Flying under the radar: vancomycin heteroresistance in Staphylococcus epidermidis peritonitis is associated with treatment failure
Malgorzata K. Kopczyk, Joshua P. Ramsay, Kieran T. Mulroney, Emily Salisbury, Wai Shaun Ho, Christine F. Carson, Elena Colombi, Teagan Paton, Aron Chakera

TL;DR
A patient with peritoneal dialysis peritonitis caused by Staphylococcus epidermidis failed vancomycin treatment due to undetected heteroresistance, highlighting diagnostic limitations.
Contribution
Demonstrates vancomycin heteroresistance in S. epidermidis peritonitis undetected by standard AST and whole-genome sequencing.
Findings
Vancomycin heteroresistance in S. epidermidis was undetected by VITEK 2 and broth-microdilution AST.
Population analysis profiling confirmed heteroresistance despite conventional susceptibility results.
Whole-genome sequencing failed to identify genetic mechanisms behind the heteroresistance.
Abstract
Antimicrobial resistance (AMR) is a global One Health problem and a growing threat to human and animal health. Antimicrobial susceptibility tests (AST) such as the broth-microdilution method (BMD) guide appropriate antimicrobial therapy but may fail to detect various forms of AMR, such as heteroresistance. We report vancomycin treatment failure in a Staphylococcus epidermidis peritoneal dialysis (PD) associated peritonitis case with vancomycin heteroresistance undetected by conventional AST and whole-genome sequencing. A patient with cloudy PD effluent presented to his local dialysis center. Samples were sent for testing, and empirical treatment with vancomycin and gentamicin was initiated. An S. epidermidis isolate (C099) was cultured, and treatment was changed to vancomycin monotherapy, with the isolate recorded as susceptible using the VITEK 2. Despite treatment, effluent remained…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
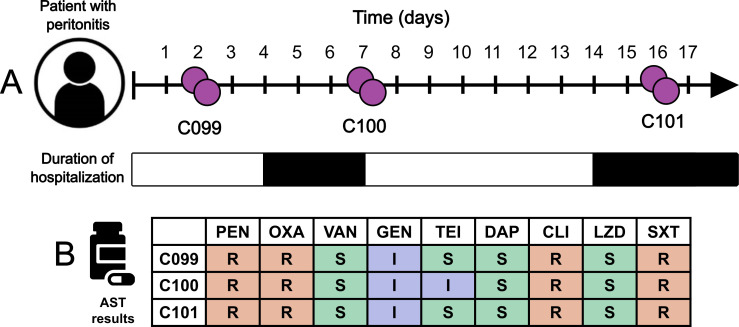 Fig 1
Fig 1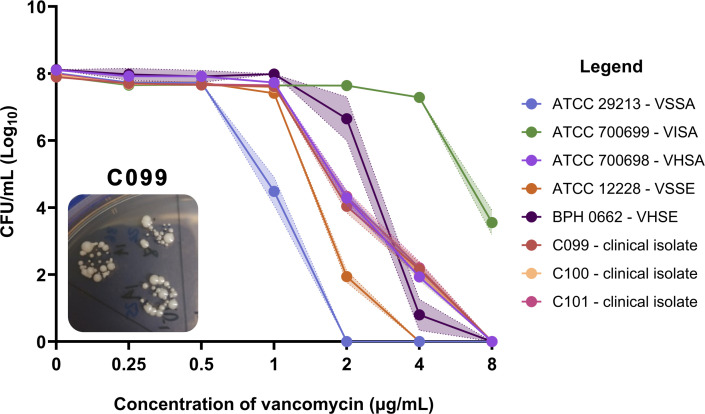 Fig 2
Fig 2| Isolate ID | PEN | OXA | GEN | CIP | CLI | LZD | DAP | TEI | VAN | TET | RIF | SXT |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C099 | ≥0.5 ( | ≥4 ( | 8 ( | 4 ( | ≥8 ( | 1 ( | 1 ( | 8 ( | 2 ( | 2 ( | ≤0.5 ( | 160 ( |
| C100 | ≥0.5 ( | ≥4 ( | 4 ( | ≥8 ( | ≥8 ( | 1 ( | 0.5 ( | 16 ( | 2 ( | 2 ( | ≤0.5 ( | 160 ( |
| C101 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Isolate ID | P/T | PEN | OXA | FOX | VAN | TEI | GEN | SXT | DAP | CLI | AMO | LZD | AXO |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C099 | 2 ( | ≥1 ( | 2 ( | 8 ( | 2 ( | 4 ( | 8 ( | 8 ( | 0.5 ( | ≥2 ( | 2 ( | ≤0.5 ( | 8 ( |
| C100 | 1 ( | ≥1 ( | 2 ( | 8 ( | 2 ( | 4 ( | 8 ( | 8 ( | 0.5 ( | ≥2 ( | 2 ( | ≤0.5 ( | 8 ( |
| C101 | 2 ( | ≥1 ( | 2 ( | 8 ( | 2 ( | 4 ( | 8 ( | 8 ( | 0.5 ( | ≥2 ( | 2 ( | ≤0.5 ( | 8 ( |
| Isolate ID | Genome characteristics | Genetic resistance markers | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Size (bp) | CDS |
|
|
|
|
| |||
