Distinct Imaging Features of Peripheral Nerve Sheath Tumours in NF2-Related Schwannomatosis: A Case Report
Küpper Hanna, Roggia Cristiana, Winter Natalie, Grimm Alexander, Nägele Thomas, Rosewich Hendrik, Schuhmann Martin Ulrich

TL;DR
A teenage patient with NF2-related schwannomatosis showed unusual nerve imaging features not typical of classic schwannomas.
Contribution
The case highlights distinct imaging features of perineurioma in NF2-related schwannomatosis, rarely reported before.
Findings
Ultrasound showed fusiform, multifascicular enlargement of the ulnar nerve and brachial plexus.
MRI revealed T2-hyperintense and T1-isointense nerve changes with diffuse gadolinium enhancement.
The findings suggest perineurioma as a rare but possible manifestation in NF2-related schwannomatosis.
Abstract
Peripheral nerve sheath tumours (PNST) are an important feature of the NF2-related schwannomatosis. These constitute primarily schwannomas which are characterized as nodular, solitary benign tumours of single fascicles. We here describe a pronounced, extensive, multifascicular enlargement of the right ulnar nerve and bilateral brachial plexus in a teenage patient with NF2-related schwannomatosis. Neither their imaging nor the clinical characterization were consistent with classic schwannomas. Within a multimodal work-up, detailed and standardized high-resolution nerve ultrasound was correlated to clinical, electroneurographic, and MRI findings. Follow-up data over 2 years were provided. The clinical presentation of a slowly progressive, predominantly motor axonal neuropathy of the right ulnar nerve prompted a comprehensive nerve ultrasound examination, initiated by this clinically and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
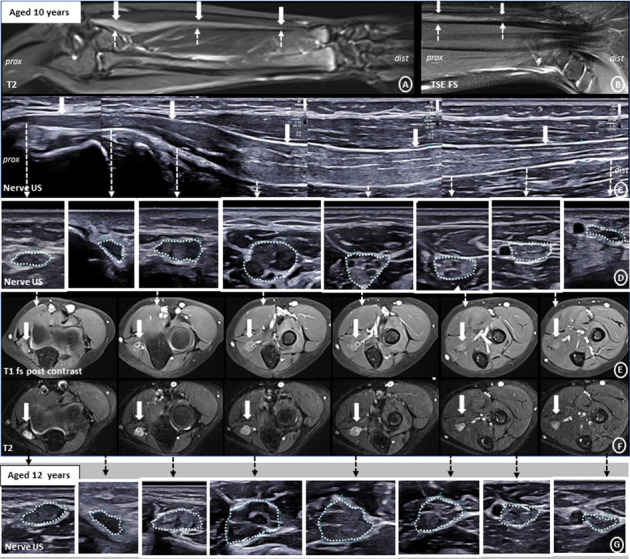 Figure 1
Figure 1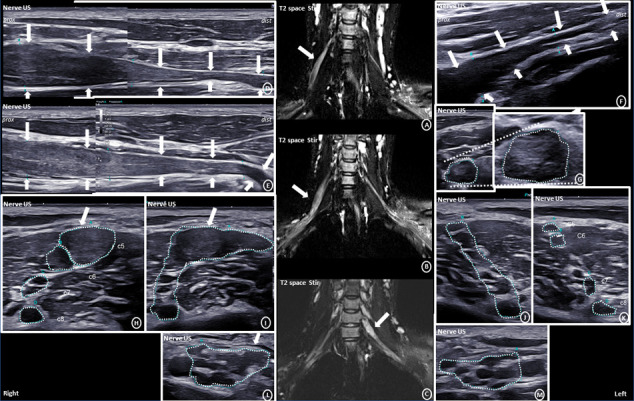 Figure 2
Figure 2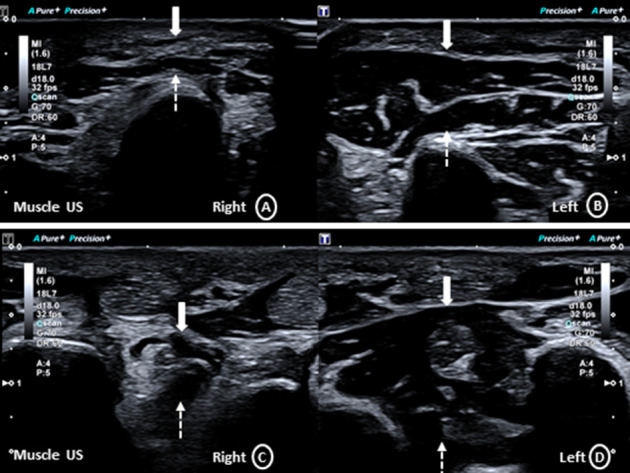 Figure 3
Figure 3- —Universitätsklinikum Tübingen
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Spinal Hematomas and Complications · Sarcoma Diagnosis and Treatment
1. Introduction
The NF2-related schwannomatosis is a rare autosomal dominant tumour predisposition disorder, linked to the neurofibromatosis type 2 (NF2) tumour suppressor gene on chromosome 22q [1, 2]. It has a broad phenotypic spectrum, affecting the nervous system, eyes and skin [3, 4]. Hearing loss is the typical presentation in adulthood, due to bilateral vestibular schwannoma. When presenting in childhood, signs of a mononeuropathy, skin tumours or ophthalmologic pathologies are frequent [3]. Tumour entities of the cranial nerves include the characteristic bilateral vestibular schwannomas. Meningioma, glioma, astrocytoma and spinal ependymoma are other manifestations in the central nervous system [4].
