Comparison of ischemic cardiovascular events between dapagliflozin and empagliflozin in combination with metformin: A nationwide population-based cohort study
Hayeon Kim, Seung Won Lee, Yejee Lim, Nayoung Han, Suin Kang, Youngjoo Byun, Kyungim Kim

TL;DR
This study compares dapagliflozin and empagliflozin in type 2 diabetes patients to see if one is better at preventing heart and blood vessel issues when used with metformin.
Contribution
It provides real-world evidence on the comparative effectiveness of two SGLT-2 inhibitors for cardiovascular outcomes in Asian patients with T2DM.
Findings
No significant difference in composite ischemic CVD events between dapagliflozin and empagliflozin when combined with metformin.
Findings suggest similar cardiovascular risk profiles for both drugs in real-world settings.
Results were consistent across individual components of CVD events and mortality.
Abstract
The comparative effectiveness of individual sodium–glucose cotransporter-2 inhibitors (SGLT-2is) in preventing ischemic cardiovascular disease (CVD) remains uncertain. Thus, this study compared the incidence of ischemic CVD events in patients with type 2 diabetes mellitus (T2DM) treated with dapagliflozin or empagliflozin in combination with metformin. This retrospective cohort study analyzed national claims data from the Korean National Health Insurance Service. Patients with T2DM who received dapagliflozin or empagliflozin, combined with metformin, between 2014 and 2019 were included. The primary outcome was composite ischemic CVD events, defined as myocardial infarction, ischemic stroke, or coronary revascularization. Secondary outcomes included each component of composite ischemic CVD events, unstable angina, and all-cause mortality. Hazard ratios (HRs) and confidence intervals…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
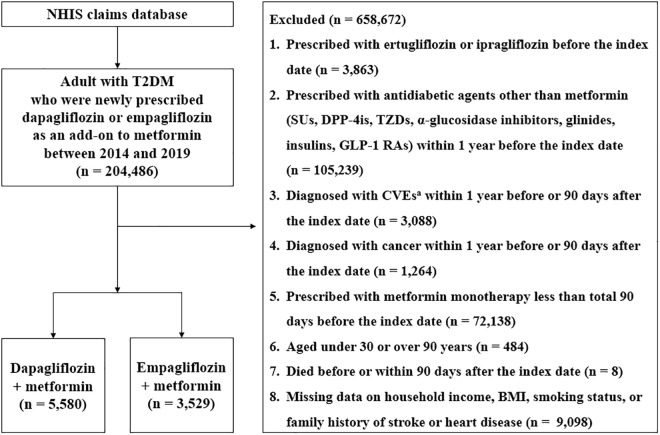 Fig 1
Fig 1- —the National Research Foundation of Korea
- —Korea University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Metabolism, Diabetes, and Cancer · Chronic Lymphocytic Leukemia Research
Introduction
Type 2 diabetes mellitus (T2DM) is a representative chronic disease and a significant public health concern, placing a substantial burden not only on individuals but also on society. Globally, the age-standardized incidence rate of T2DM was 184.6 per 100,000 people in 2017 and is projected to rise to 284.4 per 100,000 people in the 2030s [1]. Diabetes is also associated with a reduction in life expectancy by approximately 10 years [2], and two-thirds of deaths among patients with T2DM are attributed to cardiovascular disease (CVD) [3]. Macrovascular disease, particularly of cardiac origin, is a common complication of T2DM. Studies have shown that patients with T2DM have a 1.5 to 2.3 times higher risk of cardiovascular death than the nondiabetic population [4–6]. Therefore, current T2DM management guidelines emphasize not only blood glucose control but also strategies for CVD prevention [7].
