Retrospective study of elderly patients with advanced ovarian cancer who did not undergo surgery
Hui Qu, QianXue Wei, Wen Gu, Zhenhua Du, Xiuqin Li, Yu Xia

TL;DR
This study examines the treatment outcomes of elderly patients with advanced ovarian cancer who skipped surgery and received chemotherapy and maintenance therapy.
Contribution
It explores the viability of non-surgical treatment for elderly or ineligible patients with advanced ovarian cancer.
Findings
The overall response rate was 80.0%, with 12 out of 15 patients achieving partial response.
The median progression-free survival was 19.0 months, and the 3-year overall survival rate was 65.2%.
Combining chemotherapy with PARP inhibitor maintenance therapy showed promising results in disease control.
Abstract
To evaluate the clinical outcomes of elderly patients with advanced ovarian cancer who did not undergo surgery and received chemotherapy with or without maintenance therapy. We retrospectively analyzed the clinical data of 15 patients with advanced high-grade serous ovarian cancer who were treated at our hospital between 2018 and 2023. These patients either had multiple comorbidities or refused surgery. Data collected included patient demographics, treatment regimens, chemotherapy cycles, clinical response, progression-free survival (PFS), and overall survival (OS). The median age of the patients was 73 years (range, 50-86 years). Fourteen patients received platinum-based chemotherapy combined with paclitaxel or liposomal doxorubicin, with or without bevacizumab, for 3 to 6 cycles. Twelve patients who achieved disease control received PARP inhibitor maintenance therapy. The overall…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
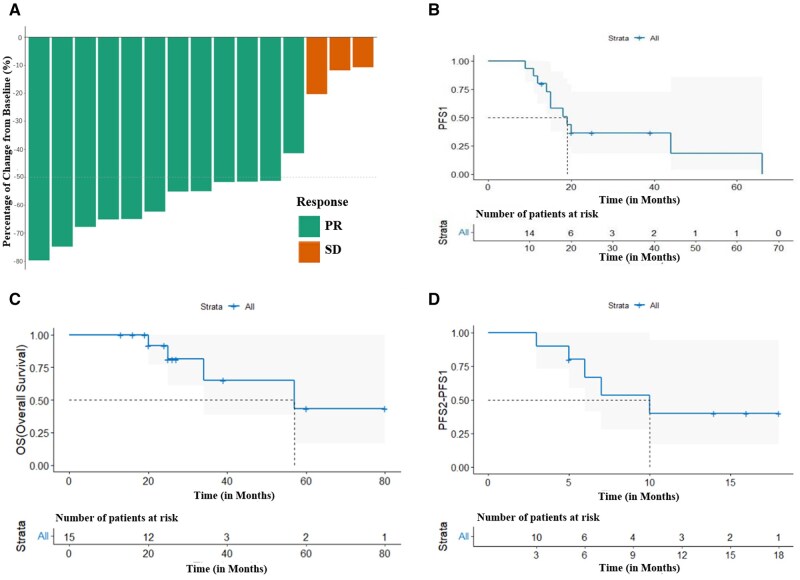 Figure 1
Figure 1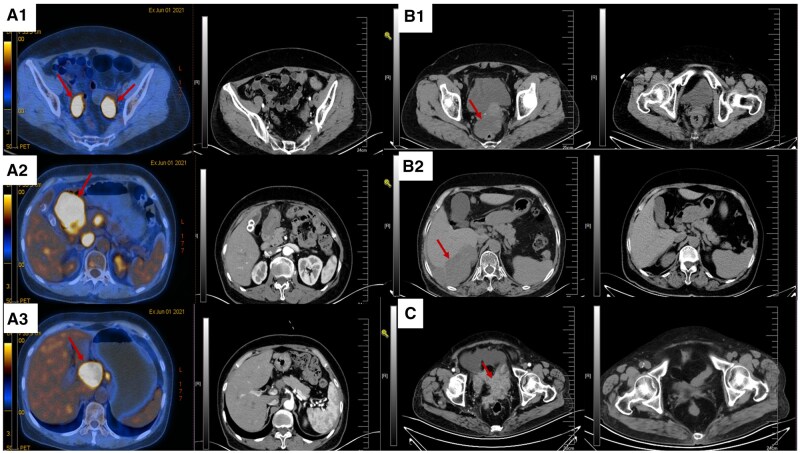 Figure 2
Figure 2|
| |
|---|---|
|
| |
|
| 7 (46.7) |
|
| 8 (53.3) |
|
| |
|
| 0 |
|
| 8 (53.3) |
|
| 7 (46.7) |
|
| |
|
| 15 (100%) |
|
| 0 |
|
| |
|
| 0 |
|
| 15 (100%) |
|
| |
|
| 12 (80.0%) |
|
| 3 (20.0%) |
| Patient number | Age (years) | Stage | Comorbidities and reasons for not undergoing surgery | Therapy regimen | Reasons for not completing chemotherapy | Efficacy evaluation | Maintenance therapy | PFS1 (months) | PFS2 (months) | OS (months) |
|---|---|---|---|---|---|---|---|---|---|---|
| P1 | 76 | III | Pulmonary embolism; Lower limb thrombosis; patient refused surgery | TC* | Not applicable | PR | Niraparib | 12 | 5 | 34 |
| P2 | 51 | IVB | Severe coronary stenosis; hypertension stage II; patient refused surgery | Docetaxel + Cisplatin*6 | Not applicable | PR | Fluzoparib | 15 | 7 | 26+ |
| P3 | 50 | IVB | Hypertension stage II; patient refused surgery due to financial reasons | TC*6 (Refusal of sequential chemotherapy) | Not applicable | PR | None | 9 | 18+ | 27+ |
| P4 | 75 | IVB | Facial nerve paralysis; hypertension stage II; patient refused surgery | TC + Bevacizumab (intraperitoneal infusion)*3 | Severe neutropenia with septic shock; patient refused further chemotherapy | SD | Fluzoparib | 15 | 6 | 25 |
| P5 | 86 | III | Rheumatoid arthritis; patient refused surgery due to advanced age | TC*3 | Herpes zoster with severe postherpetic neuralgia | SD | Fluzoparib | 25+ | Not applicable | 25+ |