Peripheral nerve sheath tumours (PNST), primarily schwannomas, are a further important hallmark of this syndrome [5]. Schwannomas are benign PNST which present as subcutaneous nodules, originating from cutaneous sensory nerves, as well as from major peripheral nerves [6]. The distinctive presentation is a slowly growing mass, with possible symptoms of nerve compression, typically sensory (paraesthesia, numbness, and radiating pain). Motor neuropathic symptoms are occasionally described [7]. Morphologically, schwannomas are solitary spindle cell tumours, with a cut surface of a fibrous capsule [8]. Only few nerve ultrasound studies of NF2-related schwannomatosis have been published to date [9, 10], examining solely adults. They describe classic schwannomas as oval-shaped, homogeneous hypo- to isoechoic nodules of single fascicles, displacing normal fascicles, with well-defined margins. On MRI [11], they are characterized as T2-hyperintense, nodular “macro- and microlesions” of peripheral nerves.
However, the here presented clinical as well as imaging characteristics of a teenage girl carrying a pathogenic variant in the NF2-gene with an extensive, multifascicular enlargement of the right ulnar nerve and parts of the brachial plexus do not correspond to classic schwannomas. For differential diagnosis, a detailed analysis of the here presented imaging data is correlated to reports of NF2-related schwannomatosis in the literature.
2. Methods
Ultrasound of peripheral nerves and muscles was conducted with a high-resolution (18 MHz) broad band linear probe (Canon Aplio a, Canon Medical Systems GmbH, Germany) with standardized ultrasound settings on yearly follow-up examinations over a period of 2 years. Cross-sectional area (CSA) and diameter of peripheral nerves and cervical roots were determined and correlated to detailed clinical examinations as well as focussed nerve conduction studies. Contrast-enhanced MRI of the lower right arm and bilateral brachial plexus was performed once, of the brain and spinal cord twice. Patient consent was obtained.
3. Results
At the age of 10 years, she presented with a motor predominant deficit of the right ulnar nerve which, retrospectively, had slowly developed over 3 years. There was pronounced weakness (Medical Research Council (MRC) Scale for Muscle Strength 3/5) for the abduction of the right little and index finger, with significant atrophy of the abductor digiti minimi and interosseus dorsalis muscles. The sensation for touch was mildly reduced in the area of the right dorsal ulnar branch. On nerve conduction study, signs of a predominantly motor axonal neuropathy were depicted for the right ulnar nerve, with normal findings for the left ulnar and right median nerve. Follow-up over 2 years was stable (Supporting table 1).