Sodium-glucose cotransporter-2 inhibitors (SGLT-2is) have shown significant clinical benefits for CVD in patients with T2DM. Large-scale randomized controlled trials (RCTs) and real-world studies have confirmed the positive effects of SGLT-2is on key cardiovascular outcomes, including major adverse cardiovascular events, cardiovascular death, and hospitalization for heart failure [8–10]. Consequently, there is a growing interest in investigating whether different SGLT-2is subtypes have varying effects on reducing the risk of CVD. In previous RCTs, varying degrees of effects in reducing CVD risk have been reported for two widely prescribed SGLT-2is, dapagliflozin and empagliflozin [8,11,12]. However, no RCTs have directly compared the two SGLT-2is. Some network meta-analyses have evaluated their differences in reducing CVD risk, but the findings remain inconclusive [13–16]. Furthermore, these studies have limitations as they combined data from both RCTs and observational studies or relied on indirect analyses mediated using a placebo. Several retrospective cohort studies have compared the risk of CVD between dapagliflozin and empagliflozin [17–21]. However, these cohort studies did not restrict the background antidiabetic agent class, and the study population received various antidiabetic combinations, making it difficult to isolate SGLT-2is-specific effects. Because the extent of antidiabetic agent use often reflects diabetes severity, a key confounder for CVD, the homogeneity of the underlying antidiabetic regimens is essential [22,23]. Moreover, certain antidiabetic agents may directly affect CVD risk [24–26], further complicating the interpretation of study results.
While dapagliflozin and empagliflozin show pharmacokinetic (PK) and pharmacodynamic (PD) differences, there is no evidence for a clinically meaningful difference in glycemic control; thus, agent selection can be individualized by comorbidities [27–30]. In this context, understanding differences in CVD risk reduction across SGLT-2is subtypes may help tailor their use in clinical practice. Therefore, this study aimed to compare the risk of subsequent ischemic CVD events in adults with T2DM who initiated dapagliflozin or empagliflozin, both combined with metformin, using nationwide claims data from South Korea. Previous studies have shown that metformin, the first-line antidiabetic agent commonly used in combination with SGLT-2is in clinical practice, has no effect on CVD incidence [31,32]. Moreover, it has been reported that combination of metformin with either empagliflozin or dapagliflozin exhibits no clinically meaningful differences in glucose-lowering effects or serious adverse effects, regardless of which SGLT-2i is used [29,30]. Therefore, the present study restricted baseline antidiabetic agents to metformin to better reflect real-world practice, ensure homogeneity of the study group, and enable a clearer comparison of the effects of SGLT-2is.
Materials and methods
Data source
This retrospective, nationwide, population-based cohort study was conducted using customized data from the National Health Insurance Service (NHIS) claims data of South Korea. The NHIS is a national healthcare insurance system covering 97% of the Korean population. Its claims database provides anonymized, longitudinal health data, including sociodemographic information, medical diagnoses (coded using the International Classification of Diseases, Tenth Revision [ICD-10]), therapeutic procedures, drug prescriptions (prescription date, supply duration, dosage, and administration route), and healthcare use type (outpatient, inpatient, or emergency department). The structure of the NHIS data has been detailed in a previous publication [33]. The NHIS also provides health checkup data, including physical examination results (height, weight, and blood pressure); selected laboratory test findings (low-density lipoprotein cholesterol [LDL-C], fasting blood glucose [FBG], serum creatinine [SCr], total cholesterol, triglycerides, high-density lipoprotein cholesterol, hemoglobin, liver function tests, and urinalysis); and information on personal and family medical history, and health-related behaviors, such as smoking status and alcohol consumption. These data are collected through annual or biennial general health checkups for NHIS-insured individuals and their dependents. For this study, both the claims and the health checkup data from the NHIS were used.
The study was approved by the Institutional Review Board of Korea University (KUIRB-2021-0036-01) and the Korea NHIS National Health Information Data Request Review Committee (NHIS 2021-1-410). The requirement for informed consent was waived because NHIS provided anonymized data. All data used in this study were fully anonymized before being accessed by the researchers. Therefore, the authors had no access to any information that could identify individual patients during and after data collection. Data used for this study were accessed for research purposes from March 24, 2021, to March 23, 2023. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline [34].