| C099 | 2,490,698 | 2,257 | + | + | + | + | + | + | + |
| C100 | 2,489,174 | 2,267 | + | + | + | + | + | + | + |
| C101 | 2,489,413 | 2,260 | + | + | + | + | + | + | + |
| Gene | Mutation | Present in isolates? |
|---|---|---|
|
| H481Y ( | No |
| D471E ( | No | |
| I527M ( | No | |
| A621E ( | No | |
| N651I ( | No | |
| P940S ( | No | |
|
| G223D ( | No—S223 |
| I237T ( | No—D237 | |
| I306F ( | No | |
| R286 ( | No | |
|
| N197 ( | No |
|
| T136I ( | No |
|
| 144 bp deletion ( | No |
| Isolate number | Local ID | Accession |
|---|---|---|
| C099 | C099 chromosome |
|
| pC99MK1 |
| |
| pC99MK2 |
| |
| pC99MK3 |
| |
| pC99MK4 |
| |
| pC99MK5 |
| |
| C100 | C100 chromosome |
|
| pC100MK1 |
| |
| pC100MK2 |
| |
| pC100MK3 |
| |
| pC100MK4 |
| |
| pC100MK5 |
| |
| pC100MK6 |
| |
| C101 | C101 chromosome |
|
| pC101MK1 |
| |
| pC101MK2 |
| |
| pC101MK3 |
| |
| pC101MK4 |
| |
| pC101MK5 |
| |
| pC101MK6 |
|
- —National Health and Medical Research Councilhttp://dx.doi.org/10.13039/501100000925
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Bacterial Identification and Susceptibility Testing · Clostridium difficile and Clostridium perfringens research
INTRODUCTION
Peritonitis is a serious complication of peritoneal dialysis (PD) and remains associated with morbidity, treatment failure, and mortality (1). PD-associated peritonitis is most commonly caused by gram-positive bacteria (2, 3), with coagulase-negative staphylococci (CoNS) such as Staphylococcus epidermidis contributing to approximately half of the cases (4, 5). Compared to peritonitis caused by other micro-organisms, CoNS peritonitis has the highest rates of relapse, recurrence, and catheter removal (6, 7), which can lead to prolonged hospitalizations, further increasing the healthcare cost burden.
The International Society for Peritoneal Dialysis (ISPD) recommends the prompt use of empirical antimicrobial therapy to cover both gram-positive and gram-negative bacteria in peritonitis cases (8). In our unit, vancomycin and gentamicin are administered intraperitoneally (IP) (9) with further treatment guided by the results of culture and antimicrobial susceptibility test (AST) results. While the broth-microdilution method (BMD) is the gold-standard AST, clinical laboratories utilize automated phenotypic testing methods (such as the VITEK 2) to reduce time to result and increase throughput (10).
Antimicrobial resistance (AMR) is a serious threat to peritonitis patients, limiting effective treatment options and associated with higher treatment failure and relapse rates (11). Heteroresistance is a form of AMR where a small subset of a bacterial population exhibits increased resistance to antimicrobial agents (12, 13). It has been documented in a variety of bacterial species including CoNS (14) but can be undetected by conventional AST methods (15, 16). This can lead to the misclassification of the AMR profile of the organism, resulting in ineffective antimicrobial therapy (12).
