Preeruptive Intracoronal Dentin Resorption: Radiographic Diagnosis and Clinical Approach
Adrian Gomez-Fernandez, Maria Fernanda Alfaro-Solis

TL;DR
A rare dental condition called preeruptive intracoronal resorption was diagnosed in a teenager using advanced imaging, highlighting the need for early detection and specialized treatment.
Contribution
This case study provides insights into the clinical management and diagnostic challenges of preeruptive intracoronal resorption.
Findings
Preeruptive intracoronal resorption was detected via CBCT in an unerupted tooth.
Early intervention failed to prevent pulp necrosis, necessitating tooth extraction.
Histopathological analysis suggested a benign follicular or odontogenic lesion.
Abstract
Preeruptive intracoronal resorption (PEIR) is a rare, asymptomatic condition typically detected incidentally on radiographic examination. Its etiology remains unclear, and clinical management is often controversial due to the lack of standardized treatment protocols. A 14-year-old female was referred after routine orthodontic imaging revealed multiple radiolucent lesions in unerupted teeth. Cone beam computed tomography (CBCT) confirmed a hypodense intracoronal lesion in Tooth 37. Initial management included interdisciplinary assessment, pulp vitality testing, and protective restoration with glass ionomer cement following electrosurgical removal of the distal operculum. Despite early intervention, the tooth developed pulp necrosis, requiring extraction. Histopathological analysis of pericoronal tissue revealed loose connective tissue consistent with follicular origin or a benign…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
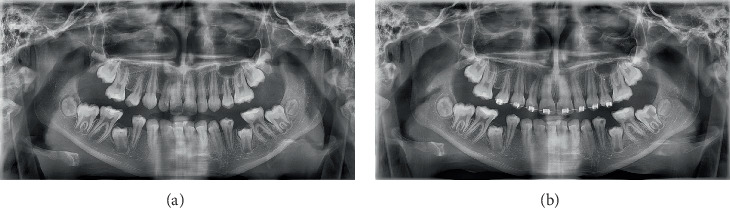 Figure 1
Figure 1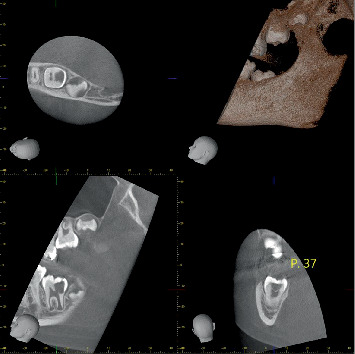 Figure 2
Figure 2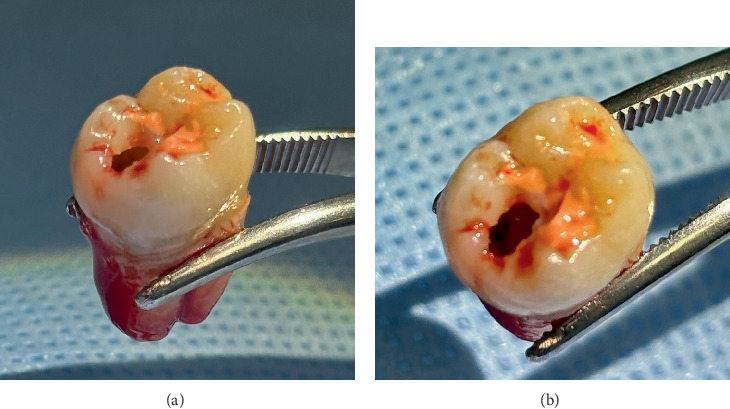 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Radiography and Imaging · Bone and Dental Protein Studies · Endodontics and Root Canal Treatments
1. Introduction
Preeruptive intracoronal resorption (PEIR) is an uncommon pathological condition that affects the dentin of unerupted teeth. It is characterized by well-defined radiolucent cavities within the crown, typically located at the dentinoenamel junction, and is detected exclusively through radiographic examinations, as it does not present clinical symptoms prior to eruption [1, 2]. Initially referred to as “occult caries,” the term PEIR is now preferred, as it more accurately reflects its noncarious origin [3, 4].
The first documented case of PEIR was reported in 1941 [4]. Since then, several etiological theories have been proposed, including apical inflammation of primary teeth, dentin developmental defects, dental caries, and ectopic eruption [5, 6]. The most widely accepted hypothesis suggests that resorption results from the invasion of resorptive cells into forming dentin, facilitated by disruptions in crown development [2, 5]. Histologically, these lesions contain soft tissue, inflammatory cells, and osteoclasts, supporting the theory of an active resorptive process distinct from conventional caries [3, 7].
The prevalence of PEIR ranges from 0.2% to 27.3%, depending on the population studied and the diagnostic methods used [8, 9]. Molars and premolars are the most frequently affected teeth, with mandibular second molars and maxillary premolars reported most often [9]. Recent studies have also identified mandibular and maxillary first molars as potential sites, with a prevalence as high as 31% in impacted teeth [5, 10]. Although PEIR has been mainly reported in permanent dentition, isolated cases in primary dentition have also been described, potentially underdiagnosed due to the infrequent use of radiographs in unerupted primary teeth [4].
