Usefulness of Telemonitoring in Respiratory Deterioration in a Patient Treated With Home High-Flow Nasal Therapy
Jean-Michel Arnal, Thomas Obert, Aude Garnero

TL;DR
Telemonitoring helped detect and manage a respiratory worsening in a patient using home high-flow nasal therapy.
Contribution
Demonstrates how telemonitoring can serve as an early warning system for respiratory issues in home high-flow nasal therapy patients.
Findings
Telemonitoring detected increased HFNC usage linked to respiratory symptoms before clinical evaluation.
Early intervention via telemonitoring led to rapid improvement after identifying an infection.
Patients can learn to adjust therapy based on telemonitoring feedback.
Abstract
A 63-year-old male with overlap syndrome had high-flow nasal cannula (HFNC) therapy added to his treatment in May 2023 after reporting reduced exercise tolerance due to dyspnea and recurrence of chronic bronchial congestion on existing therapy (noninvasive ventilation and appropriate drug treatment). HFNC therapy (Lumis HFT; ResMed) was started with prescribed usage of 2 h/day, a flow of 20 L/min, and a temperature of 37°C. Within 15 days, the patient noted improved clearance with thinner secretions, and then secretion volume decreased after 2 months. Six months after having HFNC connected to a telemonitoring platform (AirView), the homecare technician observed a sudden increase in HFNC usage (to > 4 h/day). After being contacted by the technician, the patient reported increased sputum production, low-grade fever, and exertional dyspnea. Evaluations found Haemophilus influenzae, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
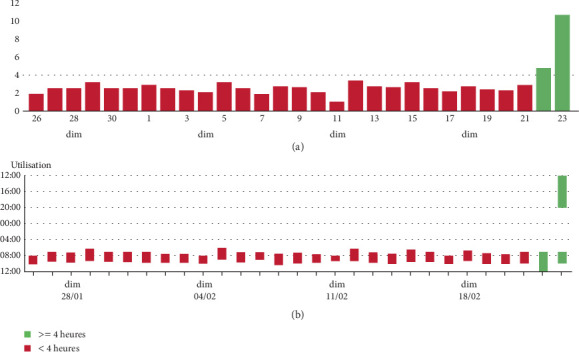 Figure 1
Figure 1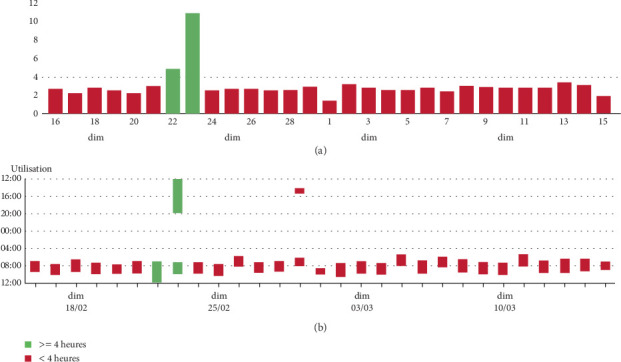 Figure 2
Figure 2- —ResMed
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Nosocomial Infections in ICU · Pediatric health and respiratory diseases
1. Introduction
High-flow nasal cannula (HFNC) therapy is recommended as a first-line treatment for acute hypoxemic respiratory failure in hospital settings and after extubation in intensive care units [1]. The use of HFNC at home has only taken place more recently. Daily humidification of inspired gases improves mucociliary clearance in patients with obstructive lung disease [2], with clinical benefits including reduced exacerbation frequency and lower hospitalization rates [3–6]. The Lumis HFT (ResMed) HFNC device is designed specifically for home use, providing lower flow rates than hospital devices; is easy to use for patients; and has remote monitoring capabilities. We present a case report where telemonitoring of home HFNC therapy allowed healthcare providers to detect a developing exacerbation early.
2. Case Presentation
The patient is a 63-year-old male with overlap syndrome, having both obesity-related obstructive sleep apnea (body mass index 31 kg/m^2^) and postsmoking chronic obstructive pulmonary disease (COPD; current nonsmoker, 50 pack-year smoking history). The patient's forced expiratory volume in 1 s (FEV_1_) was 26% of predicted. Chronic respiratory failure was diagnosed in 2020 during an acute exacerbation of COPD that required admission to the intensive care unit. At that time, home oxygen therapy (1.5 L/min) and noninvasive ventilation (NIV) were initiated (EPAP = 8 cm H_2_O; IPAP = 19 cm H_2_O; back‐up rate = 10 bpm), alongside treatment with a long-acting β2-agonist and a long-acting muscarinic antagonist. The patient was discharged home, where he lives alone, after completing a pulmonary rehabilitation program. He resumed daily walking for 90 min with ambulatory oxygen support. Nocturnal NIV usage was effective in maintaining normocapnia.
In May 2023, the patient reported reduced exercise tolerance due to dyspnea and recurrence of chronic bronchial congestion, with thick, hard-to-expectorate secretions. He was using NIV for 8 h and 15 min per night with normal arterial blood gases (PaO_2_ = 60 mm Hg; PaCO_2_ = 40 mm Hg). HFNC therapy (Lumis HFT; ResMed) was started with prescribed usage of 2 h/day, flow of 20 L/min, temperature of 37°C, and a size large nasal cannula [3]. Within 15 days, the patient noted improved clearance with initially more abundant and thinner secretions, and this was followed by a decrease in secretion volume after 2 months. The patient opted to continue HFNC therapy and self-adjusted the usage time to 1.5 h/day.