We report heteroresistance in a multi-drug-resistant (MDR) S. epidermidis isolated from a PD peritonitis case. The infection did not resolve, resulting in eventual vancomycin treatment failure. Despite phenotypic AST repeatedly confirming the sensitivity of the S. epidermidis isolates to vancomycin, drained PD effluent remained culture positive. Using multiple phenotypic methods and whole-genome sequencing (WGS), we characterized the three S. epidermidis isolates isolated sequentially (days 2, 7, and 16) during the peritonitis episode and confirmed the presence of heteroresistance as a potential explanation for the failure to resolve infection.
CASE PRESENTATION
In 2017, a 63-year-old male presented to a community peritoneal dialysis center for review of cloudy dialysis effluent (Fig. 1A). Dialysate samples were sent to the clinical laboratory for testing, and empirical treatment commenced with 200 mg of gentamicin and 2 g of vancomycin administered IP (following the statewide peritonitis treatment protocol with a minimum dwell time of 6 hours). Four days later, he presented to the hospital with persistent cloudy effluent and new abdominal pain. S. epidermidis was isolated from the samples (ID: C099), and treatment was changed to vancomycin monotherapy with the isolate recorded as susceptible using the VITEK 2 (Fig. 1B; Table 1). On admission, serum vancomycin levels demonstrated that he was within a therapeutic range at 17 mg/L (target >15 mg/L). On his third day of admission, he was improving clinically with no ongoing abdominal pain. A repeat sample was sent with results demonstrating an improvement in white cell count from 5.4 × 10^10^ /L (100% neutrophils) in the initial sample to 1.8 × 10^10^ /L (74% neutrophils). He was discharged with a plan to continue IP vancomycin for 21 days.
Isolation of MDR S. epidermidis isolates from a peritonitis case. (A) Timeline of case presentation. Bacterial isolates are shown in purple, and the duration of hospitalization is shaded in black. (B) Clinical AST results using the VITEK 2 system. Benzylpenicillin, PEN; oxacillin, OXA; vancomycin, VAN; gentamicin, GEN; ciprofloxacin, CIP; clindamycin, CLI; linezolid, LZD; trimethoprim/sulfamethoxazole, SXT. Results shown as resistant (red), susceptible (green), or intermediate (blue) inferred from breakpoints in CLSI M100 27th ed (17). All three clinical isolates tested were susceptible to vancomycin.
On day 7, S. epidermidis was again cultured from the effluent samples (ID: C100). On day 14 (after initial presentation), the patient presented to the hospital again with abdominal pain and fluid overload. Serum vancomycin levels remained within the therapeutic range, and repeat microscopy continued to show an improvement in white cell counts: 2.5 × 10^9^ /L (70% neutrophils). Dialysate samples (day 16), however, remained culture positive for S. epidermidis (ID: C101). All isolates (C099, C100, and C101) were susceptible to vancomycin according to the VITEK 2 (Fig. 1B; Table 1). As the patient could no longer adequately dialyze, the Tenckhoff catheter was removed (17 days after his initial presentation), and the patient was transferred to hemodialysis.
To investigate the potential causes for failure to resolve infection, we performed additional AST using the BMD method with Sensititre custom plates (Thermo Fisher, United States), with results shown in Table 2. The clinical isolates were susceptible to vancomycin (MIC = 2 µg/mL) and other antimicrobials, including cefoxitin (MIC = 8 µg/mL), teicoplanin (MIC = 4 µg/mL), daptomycin (MIC = 0.5 µg/mL), and linezolid (MIC ≤0.5 µg/mL). Isolates were resistant to benzylpenicillin (MIC = ≥1 µg/mL), oxacillin (MIC = 2 µg/mL), trimethoprim/sulfamethoxazole (MIC = 8 µg/mL), and clindamycin (MIC ≥2 µg/mL). VITEK 2 MIC results were not recorded for C101; however, our BMD MIC results for vancomycin and other antimicrobials tested were concordant or within essential agreement (EA) with the clinical laboratory results, with the exception of MIC results for teicoplanin for C100 (discrepancy just outside of EA). Isolates were defined as MDR as they were resistant to multiple antimicrobials from more than three antimicrobial classes (18).