| P6 | 56 | IVB | Metastasis in the upper abdomen involving the pancreas head and duodenum; patient refused surgery | TC + Bevacizumab* | Not applicable | PR | Pamiparib | 20 | Not applicable | 20 |
| P7 | 73 | III | History of thyroid cancer; hypertension stage II; patient refused surgery | TC* | Not applicable | PR | Fluzoparib | 19 | 5+ | 24+ |
| P8 | 69 | III | Hypertension stage II; patient refused surgery | TC* | Not applicable | PR | Fluzoparib | 20+ | Not applicable | 20+ |
| P9 | 65 | IVB | Patient refused surgery | TC + Bevacizumab*4 | Not applicable | PR | Fluzoparib | 14 | 5+ | 19+ |
| P10 | 76 | III | Patient refused surgery due to advanced age | TC* | Patient stopped treatment voluntarily | PR | None | 18 | 10 | 57 |
| P11 | 76 | IVB | Patient refused surgery due to advanced age | TC*6 | Not applicable | PR | Niraparib | 44 | 16+ | 60+ |
| P12 | 61 | IVB | Right tibial fracture after 3 cycles of neoadjuvant chemotherapy; patient refused surgery | Liposomal Doxorubicin + Carboplatin*6 | Not applicable | PR | None | 66 | 14+ | 80+ |
| P13 | 73 | III | Splenic metastasis; hypertension stage II; patient’s family refused surgery | TC*3 | Patient unable to tolerate chemotherapy side effects | SD | Fluzoparib | 13+ | Not applicable | 13+ |
| P14 | 81 | III | Hypertension stage II; history of liver cancer; hepatitis B and liver cirrhosis; patient refused surgery and chemotherapy | Bevacizumab immunotherapy | Not applicable | SD | Fluzoparib + immunotherapy | 11 | 3 | 16+ |
| P15 | 71 | IVB | Patient refused surgery and chemotherapy due to advanced age | TC*6 | Not applicable | PR | Niraparib | 39+ | Not applicable | 39+ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · PARP inhibition in cancer therapy · Intraperitoneal and Appendiceal Malignancies
Introduction
Ovarian cancer primarily affects elderly women, with most cases occurring in those aged 65 and older.1 Research has shown that advanced age is a significant independent risk factor for reduced survival rates in elderly ovarian cancer patients.1–3 Historically, clinical practice has demonstrated that satisfactory tumor cytoreduction (R0/R1 resection) is crucial for improving outcomes in patients with stage III and IV ovarian cancer. Over the past decade, surgical techniques for ovarian cancer have advanced significantly. To achieve R0 resection, surgeons often remove parts of the intestines, peritoneum, liver, spleen, and cardiophrenic lymph nodes. These procedures are extensive, lengthy, and highly invasive, resulting in significant surgical trauma and slow postoperative recovery for patients. However, most clinical trials have strict inclusion criteria, typically limiting participants to those under 70 years of age and excluding those with comorbidities. As the global population ages, the number of elderly individuals with multiple chronic diseases is increasing. Consequently, the number of patients who cannot undergo surgery due to advanced age or comorbidities is expected to rise. Does this mean that patients who do not undergo surgery are destined to have a poor prognosis? To explore this question, we conducted a retrospective analysis of the clinical outcomes of 15 patients who declined surgery due to comorbidities or advanced age.