On nerve ultrasound, there was pronounced long-extended enlargement of the right ulnar nerve, throughout its course from the elbow to the wrist, with a maximum CSA of 38 mm^2^ in the proximal forearm (Figure 1(D)). The enlargement was fusiform, multifascicular, mixed hypo- and hyperechogenic, without signs of calcifications. The fascicular pattern was preserved. However, at the site of maximum enlargement, fascicular differentiation was reduced. The outer margins of the ulnar nerve were well defined. Morphological appearance of the nerve proximal and distal from the enlargement was normal, and there was gradual tapering of the enlargement. On Doppler sonography, there was no increased vascularization. A similar, but more multinodular pattern of enlargement, was depicted in the right cervical nerve roots C5 and C6 as well as left C7 (Figure 2). On ultrasound follow-up after one and 2 years, the fascicular differentiation within the maximally enlarged nerve segments appeared further reduced, while the absolute extent of nerve enlargement seemed comparable (Figure 1(G)).
Muscle ultrasound depicted a hyperechogenic atrophy of the right abductor digiti minimi and dorsal interosseus muscles (Figure 3). Nerve ultrasound screening of other peripheral nerves was normal apart from some hypoechogenic, accentuated fascicles (Supporting table 2).
On MRI, the right ulnar nerve appeared T1-isointense, markedly T2-hyperintense and showed diffuse, moderate to marked contrast enhancement (T1) (Figures 1(A), 1(B), 1(E)). Laboratory work-up for inflammatory neuropathies revealed no significant abnormalities. After 2 cycles of intravenous immunoglobulin (2 g/kg), there was no significant clinical or imaging improvement. Subsequent genetic analysis, initiated originally for the differential of a rare hereditary neuropathy, revealed a disease defining pathogenic splice variant (c.1123-2A > G, p.?) in the NF2 gene. Detection of small nodular schwannomas in the vestibular (3 × 2 mm) and mandibular nerve (4 × 3 mm) (Supporting Figure 1) on subsequent brain MRI confirmed the diagnosis of an NF2-related schwannomatosis [5]. Follow-up brain MRI after 1.5 years showed no significant change. Functional testing of the vestibulocochlear nerve, ophthalmological evaluation and spinal MRI were normal. MRI of the brachial plexus demonstrated a small additional enlargement of the left cervical root C4. The enlargements were T2-hyperintense, slightly inhomogeneous, with mild diffuse contrast enhancement.
4. Discussion
This is a case report of a rare combination of different nerve sheath tumours in a teenage patient with genetically confirmed NF2-related schwannomatosis. Specific findings of the ulnar nerve were highly suggestive of a perineurioma [12–16], i.e., the history of a teenage-onset, slowly evolving, painless, predominantly motor axonal mononeuropathy, with weakness and muscle atrophy, and, on imaging, a long-extended, fusiform, multifascicular nerve enlargement, with proximal and distal tapering, in combination with a T2-hyper- and T1-isointensity as well as a marked gadolinium enhancement on MRI. The here described nerve ultrasound and MRI features correspond closely to previous imaging descriptions in 6 histologically confirmed perineurioma cases with a similar history [17, 18], thus making other differential diagnoses very unlikely. Rarely, perineurioma has been described histologically in NF2-related schwannomatosis [12], as well as mutations in the NF2 gene in histogenetic analyses of perineurioma [2]. The intraneural perineurioma is a benign PNST, with common locations in major peripheral nerves and brachial plexus. First described by Imaginarion in 1964 [19], the anecdotal connotation as a localized hypertrophic (mono)neuropathy (“dense swollen cord” [17]) or “interstitial hypertrophic neuritis” [19] as well as the Perineurioma Diagnostic Criteria [20] meet the here described characteristics [21]. To date, an epineurectomy and fascicular biopsy for further diagnostic and therapeutic purposes have not been conducted in this teenage patient, due to her long-standing stable clinical and electroneurographic course, but previewed in case of any change within the close monitoring.
