Tricuspid valve endocarditis in a horse owner, caused by Streptococcus equi subsp. zooepidemicus
C. Nicholas Roy, Catherine E. Wiechmann, Ameesh Dev, Brandon K. Walther, James M. Musser, Randall J. Olsen, Stephen B. Beres, Dierdre B. Axell-House

TL;DR
A horse owner developed a rare heart infection caused by bacteria linked to animals, highlighting the importance of considering animal exposure in diagnosing such cases.
Contribution
This is the first reported case of tricuspid valve endocarditis caused by Streptococcus equi subsp. zooepidemicus in a human.
Findings
The patient's infection was caused by a strain of Streptococcus equi subsp. zooepidemicus genetically linked to a Brazilian outbreak.
The infection required valve replacement and repair despite antibiotic treatment.
The case emphasizes the importance of exposure history in diagnosing zoonotic infections.
Abstract
Streptococcus equi subsp. zooepidemicus (SESZ) are zoonotic group C streptococci primarily acquired from contact with horses and other animals, such as llamas. They are unusual causes of infection in humans and rarely cause infective endocarditis. A 58-year-old woman presented with fever, malaise, and polyarthritis. Clinical evaluation diagnosed native tricuspid valve SESZ endocarditis. The SESZ isolate was genetically closely related to a clone causing an outbreak of post-streptococcal glomerulonephritis linked to the consumption of unpasteurized cheese in Brazil. The patient had no exposure to unpasteurized cheese but rode horses. Her infection course was notable for persistent fever despite combination antibiotic therapy. Resolution of her symptoms ultimately required tricuspid valve and aortic valve replacement and mitral valve repair. This is the first reported case of native…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig 1
Fig 1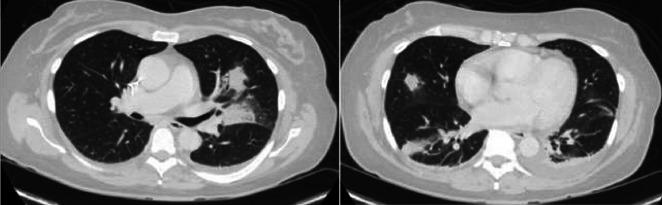 Fig 2
Fig 2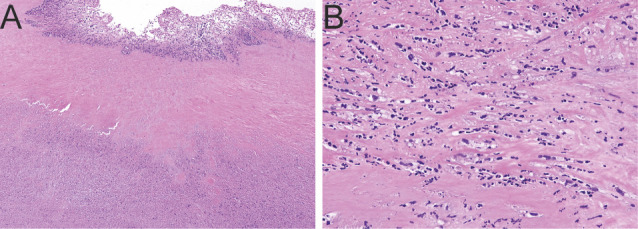 Fig 3
Fig 3| Ref. | Age/sex | Country | Medical history | Presenting symptoms | Exposure | Valve involved | Treatment | Complications | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| ( | 55/F | Romania | HTN, biliary dyskinesia | Fever, headache, confusion, obtundation | Unknown | Aortic | Penicillin G x 4 wk, gentamicin x 2 wk | Ischemic stroke | Survival |
| ( | 70/F | Spain | None | Fever, gastrointestinal symptoms | Unpasteurized cheese | nd | Beta-lactam | Pneumonia | Survival |
| ( | 82/M | Denmark | T2DM, IHD, AFib, gout, prostate cancer | Dyspnea, hemoptysis, fever, severe left shoulder pain, LE edema | Horses | Aortic | Benzylpenicillin + gentamicin, followed by amoxicillin + rifampin, total 87 d | Left shoulder osteitis | Survival |
| ( | 79/M | South Africa | None | Left wrist and right knee pain/swelling, fever, headache, lethargy | Horse manure | Aortic | Benzylpenicillin x 6 wk | Left wrist and Right knee septic arthritis | Survival |
| ( | 65/M | United States | None | Fevers, bilateral ankle/knee pain and edema | Veterinary occupation | Mitral | Penicillin G followed by ceftriaxone, 8 wk | Polyarthritis, L5-S1 discitis/OM with epidural phlegmon | Survival |
| ( | 57/M | Finland | Bicuspid AV, AI | Fever, obtundation | Horses (horse breeder) | Aortic | IV penicillin x 5 wk, gentamicin x 10 d | Meningitis | Survival |
| ( | 59/M | Quebec, CA | HTN, T2DM, HLD, CAD, CKD, ASD | Generalized weakness, lightheadedness, dyspnea, cough, fever | Horses | Mitral | Ceftriaxone + rifampin, 6 wk | Bilateral endophthalmitis, blindness, meningitis | Survival |
| ( | 69/M | Colombia | None | Polyarthralgia, followed by right hemiparesis, obtundation | Unpasteurized milk | Mitral | Penicillin G | Hemiparesis | Deceased |
- —Houston Methodist Academic Institute
- —Fondren Foundationhttp://dx.doi.org/10.13039/100015158
- —NIH Loan Repayment Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Infective Endocarditis Diagnosis and Management · Antimicrobial Resistance in Staphylococcus
INTRODUCTION