2.1. Intervention and Outcome
In August 2023, the HFNC device was connected to the AirView platform, enabling remote monitoring by the home care provider. In February 2024, the technician observed a sudden increase in HFNC usage to over 4 h/day on 2 consecutive days, with an unusually long afternoon session (Figure 1). Within the next 24 h, the technician contacted the patient, who reported increased sputum production, low-grade fever, and exertional dyspnea. The patient's physician was alerted and conducted a telephone-based Exascore [7] evaluation, suggestive of bronchitis without signs of clinical severity. Specifically, self-monitoring indicated that resting SpO_2_ remained above 92% while on his usual oxygen regimen [8]. Antibiotic therapy was initiated at home after testing showed the presence of Haemophilus influenzae. Given the acute increase in respiratory symptoms and the need for antibiotics, this episode meets criteria for a probable moderate COPD exacerbation according to GOLD, although pneumonia cannot be definitively excluded without chest imaging. Resting oxygen saturation remained at the patient's usual baseline, and no additional features suggested pneumonia, so imaging was not performed. The patient quickly improved and returned to his usual HFNC routine (Figure 2). After this episode, the patient learned to adjust his HFNC usage according to the degree of bronchial congestion.
3. Discussion
HFNC works by reducing anatomical dead space, reducing work of breathing and ventilatory burden. There is currently not a large volume of data on the use of HNFC in patients with overlap syndrome. One study suggested that it reduced nocturnal apneas and improved oxygenation [9], but no benefit in patients with overlap syndrome has been reported [10]. Our patient with overlap syndrome did benefit from HFNC therapy. However, the most interesting feature of this case was that HFNC telemonitoring data allowed the early detection of an acute moderate exacerbation of COPD, which led to timely intervention and possibly averted further clinical decline. Once a patient is familiar with the device, changes in HFNC usage duration could serve as an indicator of secretion burden, and sudden increases in usage may be an early sign of exacerbation.
Overall, telemonitoring adds value to home HFNC therapy by enabling early detection of clinical deterioration and guiding treatment adjustments based on real-life usage patterns. Empowering patients to self-modulate treatment contributes to individualized care and may prevent hospitalizations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rochwerg B. Einav S. Chaudhuri D. The Role for High Flow Nasal Cannula as a Respiratory Support Strategy in Adults: A Clinical Practice Guideline Intensive Care Medicine 202046122226223710.1007/s 00134-020-06312-y 33201321 PMC 7670292 · doi ↗ · pubmed ↗
- 2Hasani A. Chapman T. H. Mc Cool D. Smith R. E. Dilworth J. P. Agnew J. E. Domiciliary Humidification Improves Lung Mucociliary Clearance in Patients With Bronchiectasis Chronic Respiratory Disease 200852818610.1177/14799723070871902-s 2.0-5344909763918539721 · doi ↗ · pubmed ↗
- 3Rea H. Mc Auley S. Jayaram L. The Clinical Utility of Long-Term Humidification Therapy in Chronic Airway Disease Respiratory Medicine 2010104452553310.1016/j.rmed.2009.12.0162-s 2.0-7734912603420144858 · doi ↗ · pubmed ↗
- 4Storgaard L. H. Hockey H. U. Laursen B. S. Weinreich U. M. Long-Term Effects of Oxygen-Enriched High-Flow Nasal Cannula Treatment in COPD Patients With Chronic Hypoxemic Respiratory Failure International Journal of Chronic Obstructive Pulmonary Disease 2018131195120510.2147/COPD.S 1596662-s 2.0-8504597473629713153 PMC 5909797 · doi ↗ · pubmed ↗
- 5Nagata K. Horie T. Chohnabayashi N. Home High-Flow Nasal Cannula Oxygen Therapy for Stable Hypercapnic COPD: A Randomized Clinical Trial American Journal of Respiratory and Critical Care Medicine 2022206111326133510.1164/rccm.202201-0199 OC 35771533 PMC 9746854 · doi ↗ · pubmed ↗
- 6Simioli F. Fiorentino G. Cauteruccio R. Long-Term High Flow Nasal Cannula Therapy in Primary and Secondary Bronchiectasis Healthcare (Basel) 2023119 p. 125010.3390/healthcare 1109125037174791 PMC 10178516 · doi ↗ · pubmed ↗
- 7Soyez F. Ninot G. Herkert A. Validation d'un Questionnaire D'évaluation de L'exacerbation dans la BPCO: l'Exascore Revue des Maladies Respiratoires 2016331172410.1016/j.rmr.2015.09.0022-s 2.0-8495952197326518257 · doi ↗ · pubmed ↗
- 8Venkatesan P. GOLD COPD Report: 2024 Update The Lancet Respiratory Medicine 2024121151610.1016/S 2213-2600(23)00461-738061380 · doi ↗ · pubmed ↗