Heteroresistance is detected using the “gold-standard” population analysis profiling area under the curve (PAP-AUC) method (12) with test isolates compared to ATCC 700698, a reference control Staphylococcus aureus with documented heterogeneous resistance to vancomycin (19). Heteroresistance was confirmed if the area under the curve (AUC) of the test isolate divided by ATCC 700698 was ≥0.90 (20). While previous studies have applied this method directly to CoNS isolates (21), we included two S. epidermidis controls: ATCC 12228 (vancomycin susceptible) and BPH0662 (vancomycin heteroresistant) to further investigate the applicability of the diagnostic criteria to S. epidermidis. AUC ratios of 0.60 and 1.02 were obtained, respectively, for the controls, confirming classification validity, and all three clinical isolates were confirmed as heteroresistant to vancomycin (Fig. 2), with AUC ratios of 1.00, 1.00, and 1.03 for C099, C100, and C101 recorded. The sequential isolates C099, C100, and C101 also displayed small colony variant phenotypes growing on brain heart infusion (BHI) agar plates containing vancomycin (Fig. 2) and on blood agar plates.
Confirmation of heteroresistance using the PAP-AUC method. Shaded bars indicate SEM. VSSA, vancomycin susceptible S. aureus (blue); VISA, vancomycin intermediate S. aureus (15); VHSA, vancomycin heteroresistant S. aureus (purple); VSSE, vancomycin susceptible S. epidermidis (orange); VHSE, vancomycin heteroresistant S. epidermidis (dark purple); C099 (red); C100 (cream); and C101 (pink). Image of C099 growing on 2 µg/mL of vancomycin (10−1 dilution). Heterogeneous colony phenotypes (small colony variants) were seen in all three clinical isolates growing in 2 and 4 µg/mL of vancomycin.
In addition to phenotypic characterisation, WGS was also performed using both Illumina NextSeq (Illumina, United States) and MinION (Oxford Nanopore Technologies, United Kingdom) to investigate the genetic basis for the heteroresistance. All three isolates were nearly genetically identical (OrthoANIu percentages of 99.99% with over 99% genome coverage) (22). The resistome of each isolate was identified using Resfinder 4.1 (23), ABRicate (Galaxy Version 1.0.1 using the public server at usegalaxy.org.au) (24), and Comprehensive Antibiotic Resistance Database (CARD) (25). Each isolate harbored multiple chromosomal and plasmid-encoded resistance genes (Table 3) but did not harbor van genes associated with vancomycin resistance (26). The three isolates were screened for mutations in genes previously associated with vancomycin heteroresistance (Table 4). We were unable to detect any single-nucleotide polymorphisms in candidate genes associated with vancomycin heteroresistance, such as dual D471E/I527M mutations in the rpoB gene, the mechanism for heteroresistance in BPH0662 (27).
DISCUSSION
We document a case of vancomycin treatment failure in a patient with MDR S. epidermidis peritonitis where conventional AST failed to identify isolates as being resistant, and we subsequently confirmed heteroresistance. Heteroresistance was only detected using the “gold-standard” PAP-AUC method (12), and a genetic basis of the mechanism driving this phenotype was not identified. Heteroresistance is an established phenomenon, occurring in different bacterial species (12, 36), and heterogeneity to vancomycin has been observed in two S. epidermidis peritonitis cases (37, 38), though not confirmed using the PAP-AUC method. The presence of small colony variants, as documented in our study, has also been associated with the development of heteroresistance in Escherichia coli (39) and implicated in chronic and recurrent staphylococcal infections (40).
The choice of antimicrobial treatment for peritonitis relies on results from ASTs; however, there are many limitations to existing tests. While the BMD remains the gold-standard method for susceptibility testing (41), there are detection limitations inherent in BMD assays, as heteroresistant bacteria often have a slower growth rate (42). For staphylococci in particular, heteroresistant subpopulations may also only occur at a frequency of 1 in 10^6^ CFU/mL (43). The limitations of ASTs to detect heteroresistance have also been recently highlighted for the novel antibiotic cefiderocol in cases of carbapenem-resistant Acinetobacter baumannii in multiple studies (41, 44). While advances have been made in WGS, the genetic mechanisms of heteroresistance are complex and remain largely cryptic, especially for CoNS (14). To further understand these mechanisms, future studies need to expand the number of complete genomic databases for CoNS, as heteroresistance has been characterized in S. aureus to a greater extent. Limitations of this study stem from the nature of conventional antimicrobial susceptibility testing. As these tests measure antimicrobial activity in vitro, we cannot fully evaluate the effects of the host environment on infection clearance or the pharmacokinetics of the antimicrobial agents (45). In addition, the catheter from the patient was not available to assess for evidence of colonization or biofilm formation. Biofilm formation has been implicated in increased bacterial resistance (21, 46, 47) and has also been associated with treatment failure (48, 49). While biofilm formation and effective source control are important contributing factors to treatment failure, clinicians also need to be aware of heteroresistance and its implications on patient outcomes.