Materials and methods
Study design and participants
This study is a retrospective clinical investigation. The inclusion criteria encompassed patients diagnosed with advanced epithelial ovarian cancer at our center (Department of Gynecology, Shengjing Hospital of China Medical University) from 2018 to 2023. Specifically, those who were either unable to undergo ovarian cancer tumor debulking surgery or subjectively refused it, and who had a survival duration of at least 6 months, were included. Comprehensive clinical data were collected for the enrolled patients, covering basic characteristics, treatment modalities, chemotherapy courses, treatment responses, progression-free survival (PFS), overall survival (OS), and other relevant parameters. As a retrospective study, this research has secured approval from the ethics committee for a waiver of informed consent.
Treatment methods
None of the patients underwent tumor cytoreductive surgery due to comorbidities or personal preferences. Instead, they received systemic intravenous chemotherapy for 3 to 6 cycles. In accordance with the guidelines, the first-line chemotherapy regimens included paclitaxel/liposomal doxorubicin combined with platinum-based regimens, or 2 sequential regimens based on the patient’s tumor assessment. Some patients also received bevacizumab in combination with their chemotherapy. Following chemotherapy, all but 3 patients received PARP inhibitor maintenance therapy. The exceptions were 2 patients who did not have access to PARP inhibitors at the time and one patient who was unable to afford the treatment. The basic clinical characteristics of the patients are summarized in Table 1. Detailed treatment information for all patients included in the study (designated as P1 to P15) is presented in Table 2.
Clinical efficacy evaluation standards and main study endpoints
Clinical efficacy evaluation
At the conclusion of initial chemotherapy, clinical efficacy was assessed according to the RECIST (Response Evaluation Criteria in Solid Tumors) version 1.1 criteria. The criteria encompass 4 categories: complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). Specifically, a CR is defined as the disappearance of all target lesions, with the short axis of any pathological lymph nodes (whether target or non-target) reduced to less than 10 mm. A PR indicates that the sum of the diameters of all target lesions has decreased by at least 30%. PD is characterized by an increase of at least 20% in the sum of the diameters of target lesions (Note: The appearance of one or more new lesions is also considered as disease progression). SD is defined as insufficient shrinkage to qualify for PR or insufficient enlargement to qualify for PD.
Primary endpoint
The primary endpoint of this study is PFS1, which is the time interval from the start of treatment to the first recurrence. Researchers evaluated the time from treatment initiation to tumor progression (in any aspect) in subjects according to the RECIST 1.1 criteria.
Secondary endpoints
The secondary endpoints include objective response rate (ORR), disease control rate (DCR), PFS2, and OS. PFS2 is defined as the time from the first radiological progression (RECIST 1.1) to the second radiological progression or death from any cause. Even if subsequent anti-tumor therapy (eg, second-line chemotherapy or targeted maintenance) is administered after initial progression, the PFS2 start date remains the date of first progression. The endpoint is the second radiological progression or death, whichever occurs first. The ORR refers to the proportion of patients whose tumor volume decreases to a predetermined value and can be maintained for the minimum required duration. It is calculated as the sum of the proportions of patients achieving CR and PR. The DCR is defined as the ratio of the sum of cases achieving either a response (PR + CR) or SD after treatment to the total number of evaluable cases.
Safety
The safety profile of the treatment was evaluated by assessing adverse events that occurred during the patients’ treatment. These events were graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE) to determine their occurrence and severity. The adverse reactions observed included both hematological toxicities (such as anemia, thrombocytopenia, neutropenia, and leukopenia) and non-hematological toxicities (such as elevated transaminase levels, fatigue, nausea, vomiting, and diarrhea).