Streptococci once caused the majority of infective endocarditis (IE) cases. However, with the recent rise of Staphylococcus aureus endocarditis, streptococci now comprise 20%–30% of cases (1). The majority of streptococcal endocarditis cases are caused by viridans group streptococci, followed by Lancefield group D streptococci (S. bovis/gallolyticus) (2). Lancefield groups A, B, C, and G beta-hemolytic streptococci are uncommon causes of endocarditis (2). Group C and group G streptococci (GCGS) are closely related genetically, and the taxonomy of these organisms has been in flux over time (3), complicated by the lack of consistency in obtaining accurate species-level identification until recent advancements in matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF) (4). The GCGS S. dysgalactiae subsp. equisimilis and subsp. dysgalactiae are commensal organisms of the human oropharynx, skin, and female genitourinary tract, and they cause the majority of human GCGS infections (5). Streptococcus equi subspecies zooepidemicus (SESZ) and subspecies equi (SESE) are zoonotic GCGS; SESZ are commensal organisms of horses but can also cause acute equine infections (6). Human infections with SESZ can be acquired from contact with infected animals, primarily horses (6), and consumption of unpasteurized dairy products from animals with SESZ mastitis (7). We present a case of SESZ infective endocarditis in a patient with exposure to horses.
CASE PRESENTATION
A 58-year-old woman presented with progressively worsening fever, malaise, and chills for 4 weeks and severe arthralgias for 4 days. She developed anterior right shoulder pain 4 days prior to presentation and left wrist pain and hand swelling 2 days prior to presentation. She had no additional symptoms, no history of surgeries or trauma, and no family history of autoimmune conditions. She was taking olmesartan for hypertension and sumatriptan for migraines but was otherwise healthy. Upon inquiry of potential exposure history, she stated that she had regular interaction with horses as an owner and also interacted with llamas and alpacas regularly at a farm. None of the horses or other farm animals were noticeably ill. On examination, she was tachycardic with a heart rate of 101 bpm and febrile with a temperature of 101.1°F. She had a grade II systolic murmur heard best at the left lower sternal border, decreased abduction of her right shoulder, and nonpitting edema of her left wrist and dorsum of her hand. Despite the fever, she did not appear acutely ill. The remainder of her physical examination was normal. Complete blood count was remarkable for white blood cell count of 13,000 cells/µL (ref. range, 3,400–11,000 cells/µL) and thrombocytopenia of 65,000 platelets/μL (ref. range, 150,000–450,000 platelets/μL). A complete metabolic panel showed serum albumin of 2.9 g/dL (ref. range, 3.5–5.0 g/dL), alanine transaminase of 63 U/L (ref. range, 0–50 U/L), aspartate transferase of 80 U/L (ref. range, 0–35 U/L), and was otherwise normal. Urine dipstick was positive for bilirubin, trace ketones, and 2+ protein. No bacteria were grown from urine. A chest radiograph was normal. Magnetic resonance imaging (MRI) of the patient’s right shoulder and left wrist demonstrated nonspecific inflammation of the acromioclavicular joint and synovitis at the base of the left thumb joint. Two sets of blood cultures were drawn, and cefepime 2 g q8h and vancomycin 15 mg/kg q12h after a one-time 20 mg/kg loading dose were initiated for empiric treatment of sepsis. All four blood culture bottles grew group C streptococci after 20 h of incubation. Species identification by matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) in the clinical microbiology laboratory confirmed Streptococcus equi subspecies zooepidemicus (SESZ).
The genome of the SESZ strains recovered from the patient’s blood cultures was sequenced using an Illumina Nextera XT kit and NextSeq instrument as previously described (8). We retrieved 684 publicly available SESZ genomes, recovered from a variety of human and animal hosts worldwide, deposited in the NCBI Short Read Archive (https://www.ncbi.nlm.nih.gov/sra) and Microbial Genome Database (https://www.ncbi.nlm.nih.gov/genome/microbes). Phylogenetic analysis was performed to compare the patient’s SESZ isolates to the publicly available genomes.