Study population
From the NHIS database, which includes approximately 100 million individuals, this study identified adults aged 30–90 years with T2DM who were newly prescribed dapagliflozin or empagliflozin as an add-on to metformin between 2014 and 2019. Patients with T2DM were defined as individuals who met the following two criteria: a primary or subdiagnosis of T2DM (ICD-10 code E11) and at least one prescription history for an antidiabetic agent. This operational definition was validated in a Korean study using NHIS claims data with high specificity and accuracy and is consistent with Canadian validation findings showing that diagnosis-plus-prescription algorithms achieve very high specificity [35,36]. Patients were included if they had received metformin monotherapy for at least 90 days before adding SGLT-2is to minimize the possibility of metformin-induced glycemic fluctuations. This 90-day duration was selected based on previous studies indicating that metformin provides no statistically significant additional blood glucose–lowering effects after approximately 3 months (90 days) [37,38]. The initiation date of dapagliflozin or empagliflozin was designated as the index date. To ensure comparability between the treatment groups and assess the actual effects of each SGLT-2i, this study excluded patients treated with antidiabetic agents other than metformin within 1 year before the index date. Additionally, individuals who had previously used other subtypes of SGLT-2is (such as ertugliflozin or ipragliflozin) before the index date were also excluded. To minimize the impact of pre-existing CVD events or cancer on the study outcomes, individuals with a history of ischemic heart disease (I20–I25), heart failure (I50), cerebrovascular disease (I60–I69), coronary revascularization (percutaneous coronary intervention or coronary artery bypass graft), or transient cerebral ischemic attack (G45) were excluded. Patients diagnosed with any cancer type within 1 year before or 90 days after the index date were also excluded. The exclusion criterion for pre-existing CVD events was based on evidence suggesting that most recurrent CVD events tend to occur within the first year following the initial episode [39,40]. The study selection process is presented in Fig 1.
Flow diagram of the study population.This cohort study used customized Korean claims data from the NHIS database. Patients with T2DM who newly initiated dapagliflozin or empagliflozin as an add-on to metformin between 2014 and 2019 were identified. After applying predefined exclusion criteria, 9,109 eligible patients remained, including 5,580 treated with dapagliflozin and 3,529 with empagliflozin. aCVEs include ischemic heart diseases (I20–I25), coronary revascularization (procedure codes: M6551, M6552, M6561, M6563, M6564, M6571, M6572, O1641, O1642, O1647, OA641, OA642, and OA647), heart failure (I50), cerebrovascular disease (I60–I69), or transient cerebral ischemic attack (G45). Abbreviations: BMI, body mass index; CVEs, cardiovascular events; DPP-4is, dipeptidyl peptidase-4 inhibitors; GLP-1RAs, glucagon-like peptide-1 receptor agonists; SUs, sulfonylureas; T2DM, type 2 diabetes mellitus; TZDs, thiazolidinediones.
Study outcomes
The primary outcome was composite ischemic CVD events, defined as a patient hospitalized or visited the emergency department for myocardial infarction (MI) (I21–I23), coronary revascularization procedures (M6551, M6552, M6561, M6563, M6564, M6571, M6572, O1641, O1642, O1647, OA641, OA642, OA647), or ischemic stroke (I63). The secondary outcomes included individual components of the composite ischemic CVD events, unstable angina (I20.0), and all-cause mortality. Study outcomes were determined based on at least one record of hospitalization or emergency department visit with the corresponding diagnostic or procedure code as the primary or first subdiagnosis. Patients were followed from 90 days after the index date until the first occurrence of the study outcome, death from any cause, or the end of the study (December 31, 2019), whichever occurred first. The 90-day lag period was prespecified to account for the induction/latency period required for SGLT-2is to affect ischemic CVD risk and to reduce reverse causation. This design is supported by large-scale RCTs on dapagliflozin and empagliflozin, which showed that cardiovascular benefits typically emerged approximately 3 months after initiation [11,12,41]. The same lag was applied to both study groups to minimize differential immortal time [42].