Since PEIR is asymptomatic before eruption, diagnosis relies entirely on systematic radiographic evaluations. Cone beam computed tomography (CBCT) has proven useful in assessing lesion extent and proximity to the pulp chamber, aiding in treatment planning [10, 11]. The lesion may remain stable or progress rapidly, causing significant structural damage, underscoring the importance of early detection [12].
Despite increasing clinical recognition, there is no consensus on the ideal treatment approach. Some authors recommend monitoring small lesions, while others suggest surgical exposure and restoration or extraction in advanced cases [13, 14]. Biocompatible restorative materials such as glass ionomer cement and Biodentine have been proposed for pulp preservation [3]. This article presents a clinical case of PEIR in a pediatric patient, emphasizing the importance of early diagnosis, interdisciplinary management, and the role of advanced imaging tools.
2. Case Report
2.1. Medical History
A 14-year-old Costa Rican female, single and a high school student, was referred to the postgraduate program in pediatric dentistry for dental evaluation after an orthodontic assessment revealed radiolucent areas in several unerupted teeth. She had no relevant medical or family history and was not taking any medications. At the time of the consultation, she was asymptomatic and wore fixed orthodontic appliances in the upper arch, which were recommended for removal to facilitate a more accurate diagnosis.
2.2. Clinical and Radiographic Findings
Panoramic radiographs taken in January and May 2023 revealed progressive radiolucency in the mandibular left second molar (Tooth 37) (Figure 1a,b), as well as stable radiolucent areas in Teeth 47, 45, and 34. A periapical radiograph initially raised suspicion of dental caries, although the tooth had not yet erupted.
To confirm the diagnosis and assess the extent of the lesion, a CBCT scan was performed (Figure 2). It showed a hypodense area extending into the pulp chamber, without signs of periapical inflammation. Additionally, a discontinuity in the enamel at the distal fossa was observed.
An interdisciplinary evaluation by the endodontics, orthodontics, and pediatric dentistry departments included pulp vitality testing of Tooth 37, which yielded normal responses at that time. However, the patient reported discomfort in Teeth 26 and 36, prompting occlusal adjustment and the application of fluoride varnish (Clinpro, 3M ESPE). A few days later, she presented with persistent pain in the lower left quadrant.
2.3. Treatment
Due to persistent pain, a new endodontic evaluation was conducted in November 2023. Cold testing with EndoIce on Tooth 37 elicited a positive response, indicating potential pulp involvement. A referral to the periodontics department was made for removal of the distal operculum using electrosurgery, which allowed direct visualization of the lesion. A provisional protective restorative material (Fuji TRIAGE, GC Corporation) was then applied. Two days later, during the initiation of endodontic treatment, pulp necrosis was confirmed, and extraction was deemed necessary. The procedure was performed by the oral surgery department. A specimen that included pericoronal soft tissue and, based on clinical inspection, part of the intracoronal lesion contents was collected for histopathological analysis. The extracted mandibular left second molar revealed cavitation consistent with intracoronal resorption (Figure 3). Following extraction, the mandibular left second molar (Tooth 37) was examined macroscopically.
Histopathological analysis revealed loose connective tissue, consistent with either a dental follicle or a benign lesion such as a myxoma.
2.4. Follow-Up
At the 6-, 10-, and 12-month follow-up appointments, the patient remained asymptomatic. Periapical radiographs showed no new lesions or progression of existing ones. The patient continues to be monitored through interdisciplinary follow-up to assess her long-term clinical progress (Figure 4).
3. Discussion
This clinical case highlights the importance of early diagnosis and an interdisciplinary approach in managing PEIR, a rare condition whose timely detection can prevent serious complications. The well-defined radiolucency observed at the dentinoenamel junction was consistent with previously reported cases [9]. CBCT allowed precise assessment of the lesion's extent and its proximity to adjacent structures [10, 11].
Although the reported prevalence of PEIR ranges from 0.2% to 27.3%, its asymptomatic nature and low frequency complicate its identification [6, 12]. Therefore, systematic radiographic assessment of unerupted teeth is strongly recommended [15].
In this case, initial management was conservative, in accordance with current literature recommendations [4, 6]. Interventions such as the removal of the distal operculum and the application of Fuji TRIAGE aimed to preserve the tooth's function. However, the lesion progressed to pulp necrosis, necessitating extraction. This outcome underscores that despite timely intervention, tooth preservation may not always be feasible in advanced cases [9, 10].
The timing of diagnosis plays a pivotal role in determining the most appropriate treatment approach for PEIR. In children between 9 and 11 years of age, extraction combined with strategic orthodontic planning for distal molar substitution may be a favorable option—even when the affected tooth appears salvageable—particularly when long-term prognosis is uncertain. Current clinical guidelines and recent literature emphasize that early detection broadens the therapeutic window, allowing for a more individualized approach ranging from restorative management to extraction with orthodontic space closure, adapted to the patient's stage of dental development and occlusal considerations [16–18].