Transesophageal echocardiogram (TEE) revealed several 1- to 2-cm vegetations on the atrial surface of the tricuspid valve with possible leaflet perforation (Fig. 1) and moderate tricuspid regurgitation. Antibiotic treatment was changed to ceftriaxone 2 g q24h and gentamicin 3 mg/kg q24h in accordance with the Infectious Diseases Society of America/American Heart Association guidelines for group C streptococcus endocarditis (9). Blood cultures were repeated 3 days after initial blood cultures were negative for growth. Cardiothoracic surgery consultants advised antibiotic treatment with follow-up at the end of therapy. Given the high suspicion for septic arthritis, joint aspiration of the left wrist triscaphe joint was performed, but the aspiration did not yield any fluid.
Tricuspid valve with 1–2 cm vegetation (yellow arrow) on the atrial surface.
Within 3–4 days of antibiotic therapy, the patient had rapid improvement in her joint pain and swelling. Despite this, daily fevers up to 103°F persisted, and a computed tomography (CT) scan of chest, abdomen, and pelvis demonstrated mild multifocal pulmonary opacities consistent with septic emboli (Fig. 2). Gentamicin was stopped after the patient developed a mild acute kidney injury during her admission, which subsequently resolved. She continued to feel well, had resolution of leukocytosis, thrombocytopenia, and acute kidney injury, became afebrile, and was discharged on hospital day 12 on combination therapy with intravenous ceftriaxone 2 g q24h and oral levofloxacin 750 mg daily to complete 6 weeks of antibiotics.
Computed tomography of the chest demonstrating multiple pulmonary opacities consistent with pulmonary septic emboli.
Upon follow-up in the Infectious Diseases clinic at the end of antibiotic treatment, the patient now had new symptoms of bilateral lower extremity swelling, shortness of breath, and subjective fever both during and after antibiotic treatment. Repeat TEE demonstrated failure of the lateral commissure of the tricuspid valve with associated worsened tricuspid regurgitation and new moderate mitral and aortic valve regurgitation. No abscess was apparent by TEE. The patient was hospitalized and found to have a left pleural effusion; 900 cc of exudative pleural fluid was removed with cultures yielding no growth. While hospitalized, she had recurrent daily fevers up to 102°F while remaining otherwise asymptomatic and without other abnormal vital signs. Blood cultures repeated on day 42 after the initial blood cultures remained negative. CT angiography of chest, abdomen, and pelvis, magnetic resonance imaging (MRI) of the brain with contrast, and a tagged white blood cell scan did not demonstrate evidence of disseminated infection. A cardiac MRI demonstrated new evidence of a flail mitral valve. Due to the patient’s worsening symptoms and valvular dysfunction, she underwent tricuspid valve and aortic valve replacement, mitral valve repair, and left atrial appendage clip. Tricuspid valve histopathology demonstrated marked necrosis with acute neutrophilic infiltrate (Fig. 3). She tolerated surgery well, was extubated on post-operative day 1, and was discharged home to complete a 4 week course of ceftriaxone 2 g q24h. Overall, she completed 10 weeks of antibiotics. She had complete resolution of symptoms of heart failure and fever and continues to do well more than a year after surgery.
Histopathologic examination of the tricuspid valve leaflet. Micrographs show prominent areas of myxoid degeneration and necrosis with acute inflammation. Original magnification (A) 2× and (B) 20×. Hematoxylin and eosin (H&E) stain.
DISCUSSION
Human infections with SESZ can be acquired from consumption of unpasteurized dairy products from animals with SESZ mastitis (7), as well as contact with infected animals, primarily horses (6), and pertinently to our patient, alpacas and llamas (10), although direct animal-to-human transmission has not been documented. Our patient denied any obvious illness in animals that she encountered.
In the literature, human SESZ infections are predominantly reported in Europe, Asia, or Canada, with a variety of clinical presentations (6). Review of the modern epidemiology of SESZ native valve endocarditis identified eight cases published since 2000 (Table 1). Including our patient, the median age of patients with SESZ endocarditis is 65 years old. Two patients had exposure to unpasteurized cheese, four patients had exposure to horses, and one patient was a retired veterinarian. Four patients had an initial presentation with polyarthritis, with two patients with culture-proven SESZ septic arthritis. All prior reported cases had involvement of either the aortic or mitral valve (7, 11–17). To our knowledge, our patient is the first reported case of right-sided SESZ endocarditis. Our patient was previously healthy, with a past medical history of well-controlled hypertension and migraines. She had no previous cardiac history and was fit and active prior to illness. She did not have typical risk factors for right-sided endocarditis, including intravenous drug use, implantable cardiac device, or cardiac abnormalities.
Of the publicly available SESZ genomes, the patient’s isolates were genetically most similar to strains recovered during a post-streptococcal glomerulonephritis outbreak epidemiologically linked to consumption of unpasteurized cheese (18). Our patient denied consumption of unpasteurized dairy products. Although her initial hospital course was complicated by mild acute kidney injury, this was temporally related to the initiation of gentamicin therapy, and renal abnormalities resolved after discontinuation of the antibiotic. She did not have any other episodes of impaired renal function or clinically apparent glomerulonephritis throughout her follow-up.