Covariates
The study covariates included age, sex, metformin monotherapy duration, index year, household income, region of residence, Charlson comorbidity index (CCI), comorbidities, comedications, and health checkup data. The duration of metformin monotherapy was defined as the period during which metformin was used alone before adding dapagliflozin or empagliflozin, starting in 2013. CCI scores were calculated based on patients’ disease records using previously validated algorithms [43]. Comorbidities included hypertension, dyslipidemia, atrial fibrillation, chronic kidney disease, microvascular complications of diabetes, and rheumatoid arthritis, all diagnosed within 1 year before the index date. Comedications were defined as antihypertensive, antihyperlipidemic, antiplatelet, and anticoagulant agents prescribed for more than total 90 days within 1 year before the index date. The relevant ICD-10 codes and generic names for comorbidities and comedications are provided in S1 and S2 Tables. Health checkup data recorded within 2 years before the index date were included as covariates. These variables comprised body mass index (BMI), smoking status, family history of stroke or heart disease (MI or angina pectoris), systolic blood pressure (SBP), LDL-C, FBG, and SCr.
Statistical analyses
Baseline characteristics of the dapagliflozin and empagliflozin groups were presented as frequencies and percentages and compared using the χ^2^ test. Cox proportional hazards regression models were used to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for the risk of composite ischemic CVD events in the empagliflozin group relative to the dapagliflozin group. Crude and adjusted HR (aHR) were estimated for individual components of composite ischemic CVD events, unstable angina, and all-cause mortality. The covariates were adjusted in three sequential models to show the incremental impact of broader baseline information on the effect estimates: Model 1 adjusted for age and sex; Model 2 adjusted for the variables in Model 1 as well as metformin monotherapy duration, index year, comorbidities, CCI score, comedications, BMI, smoking status, and family history of stroke or heart disease; and Model 3 adjusted for the variables in Model 2 along with specific clinical parameters from health checkup data (SBP, LDL-C, FBG, and SCr) measured within 2 years before the index date. Because Model 3 represented the fully adjusted and most conservative specification, it served as the primary basis for inference.
Subgroup analyses were conducted to assess crude HR and aHR in Model 2 for composite ischemic CVD events, stratified by age group, sex, BMI, FBG, estimated glomerular filtration rate (eGFR), and LDL-C. However, due to the small sample size in each subgroup in Model 3, further subgroup analyses for Model 3 were not conducted. All analyses followed an intention-to-treat approach and were conducted using SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA). A two-sided p-value of <0.05 was considered statistically significant.
Results
Study population and baseline characteristics
This study included 9,109 patients who were newly prescribed SGLT-2is as an add-on to metformin, with 5,580 receiving dapagliflozin and 3,529 receiving empagliflozin (Fig 1). Detailed baseline characteristics are presented in Table 1. The mean follow-up duration was 747.6 ± 495.9 days for the dapagliflozin group and 529.5 ± 341.9 days for the empagliflozin group. The mean age was 52.82 ± 9.78 for dapagliflozin group and 53.86 ± 9.83 for empagliflozin group.
Table 1: Baseline characteristics of dapagliflozin and empagliflozin groups.
Comparative risk of ischemic CVD events among patients using different SGLT-2is
A total of 55 and 10 composite ischemic CVD events occurred in the dapagliflozin and empagliflozin groups, respectively. In Models 1 and 2, patients newly treated with empagliflozin showed an approximately 55% lower risk of composite ischemic CVD events than those receiving dapagliflozin (aHR 0.42, 95% CI: 0.21–0.84; aHR 0.48, 95% CI: 0.23–0.98, respectively). However, in Model 3, after fully adjusting for all covariates, including clinical parameters—SBP, LDL-C, FBG, and SCr—the significant difference between empagliflozin and dapagliflozin groups was no longer observed (aHR 0.50, 95% CI: 0.24–1.03; Table 2). Additionally, across all three adjusted models, there were no significant differences between dapagliflozin and empagliflozin groups in the risk of individual components of composite ischemic CVD events, unstable angina, and all-cause mortality (Table 2).
Table 2: Risk comparison of ischemic CVD events between dapagliflozin and empagliflozin groups.