Statistical analysis
Statistical analysis was conducted using SPSS 25.0 software. Qualitative data were presented as percentages. The Kaplan–Meier method was employed to analyze PFS and OS, including median PFS values, PFS rates, median OS values, and OS rates. Graphical representations were generated using R version 4.2.2. The significance level (α) was set at 0.05.
Results
Patient characteristics
Among the 15 patients included in the study, the median age was 73 years, with a range from 50 to 86 years. All patients were diagnosed with high-grade serous epithelial ovarian cancer. At baseline, 8 patients (54%) had an ECOG Performance Status (PS) score of 1, while 7 patients (46%) had a score of 2. Each patient had at least 2 metastatic sites. The median follow-up duration was 25 months, ranging from 13 to 80 months. The detailed baseline disease characteristics of the patients are presented in Table 1.
Treatment method
With the exception of patient P14, all other 14 patients received systemic intravenous chemotherapy with platinum-based plus paclitaxel/liposomal doxorubicin regimens, with or without the addition of intravenous bevacizumab. The standard treatment course consisted of 6 cycles. Among these patients, 5 (P1, P6, P7, P8, and P10) underwent sequential treatment with 2 first-line chemotherapy regimens. Additionally, 5 patients (P4, P5, P10, and P13) were unable to complete the full course of chemotherapy due to personal reasons or severe side effects encountered during treatment. Four patients (P4, P6, P8, and P9) received bevacizumab in combination with chemotherapy. Following chemotherapy, 12 patients who achieved disease control continued with PARP inhibitor maintenance therapy. Three patients (P3, P1, and P12) opted for observation after chemotherapy. Patient P14 initially declined intravenous chemotherapy and requested anti-angiogenic targeted therapy combined with immunotherapy. The comorbidities, reasons for not undergoing surgery, therapy regimens, reasons for incomplete treatment courses, and maintenance therapies for each patient are detailed in Table 2.
Efficacy
All 15 patients were included in the short-term efficacy evaluation. According to the RECIST 1.1 criteria, nobody achieved CR. Twelve out of 15 patients (80.0%) achieved PR, while 3 out of 15 patients (20.0%) had SD (see Table 2). The ORR was 80.0%, or 12 of 15 patients achieved PR. The DCR was 100% (15/15). The changes in target lesions compared to baseline are illustrated in Figure 1.
Treatment outcomes and survival analysis. (A) Best percentage change in tumor lesion size from baseline. A negative value indicates that the tumor size was smaller at follow-up compared to baseline. (B) Kaplan–Meier estimates of progression-free survival (PFS1). (C) Kaplan–Meier estimates of overall survival (OS). (D) Kaplan–Meier estimates of progression-free survival (PFS2).
The follow-up cutoff date was November 2024. For the 15 patients assessed by the investigators, the median PFS1 was 19.0 months (95% CI = 11.85-26.15), with a range from 9 to 66 months. The 1-year PFS rate was 80.0%, the 2-year PFS rate was 36.4%, and the 3-year PFS rate was 36.4% (see Figure 1). The median OS for the 15 patients was 57.0 months (95% CI = 13.00-100.99) (range 13-80 months). The 1-year OS rate was 100.0%, the 2-year OS rate was 91.7%, and the 3-year OS rate was 65.2% (see Figure 1). Among the 10 patients who received subsequent treatment after the first recurrence, the median PFS2 was 10 months (see Figure 1).
The PFS1, PFS2, and OS results for each patient are detailed in Table 2. In this study, we conducted a comparative analysis of CT images before and after treatment for selected patients. The comparative analysis of CT images for these patients is presented in Figure 2.
Comparison of CT images before and after treatment. (A) 1-3. Patient P6. (B) 1-2. Patient P9. (C) Patient P10. The lesion indicated by the arrow corresponds to the baseline lesion prior to treatment.
Safety
All 15 patients were included in the safety analysis (see Table S1). The most common hematological toxicities included leukopenia (93.3%), with a grade 1-2 incidence of 73.3%; neutropenia (93.3%), with a grade 1-2 incidence of 53.3%; and thrombocytopenia (73.3%), all of which were grade 1-2. The primary non-hematological toxicities were fatigue (100%), vomiting (100%), and nausea (100%), all of which were grade 1-2.