Our patient notably had persistent fever during her initial hospitalization and subsequent outpatient treatment and through her second hospitalization up until surgery. Persistent fever in patients with infective endocarditis (IE) is worrisome for unidentified disseminated sites of infection, cardiac complications such as cardiac abscess, new infections including nosocomial, and drug fever (19). However, none of these etiologies could be identified in our patient. We hypothesize that her persistent fever is related to the ongoing inflammation and necrosis of the large valvular vegetation, as described in other reports of IE (20). This possibility is particularly supported by her complete defervescence after surgery.
SESZ is closely related to group A Streptococcus (GAS, S. pyogenes) (18). While the molecular pathogenesis of GAS has been well studied, little is known about GCGS. A recent study of GCGS S. dysgalactiae subsp. equisimilis (SDSE) strains reported that compared to other SDSE emm-types, stG62647 strains were associated with significantly increased virulence in a mouse model of invasive infection (8). The molecular basis for the difference in virulence among SDSE strains is under investigation. The potential role of virulence factors shared among GAS and GCCS, such as secreted toxins, proteases, antiphagocytic proteins, and others, is unstudied in SESZ human disease.
In conclusion, Streptococcus equi subsp. zooepidemicus is a zoonotic pathogen with prominent risk factors of exposure to horses and other domestic animals and consumption of unpasteurized dairy products. Human infection with SESZ can be invasive and severe, and endocarditis is an uncommon but possible manifestation. Clinicians should have a high index of suspicion for zoonotic infections, such as those caused by SESZ in patients with significant exposure to animals. Further study is needed to understand the molecular pathogenesis of SESZ, which may reveal which patients are likely to have severe disease courses or suffer post-streptococcal immunological phenomena.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fowler V, Miro JM, Hoen B, et al.. 2005. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA 293:3012–3021. doi:10.1001/jama.293.24.301215972563 · doi ↗ · pubmed ↗
- 2Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG Jr, Bayer AS, Karchmer AW, Olaison L, Pappas PA, Moreillon P, Chambers ST, Chu VH, Falcó V, Holland DJ, Jones P, Klein JL, Raymond NJ, Read KM, Tripodi MF, Utili R, Wang A, Woods CW, Cabell CH, International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) Investigators. 2009. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohor · doi ↗ · pubmed ↗
- 3Facklam R. 2002. What happened to the Streptococci: overview of taxonomic and nomenclature changes. Clin Microbiol Rev 15:613–630. doi:10.1128/CMR.15.4.613-630.200212364372 PMC 126867 · doi ↗ · pubmed ↗
- 4Daubié AS, Defrance C, Renvoisé A, Barreda E, D’Alessandro C, Brossier F, Jarlier V, Aubry A. 2014. Illustration of the difficulty of identifying Streptococcus equi strains at the subspecies level through a case of endocarditis in an immunocompetent man. J Clin Microbiol 52:688–691. doi:10.1128/JCM.01447-1324478515 PMC 3911343 · doi ↗ · pubmed ↗
- 5Jensen A, Kilian M. 2012. Delineation of Streptococcus dysgalactiae, its subspecies, and its clinical and phylogenetic relationship to Streptococcus pyogenes. J Clin Microbiol 50:113–126. doi:10.1128/JCM.05900-1122075580 PMC 3256718 · doi ↗ · pubmed ↗
- 6Timoney JF. 2004. The pathogenic equine streptococci. Vet Res 35:397–409. doi:10.1051/vetres:200402515236673 · doi ↗ · pubmed ↗
- 7Bordes-Benítez A, Sánchez-Oñoro M, Suárez-Bordón P, García-Rojas AJ, Saéz-Nieto JA, González-García A, Álamo-Antúnez I, Sánchez-Maroto A, Bolaños-Rivero M. 2006. Outbreak of Streptococcus equi subsp. zooepidemicus infections on the island of Gran Canaria associated with the consumption of inadequately pasteurized cheese. Eur J Clin Microbiol Infect Dis 25:242–246. doi:10.1007/s 10096-006-0119-x 16550347 · doi ↗ · pubmed ↗
- 8Beres SB, Olsen RJ, Long SW, Eraso JM, Boukthir S, Faili A, Kayal S, Musser JM. 2023. Analysis of the genomics and mouse virulence of an emergent clone of Streptococcus dysgalactiae Subspecies equisimilis Microbiol Spectr 11:e 0455022. doi:10.1128/spectrum.04550-2236971562 PMC 10100674 · doi ↗ · pubmed ↗