Subgroup analysis
Subgroup analysis was conducted by stratifying patients based on age group, sex, BMI, FBG, eGFR, and LDL-C to assess the risk of composite ischemic CVD events. Both crude HR and aHR from Model 2 were reported. Overall, the results showed no significant differences between dapagliflozin and empagliflozin groups, except for patient group with eGFR levels between 60 and 90 mL/min/1.73m^2^ (S3 Table).
Discussion
This retrospective cohort study assessed whether the risk of ischemic CVD events differed between dapagliflozin and empagliflozin, used as add-on therapies to metformin, among adults with T2DM. Using three stepwise-adjusted models, the results from Models 1 and 2 showed a potential difference in risk. However, in the fully adjusted Model 3, no significant difference in risk was observed between dapagliflozin and empagliflozin. Additionally, the two SGLT-2is showed no significant differences in the individual components of composite ischemic CVD events, unstable angina, and all-cause mortality in any of Models 1–3, supporting the conclusion that there were no statistically significant between-drug differences in reducing the incidence of ischemic CVD events.
In this study, Model 3 adjusted for key clinical parameters, including SBP, LDL-C, FBG, and SCr, in addition to traditional covariates such as comorbidities, an approach consistent with previous studies [19,21,44,45]. This approach was employed because the incidence of ischemic CVD events can be influenced by the presence of disease as well as by its severity, and incorporating these parameters allows for a more accurate reflection of the underlying disease state. These four clinical parameters are well-established risk factors for ischemic CVD events. SBP, a known risk factor for ischemic heart disease and stroke, has a documented positive association with the risk of both conditions [46,47]. LDL-C is supported by both clinical and genetic evidence as a correlate of atherosclerotic CVDs, including MI and stroke [48,49]. The atherogenic potential of LDL-C, such as its role in atherosclerotic plaque formation and acceleration of inflammatory processes, may contribute to ischemic CVD events [48]. Furthermore, impaired FBG level is a significant risk factor for ischemic CVD events, as abnormal glucose levels can induce endothelial dysfunction and promote plaque formation [50,51]. Decreased eGFR, as determined by creatinine levels, is associated with a higher risk of future ischemic CVD events [52,53]. High SCr levels are linked to endothelial dysfunction and contribute to increased cardiovascular risk by placing additional strain on the heart [54]. Therefore, by including these four significant risk factors as covariates, the present study offers more comprehensive and reliable findings on the development of ischemic CVD events.
Differences in the PK and PD properties of dapagliflozin and empagliflozin have been documented. Previous studies have reported that empagliflozin has greater selectivity for SGLT-2 over SGLT-1 and reaches peak concentration faster than dapagliflozin, whereas dapagliflozin has a slightly longer half-life, higher protein binding, and a larger volume of distribution [27,28]. However, differential effects on clinical parameters, such as HbA1c, FBG, and BMI, remain inconclusive [29,30,55,56]. Furthermore, it remains unclear whether differences in PK or PD properties translate into distinct effects on ischemic CVD events. Notably, a meta-regression analysis found no correlation between the magnitude of HbA1c reduction from SGLT-2is use and the incidence of CVD events [57]. These results imply that the development and manifestation of ischemic CVD events likely result from the complex interplay of multiple factors. In this context, the findings of current study—where significant differences in ischemic CVD events were observed between dapagliflozin and empagliflozin in Models 1 and 2, but not in Model 3 which adjusted for key clinical parameters—can be better understood.
Previous cohort studies have reported comparable effects of dapagliflozin and empagliflozin on subsequent cardiovascular outcomes [17–21]. While the results are similar, the current study differentiates itself in its design. Restricting the study population to patients receiving a combination of metformin and SGLT-2i provides a more controlled comparison between the two treatment groups. The type and number of antidiabetic agents used may reflect a patient’s glycemic control status or disease severity [23]. A previous study has shown that the duration for which HbA1c levels remain above target is positively associated with the number of antidiabetic agents used [58]. Additionally, different antidiabetic agents and their combinations may have varying effects on diabetes progression and subsequent ischemic CVD events [59]. For example, some antidiabetic agents, such as sulfonylureas, have been suggested to increase CVD risk patients with T2DM [60]. In this context, the current study focuses on patients who received dapagliflozin or empagliflozin as an add-on to metformin, offering more substantive evidence by comparing the distinct effects of these two SGLT-2is within a homogenous patient group—an approach that distinguishes it from previous studies.