Histopathological analysis of the lesion in the present case revealed loose connective tissue with mild vascularity and edema, without evidence of inflammation, neoplastic changes, or calcified structures. No odontogenic epithelial rests or enamel organ remnants were identified, but the features were compatible with either a myxoma or dental follicular tissue. Although the clinical impression was that the excisional biopsy included both the pericoronal soft tissue and part of the intracoronal contents, the histopathological report describes the sample as connective tissue compatible with dental follicle or myxoid tissue, without explicitly distinguishing between the pericoronal and intracoronal components. Further studies with targeted sampling could help clarify the histological differences between these regions in PEIR lesions.
Previous studies have reported that these resorptive areas may contain fibrous tissue, dental follicle remnants, myxoid areas, or even granulomatous components [12–14]. Additional recent reports have documented intracoronal cavities consisting of fibrovascular connective tissue with inflammatory infiltrate and odontogenic epithelial remnants, as well as fibrous stroma with occasional inflammatory cells and signs of active resorptive activity, further supporting a cell-mediated resorptive process [19, 20]. However, the exact origin and pathological mechanism of tissue resorption remain poorly understood. Further research into the cellular composition of these lesions may help elucidate their etiology and support more precise clinical management.
Ultimately, this case reinforces the value of CBCT in the accurate diagnosis and treatment planning of PEIR, as well as the necessity of interdisciplinary collaboration. Long-term clinical and radiographic follow-up is essential not only to monitor for recurrence but also to prevent the development of new lesions, ensuring improved outcomes for affected patients.
4. Conclusion
This clinical case underscores the importance of systematic radiographic evaluation and the use of advanced diagnostic tools such as CBCT in the detection and management of PEIR. The interdisciplinary approach enabled accurate assessment of the lesion and supported informed clinical decision-making.
While conservative treatment is preferable in early stages, this case demonstrates that extraction may be unavoidable in advanced lesions with pulp involvement to prevent further complications. Moreover, the histopathological analysis reinforces the need for tissue evaluation in complex cases to confirm the diagnosis.
This report contributes to the clinical understanding of PEIR by highlighting the need to establish clearer management protocols and encouraging further research into its etiology, prevalence, and clinical progression. It also emphasizes the importance of long-term follow-up to improve both clinical and functional outcomes in affected patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yüksel H. T. Türkmenoğlu A. Çelikkol B. EvirgenŞ. Gulsahi K. Gulsahi A. Pre-Eruptive Intracoronal Resorption of Permanent Dentition: A New Classification and a Multidisciplinary Study Australian Endodontic Journal 202349 Supplement 116216910.1111/aej.1270636317538 · doi ↗ · pubmed ↗
- 2Counihan K. P. O'Connell A. C. Case Report: Pre-Eruptive Intra-Coronal Radiolucencies Revisited European Archives of Paediatric Dentistry 201213422122610.1007/BF 032628742-s 2.0-8486766601322883363 · doi ↗ · pubmed ↗
- 3Spierer W. A. Fuks A. B. Pre-Eruptive Intra-Coronal Resorption: Controversies and Treatment Options Journal of Clinical Pediatric Dentistry 201438432632810.17796/jcpd.38.4.dm 7652634 h 12705 v 25571683 · doi ↗ · pubmed ↗
- 4Omar S. Choi J. Nelson B. Shin M. Chen J. W. Pre-Eruptive Intracoronal Resorption (PEIR): Literature Review and Case Report Journal of the California Dental Association 201543525526010.1080/19424396.2015.1222284526798901 · doi ↗ · pubmed ↗
- 5Alon E. Amato R. B. Ptak D. M. Pre-Eruptive Intracoronal Resorption (PEIR): A Case Report Journal of Endodontics 202349222422810.1016/j.joen.2022.11.00936403786 · doi ↗ · pubmed ↗
- 6Gurdán Z. Balázs D. Pásti D. Pre-Eruptive Intracoronal Resorption in Orthodontic Patients: A Retrospective Analysis of 3,143 Patients Heliyon 202398 e 1869910.1016/j.heliyon.2023.e 1869937560674 PMC 10407135 · doi ↗ · pubmed ↗
- 7Al-Batayneh O. B. Al Tawashi E. K. Pre-Eruptive Intra-Coronal Resorption of Dentine: A Review of Aetiology, Diagnosis, and Management European Archives of Paediatric Dentistry 202021111110.1007/s 40368-019-00470-42-s 2.0-8507071892131414395 · doi ↗ · pubmed ↗
- 8Wong L. Khan S. Occult Caries or Pre-Eruptive Intracoronal Resorption? A Chance Finding on a Radiograph Pediatric Dentistry 201436542943225303513 · pubmed ↗