In conclusion, vancomycin heteroresistance was not detected by conventional AST methods, with the patient failing to clear the infection. Our investigation did not find mutations in genes previously associated with heteroresistance in CoNS isolates C099, C100, and C101; however, the phenotypic PAP-AUC results unequivocally indicated heteroresistance. In the treatment of intractable or non-resolving peritonitis, it is important to recognize the limitations of conventional AST methods and the potential role of heteroresistance, so that therapy can be tailored to prevent adverse outcomes. Our results highlight the need for standardized, rapid screening assays that could be utilized at clinical laboratories to detect heteroresistance and help guide appropriate antimicrobial therapy, ultimately improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salzer WL. 2018. Peritoneal dialysis-related peritonitis: challenges and solutions. Int J Nephrol Renovasc Dis 11:173–186. doi:10.2147/IJNRD.S 12361829928142 PMC 6001843 · doi ↗ · pubmed ↗
- 2Musoke J, Bisiwe F, Natverlal A, Moola I, Moola Y, Kajee U, Parlato A, Bailey A, Arendse J. 2020. The prevalence and bacterial distribution of peritonitis amongst adults undergoing continuous ambulatory peritoneal dialysis at Universitas hospital. S Afr J Infect Dis 35:104. doi:10.4102/sajid.v 35i 1.10434485466 PMC 8378107 · doi ↗ · pubmed ↗
- 3Santoianni JE, Predari SC, Verón D, Zucchini A, de Paulis AN. 2008. A 15 year-review of peritoneal dialysis-related peritonitis: microbiological trends and patterns of infection in a teaching hospital in Argentina. Rev Argent Microbiol 40:17–23.18669048 · pubmed ↗
- 4Kofteridis DP, Valachis A, Perakis K, Maraki S, Daphnis E, Samonis G. 2010. Peritoneal dialysis-associated peritonitis: clinical features and predictors of outcome. Int J Infect Dis 14:e 489–e 493. doi:10.1016/j.ijid.2009.07.01619926324 · doi ↗ · pubmed ↗
- 5Kitterer D, Latus J, Pöhlmann C, Alscher MD, Kimmel M. 2015. Microbiological surveillance of peritoneal dialysis associated peritonitis: antimicrobial susceptibility profiles of a referral center in GERMANY over 32 years. P Lo S One 10:e 0135969. doi:10.1371/journal.pone.013596926405797 PMC 4583423 · doi ↗ · pubmed ↗
- 6Lau SY, Bee BC, Wong HS, Omar MS, Bahari N. 2022. Predictive factors, treatment, and outcomes of coagulase-negative staphylococcal peritonitis in Malaysian peritoneal dialysis patients: a single-center study. Int J Nephrol 2022:8985178. doi:10.1155/2022/898517835449558 PMC 9017555 · doi ↗ · pubmed ↗
- 7Nessim SJ, Nisenbaum R, Bargman JM, Jassal SV. 2012. Microbiology of peritonitis in peritoneal dialysis patients with multiple episodes. Perit Dial Int 32:316–321. doi:10.3747/pdi.2011.0005822215659 PMC 3525437 · doi ↗ · pubmed ↗
- 8Li PK-T, Chow KM, Cho Y, Fan S, Figueiredo AE, Harris T, Kanjanabuch T, Kim Y-L, Madero M, Malyszko J, Mehrotra R, Okpechi IG, Perl J, Piraino B, Runnegar N, Teitelbaum I, Wong JK-W, Yu X, Johnson DW. 2022. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Perit Dial Int 42:110–153. doi:10.1177/0896860822108058635264029 · doi ↗ · pubmed ↗