This study has several key strengths. First, this study used comprehensive, nationwide healthcare data encompassing most of the South Korean population. Second, to enhance the robustness of the study, multivariable adjustments were performed incorporating health checkup data as covariates, including smoking status, family history of stroke or heart disease, and clinical parameters associated with ischemic CVD events [61,62]. By fully adjusting for potential risk factors for ischemic CVD events, this study effectively minimizes confounding effects.
Despite its strengths, this study has several limitations. First, because of the inherent limitations of claims and health checkup data, unmeasured or unknown residual confounding factors cannot be excluded. In particular, since information on HbA1c and diabetes duration was unavailable, data on FBG—the only available glycemic measure—were used for adjustment. However, considering that FBG may not fully reflect long-term glycemic control, residual confounding likely persisted and may have affected the results. Second, this study cannot rule out the possibility of selection bias. To ensure population homogeneity, individuals who had been treated with other antidiabetic agents within 1 year prior to the index date were excluded. This approach may have biased the study population toward patients with T2DM at earlier disease stages or those whose condition was relatively well controlled with metformin monotherapy. Moreover, the average participation rate in the general health checkup program during the study period was 75.4% [63]. Model 3 excluded individuals without health checkup data, which may have introduced bias related to data missing not at random (MNAR). Nevertheless, considering that even patients with early-stage diabetes have a higher risk for CVD and a greater need for risk factor management than the general population [64–67], examining CVD risk in this population still provides clinically meaningful insights. However, caution is warranted when interpreting and applying these findings. Third, a temporal difference in enrollment was observed between dapagliflozin and empagliflozin users, as empagliflozin was covered by the NHIS later than dapagliflozin in Korea. Although the index year was adjusted in the multivariate analyses in Models 2 and 3, the possibility that it may act as a time-related confounder cannot be ruled out. Finally, the small number of outcome events in this study may have limited its statistical power. However, the incidence of ischemic CVD events in Korean patients with T2DM has been reported to be lower than that in other countries [68–71], with previous Korean studies demonstrating event rates comparable to those observed in our study [18–20]. Moreover, the relatively healthy study population—consisting of patients with early-stage or well-controlled diabetes managed with metformin monotherapy, and a high proportion of patients in their 50s—may have contributed to the low event rates. Therefore, further studies with longer follow-up durations are warranted to address these limitations and improve the accuracy and generalizability of the findings.
In this nationwide cohort study, after adjustment for potential risk factors, including key clinical parameters, no significant difference in the risk of ischemic CVD events was observed between dapagliflozin and empagliflozin in combination with metformin in patients with T2DM. This finding provides real-world evidence that neither agent showed statistically significant superiority over the other in reducing the incidence of ischemic CVD events.