Discussion
After decades of clinical practice and exploration, primary debulking surgery has long been the preferred treatment for patients with stage III and IV ovarian cancer. Achieving satisfactory tumor cytoreduction (R0/R1) is a crucial determinant of patient survival. To meet the R0/R1 surgical standards, it is often necessary to resect parts of the bowel, peritoneum, liver, spleen, and other organs. This can subject patients to significant surgical trauma and prolonged postoperative recovery. In cases where advanced ovarian cancer patients have extensive tumor involvement and satisfactory debulking cannot be achieved, neoadjuvant chemotherapy followed by interval debulking surgery serves as a viable alternative.4–8
However, patients in those randomized controlled trials are typically selected based on strict inclusion criteria, often being under the age of 70 and free from comorbidities. With the increasing aging population and extended human lifespan, approximately 70% of elderly patients have at least one chronic disease, and a significant proportion may have 2 to 3 comorbidities. The proportion of elderly patients with ovarian cancer is expected to continue rising, and these patients face significantly higher perioperative risks, postoperative severe complication rates, and mortality rates.4–6 In the real world, how should clinicians make informed decisions for such patients?
In this study, the median age of the 15 patients was 73 years. Seven patients (46%) had an ECOG score of 2, and among them, 3 had absolute contraindications to surgery. This reflects the current state of real-world clinical practice, where elderly patients and those with multiple comorbidities often have compromised organ function. This not only increases the risks associated with the perioperative period but also means that even the choice of chemotherapy alone requires careful consideration. In this study, 5 patients were unable to complete the full course of chemotherapy due to intolerable side effects, and among them, 3 were evaluated to have SD. Nevertheless, the DCR of this study reached 100%, with a median PFS1 of 19.0 months and a 1-year PFS rate of 80%. Even patients with SD achieved a minimum PFS1 of 11 months. In this small-sample retrospective cohort, non-surgical treatment demonstrated potential signals of benefit, though validation through large-scale studies is still required.
It is widely recognized that the advent of PARP inhibitors has been a significant boon for patients with ovarian cancer. The current standard treatment paradigm for ovarian cancer includes surgery, chemotherapy (typically paclitaxel and platinum-based agents), targeted therapy (such as bevacizumab), and maintenance therapy with PARP inhibitors.9–12 In this study, 12 patients received PARP inhibitors (including fluzoparib and niraparib) for maintenance therapy. One patient was unable to receive PARP inhibitors due to financial constraints, while another 2 patients did not use PARP inhibitors because there were no frontline data available for the entire population before 2019.
In this study, the median PFS1 was 19.0 months. This is comparable to the median PFS of 13.8 months observed in the entire population of the PRIMA study13 and the median PFS of 19.6 months in the single-arm clinical study OVARIO.14 Notably, some patients in this study received only 3 cycles of chemotherapy and were assessed as having SD, yet they still achieved a considerably extended survival period. This extended survival may be attributed to the sequential synergistic anti-tumor effect of PARP inhibitors in combination with chemotherapy.
Cancer treatment has now entered the immunotherapy era. Combining immune checkpoint inhibitors (ICIs) with chemotherapy or targeted therapies has achieved breakthroughs in treating many solid tumors. However, progress in treating recurrent and later-line ovarian cancer with ICIs has been limited. Studies show that the response rate to ICI monotherapy in ovarian cancer patients is only 10% to 15%.15 ICIs work by activating T cells to fight tumors, and their effectiveness largely depends on T cell infiltration in the tumor tissue.16
Most ovarian cancer recurrences occur in the pelvic and abdominal regions. The omentum and pelvic lymph nodes, often removed during initial treatment, are peripheral immune organs that store mature lymphocytes and filter harmful substances, including tumor cells, from lymphatic fluid. In this study, patients received up to 6 cycles of initial chemotherapy, but about one-third completed only 3 to 4 cycles due to health reasons. Despite achieving only SD, these patients had a median PFS1 of 19 months. Could preserving the omentum and pelvic lymph nodes help maintain immune balance and control tumor progression?
