics Statement
The study was approved by the institutional review board of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent
Informed consent was obtained from all patients included in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. Salles , J. Duell , G. E. Barca , et al., “Tafasitamab Plus Lenalidomide in Relapsed or Refractory Diffuse Large B‐Cell Lymphoma (L‐MIND): A Multicentre, Prospective, Single‐Arm, Phase 2 Study,” Lancet Oncology 21, no. 7 (2020): 978–988.32511983 10.1016/S 1470-2045(20)30225-4 · doi ↗ · pubmed ↗
- 2G. Salles , A. K. Gopal , M. C. Minnema , et al., “Phase 2 Study of Daratumumab in Relapsed/Refractory Mantle‐Cell Lymphoma, Diffuse Large B‐Cell Lymphoma, and Follicular Lymphoma,” Clinical Lymphoma, Myeloma & Leukemia 19, no. 5 (2019): 275–284, 10.1016/j.clml.2018.12.013.30795996 · doi ↗ · pubmed ↗
- 3K. Amaador , J. M. I. Vos , S. T. Pals , et al., “Meta‐Analysis Between Waldenstrom Macroglobulinemia and Marginal Zone Lymphoma Using Logistic LASSO Regression,” Leukemia & Lymphoma 63, no. 5 (2022): 1070–1079, 10.1080/10428194.2021.2018584.34961399 · doi ↗ · pubmed ↗
- 4B. Vakrmanova , M. Novakova , P. Řiha , et al., “CD 38: A Target in Relapsed/Refractory Acute Lymphoblastic Leukemia‐Limitations in Treatment and Diagnostics,” Pediatric Blood & Cancer 69, no. 9 (2022): e 29779, 10.1002/pbc.29779.35592935 · doi ↗ · pubmed ↗
- 5M. Farber , Y. Chen , L. Arnold , et al., “Targeting CD 38 in Acute Myeloid Leukemia Interferes With Leukemia Trafficking and Induces Phagocytosis,” Scientific Reports 11, no. 1 (2021): 22062, 10.1038/s 41598-021-01300-8.34764342 PMC 8586007 · doi ↗ · pubmed ↗
- 6F. Wada , Y. Shimomura , T. Yabushita , et al., “CD 38 Expression Is an Important Prognostic Marker in Diffuse Large B‐Cell Lymphoma,” Hematological Oncology 39, no. 4 (2021): 483–489, 10.1002/hon.2904.34327725 · doi ↗ · pubmed ↗
- 7J. P. Laubach , Y. T. Tai , P. G. Richardson , and K. C. Anderson , “Daratumumab Granted Breakthrough Drug Status,” Expert Opinion on Investigational Drugs 23, no. 4 (2014): 445–452, 10.1517/13543784.2014.889681.24555809 · doi ↗ · pubmed ↗
- 8K. Mc Keage , “Daratumumab: First Global Approval,” Drugs 76, no. 2 (2016): 275–281, 10.1007/s 40265-015-0536-1.26729183 · doi ↗ · pubmed ↗