The findings of the here described vestibular and mandibular nerves are, in contrast, characteristic of classic schwannomas [9–11], due to their nodular, homogenous enlargement and, to date, asymptomatic status. By comparison, the multinodular to diffusely thickened appearance [22] of the bilateral brachial plexus on ultrasound (supporting video 6-7) as well as the slightly inhomogeneous pattern with only mild diffuse contrast enhancement on MRI, without any clinical correlate, could be consistent with plexiform schwannomas. First characterized by Masson in 1970 [23], these have been described as benign variants in NF2-related schwannomatosis [1, 24]. However, their localization in the plexus is characterized as rare [25] and the morphological pattern often as irregular inhomogeneous masses [22], occasionally including degenerative changes (haemorrhage, cyst formation and dystrophic calcifications) which is not present here. Hybrid nerve sheath tumour (HNST) [26] in NF2-related schwannomatosis has, on the other hand, to date only been described for the combination of schwannoma and neurofibroma [27], not perineurioma and plexiform schwannoma. No characteristic features, though, of classic neurofibroma (small, hypoechogenic, and nodular; supporting Figure 2) [16] or plexiform neurofibroma (increased, hyperechogenic stroma between clearly discernible fascicles, and “bag of worms” appearance) were delineated in this teenage patient. A fascicular biopsy for further diagnostic purposes has not been performed to date due to her long-standing stable clinical and imaging course, but previewed in case of any change within the close monitoring. Malignant transformation of PNST in NF2-related schwannomatosis is exceedingly rare [28], especially without preceding radiation. Correspondingly, there was no conspicuous central necrosis, haemorrhage, peritumoral oedema, calcification, rich vascularization, and intratumoral lobulation [16] in the here presented case.
The pathogenic splice variant c.1123-2A > G, p.? affects the exons 11–15 of the NF2 gene which, within the known genotype-phenotype correlation, has been associated with a milder disease course [29]. However, the young manifestation age in this girl argues against this. The importance of thorough phenotyping including detailed HRUS nerve imaging in NF2-related schwannomatosis, within the differential work-up of hypertrophic (mono)neuropathy [20], is corroborated by the here presented case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Masson P. Human Tumors 19702 nd Histology Diagnosis and Technique
- 2Da Gama Imaginário J. Coelho B. ToméF. Luis M. L. S. Névrite Interstitielle Hypertrophique Monosymptomatique Journal of the Neurological Sciences 1964134034714192576 · pubmed ↗
- 3Ruggieri M. PraticòA. D. Serra A. Childhood Neurofibromatosis Type 2 (NF 2) and Related Disorders: From Bench to Bedside and Biologically Targeted Therapies Acta Otorhinolaryngologica Italica 2016 October 36534536710.14639/0392-100X-10932-s 2.0-8500370766627958595 PMC 5225790 · doi ↗ · pubmed ↗
- 4Pellerino A. Verdijk R. M. Nichelli L. Andratschke N. H. Idbaih A. Goldbrunner R. Diagnosis and Treatment of Peripheral and Cranial Nerve Tumors With Expert Recommendations: An European Network for Rare Cancers (EURACAN) Initiative Cancers (Basel) 2023 March 157p. 193010.3390/cancers 15071930 PMC 1009350937046591 · doi ↗ · pubmed ↗
- 5Asthagiri A. R. Parry D. M. Butman J. A. Neurofibromatosis Type 2 The Lancet 2009 June 37396791974198610.1016/S 0140-6736(09)60259-22-s 2.0-66149185290 PMC 474885119476995 · doi ↗ · pubmed ↗
- 6Farschtschi S. Gelderblom M. Buschbaum S. Bostock H. Grafe P. Mautner V. F. Muscle Action Potential Scans and Ultrasound Imaging in Neurofibromatosis Type 2 Muscle & Nerve 2017 March 55335035810.1002/mus.252562-s 2.0-8500686889227422240 · doi ↗ · pubmed ↗
- 7Belakhoua S. M. Rodriguez F. J. Diagnostic Pathology of Tumors of Peripheral Nerve Neurosurgery 2021 February 88344345610.1093/neuros/nyab 02133588442 PMC 7884141 · doi ↗ · pubmed ↗
- 8Winter N. Rattay T. W. Axer H. Ultrasound Assessment of Peripheral Nerve Pathology in Neurofibromatosis Type 1 and 2 Clinical Neurophysiology 2017 May 128570270610.1016/j.clinph.2017.02.0052-s 2.0-8501538616328315612 · doi ↗ · pubmed ↗