Among the 10 patients with recurrence who were evaluable for PFS2, the median PFS2 was 10 months. Patients remained sensitive to chemotherapy after recurrence. For example, Patient P10 experienced 4 recurrences, using only chemotherapy and bevacizumab without PARP inhibitors, and each chemotherapy course was limited to 4 cycles, yet each PFS exceeded 6 months. The patient lived with the tumor for 57 months and ultimately died of cerebral hemorrhage, not cancer. Patient P14, an 81-year-old with multiple comorbidities (liver cancer, cirrhosis, and splenomegaly), controlled the disease for 11 months using bevacizumab and immunotherapy without chemotherapy. After progression, combining PARP inhibitors with immunotherapy controlled the disease for another 3 months. We speculate that ICIs played a significant role in this patient’s treatment.
The sample size of this study was relatively small (only 15 cases), resulting in limited statistical power; therefore, the results should be interpreted with caution. The findings of this study should be regarded as exploratory. We strongly recommend that future large-scale, prospective studies be conducted to further validate these findings.
Conclusions
The patients in this study were either elderly or had significant comorbidities and poor physical conditions. Despite not undergoing surgery, they achieved a median OS of 57.0 months, with a 1-year OS rate of 100.0%, a 2-year OS rate of 91.7%, and a 3-year OS rate of 65.2% through comprehensive treatment. These outcomes are comparable to previously reported standard treatments.
Our study provides an alternative treatment option for elderly ovarian cancer patients. Future considerations could include using chemotherapy ± bevacizumab plus ICIs for initial treatment, followed by PARP inhibitors for maintenance therapy after disease control. We do not advocate replacing existing guidelines or making our approach the preferred method. Future prospective, multicenter clinical trials should be conducted to validate and optimize the non-surgical treatment strategy proposed in this study.
Supplementary Material
oyaf290_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liontos M , Papatheodoridi A, Andrikopoulou A, et al Management of the elderly patients with high-grade serous ovarian cancer in the REAL-WORLD setting [published online ahead of print April 04, 2021]. Curr Oncol. 2021;28:1143-1152. 10.3390/curroncol 2802011033800101 PMC 8025751 · doi ↗ · pubmed ↗
- 2van Walree IC , van Soolingen NJ, Hamaker ME, et al Treatment decision-making in elderly women with ovarian cancer: an age-based comparison [published online ahead of print January 15, 2019]. Int J Gynecol Cancer. 2019;29:158-165. 10.1136/ijgc-2018-00002630640699 · doi ↗ · pubmed ↗
- 3Tew WP. Ovarian cancer in the older woman [published online ahead of print August 09, 2016]. J Geriatr Oncol. 2016;7:354-361. 10.1016/j.jgo.2016.07.00827499341 · doi ↗ · pubmed ↗
- 4Long Roche K , Chi DS. Practical guidelines for triage to neoadjuvant chemotherapy in advanced ovarian cancer: big risk, big reward…or too much risk? [published online ahead of print June 13, 2020]. Gynecol Oncol. 2020;157:561-562. 10.1016/j.ygyno.2020.05.00332527446 PMC 7279726 · doi ↗ · pubmed ↗
- 5Narasimhulu DM , Kumar A, Weaver AL, et al Less guessing, more evidence in identifying patients least fit for cytoreductive surgery in advanced ovarian cancer: a triage algorithm to individualize surgical management [published online ahead of print April 06, 2020]. Gynecol Oncol. 2020;157:572-577. 10.1016/j.ygyno.2020.03.02432247602 PMC 7293555 · doi ↗ · pubmed ↗
- 6Straubhar AM , Wolf JL, Zhou MQC, et al Advanced ovarian cancer and cytoreductive surgery: independent validation of a risk-calculator for perioperative adverse events [published online ahead of print December 05, 2020]. Gynecol Oncol. 2021;160:438-444. 10.1016/j.ygyno.2020.11.02133272645 PMC 7856180 · doi ↗ · pubmed ↗
- 7Nishio S , Ushijima K. Clinical significance of primary debulking surgery and neoadjuvant chemotherapy-interval debulking surgery in advanced ovarian cancer [published online ahead of print February 23, 2020]. Jpn J Clin Oncol. 2020;50:379-386. 10.1093/jjco/hyaa 01532083282 · doi ↗ · pubmed ↗
- 8Angeles MA , Rychlik A, Cabarrou B, et al A multivariate analysis of the prognostic impact of tumor burden, surgical timing and complexity after complete cytoreduction for advanced ovarian cancer [published online ahead of print July 28, 2020]. Gynecol Oncol. 2020;158:614-621. 10.1016/j.ygyno.2020.06.49532709536 · doi ↗ · pubmed ↗