Supporting information
S1 TableList of outcomes and comorbidities with corresponding codes.Abbreviations: ICD-10, International Classification of Diseases 10th revision.(PDF)
S2 TableList of drugs used for the covariates with corresponding codes.Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ADP, adenosine diphosphate; ARB, angiotensin receptor blocker; BB, beta-blocker; CCB, calcium channel blocker; COX, cyclooxygenase; DU, diuretic; LMWH, low molecular weight heparin; PCSK9, proprotein convertase subtilisin/kexin type 9; PDE, phosphodiesterase; UFH, unfractionated heparin.(PDF)
S3 TableSubgroup analysis for composite ischemic CVD events.Composite ischemic CVD events include MI, coronary revascularization, or ischemic stroke. Bold values indicate statistical significance. ^a^Hazard ratios were adjusted for age, sex, metformin monotherapy duration, index year, household income, region of residence, comorbidities (hypertension, dyslipidemia, atrial fibrillation, chronic kidney disease, microvascular complications of diabetes [diabetic retinopathy, neuropathy, and nephropathy], and rheumatoid arthritis), CCI, comedications (antihypertensive, antihyperlipidemic, antiplatelet, and anticoagulant agents), BMI, smoking status, and family history of stroke or heart disease. ^b^The BMI < 18.5 kg/m^2^ group (n = 9) and FBG < 70 mg/dL group (n = 3) are omitted because of the small total number of patients. Abbreviations: CVD, cardiovascular disease; DAPA, dapagliflozin; EMPA, empagliflozin; MET, metformin; BMI, body mass index; CCI, Charlson comorbidity index; CI, confidence interval; eGFR, estimated glomerular filtration rate; FBG, fasting blood glucose; HR, hazard ratio; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction.(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ye J, Wu Y, Yang S, Zhu D, Chen F, Chen J, et al. The global, regional and national burden of type 2 diabetes mellitus in the past, present and future: a systematic analysis of the Global Burden of Disease Study 2019. Front Endocrinol (Lausanne). 2023;14:1192629. doi: 10.3389/fendo.2023.1192629 37522116 PMC 10376703 · doi ↗ · pubmed ↗
- 2Emerging Risk Factors Collaboration. Life expectancy associated with different ages at diagnosis of type 2 diabetes in high-income countries: 23 million person-years of observation. Lancet Diabetes Endocrinol. 2023;11(10):731–42. doi: 10.1016/S 2213-8587(23)00223-1 37708900 PMC 7615299 · doi ↗ · pubmed ↗
- 3Cavallari I, Bhatt DL, Steg PG, Leiter LA, Mc Guire DK, Mosenzon O, et al. Causes and Risk Factors for Death in Diabetes: A Competing-Risk Analysis From the SAVOR-TIMI 53 Trial. J Am Coll Cardiol. 2021;77(14):1837–40. doi: 10.1016/j.jacc.2021.02.030 33832610 · doi ↗ · pubmed ↗
- 4Emerging Risk Factors Collaboration, Sarwar N, Gao P, Seshasai SRK, Gobin R, Kaptoge S, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215–22. doi: 10.1016/S 0140-6736(10)60484-9 20609967 PMC 2904878 · doi ↗ · pubmed ↗
- 5Barnett KN, Ogston SA, Mc Murdo ME, Morris AD, Evans JM. A 12-year follow-up study of all-cause and cardiovascular mortality among 10,532 people newly diagnosed with Type 2 diabetes in Tayside, Scotland. Diabet Med. 2010;27:1124–9. doi: 10.1111/j.1464-5491.2010.03075.x 20854379 · doi ↗ · pubmed ↗
- 6Eberly LE, Cohen JD, Prineas R, Yang L, Intervention Trial Research group. Impact of incident diabetes and incident nonfatal cardiovascular disease on 18-year mortality: the multiple risk factor intervention trial experience. Diabetes Care. 2003;26(3):848–54. doi: 10.2337/diacare.26.3.848 12610048 · doi ↗ · pubmed ↗
- 7Kelsey MD, Nelson AJ, Green JB, Granger CB, Peterson ED, Mc Guire DK, et al. Guidelines for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes: JACC Guideline Comparison. Journal of the American College of Cardiology. 2022;79:1849–57. doi: 10.1016/j.jacc.2022.02.04635512864 PMC 8972581 · doi ↗ · pubmed ↗
- 8Mc Guire DK, Shih WJ, Cosentino F, Charbonnel B, Cherney DZI, Dagogo-Jack S, et al. Association of SGLT 2 Inhibitors With Cardiovascular and Kidney Outcomes in Patients With Type 2 Diabetes: A Meta-analysis. JAMA Cardiol. 2021;6(2):148–58. doi: 10.1001/jamacardio.2020.4511 33031522 PMC 7542529 · doi ↗ · pubmed ↗