Lithium Augmentation in Treatment‐Resistant Depression: A Qualitative Review of the Literature
Angela Acero‐González, Yahira Guzman, Nadia Juliana Proaños, Rosa‐Helena Bustos, María Aconcha, Ivan Guerrero, Laura Alejandra Martinez, Michael Berk, Seetal Dodd

TL;DR
This paper reviews how lithium can help treat depression that doesn't respond to standard medications, focusing on its benefits and safety.
Contribution
The paper provides a qualitative review of lithium's role as an augmentation therapy for treatment-resistant depression.
Findings
Lithium is a cost-effective and effective augmentation therapy for treatment-resistant depression.
Lithium reduces mortality risk by lowering aggression and suicide rates in patients with TRD.
Lithium requires careful monitoring due to its narrow therapeutic range and potential toxicity.
Abstract
Depression is the leading cause of disability worldwide, affecting people of all ages. Both pharmacological and non‐pharmacological therapies are available for its treatment. However, some patients do not respond to first‐line pharmacological interventions, referred to as treatment‐resistant depression (TRD). Individuals with TRD face a significantly higher risk of mortality, including an increased risk of suicide. Additionally, TRD poses a substantial economic burden on health care systems. Various treatment options have been explored for TRD, including augmentation of an antidepressant through the use of an additional agent. Lithium salts have shown promising benefits in the TRD. Lithium requires close therapeutic monitoring due to its narrow therapeutic range, with well‐defined thresholds for efficacy and toxicity, in addition to its pharmacokinetic characteristics. Furthermore,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
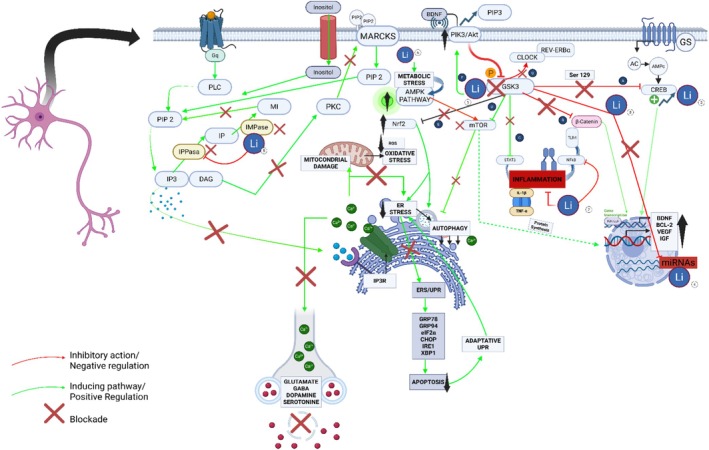 FIGURE 1
FIGURE 1| Structure | |
| Chemical formula | Li2O3 |
| Synonyms | Lithonate, Lithium carbonate, Lithi carbonas, Dilithium carbonate |
| Chemical structure | Composed of two lithium cations (Li+) and one carbonate anion (CO3 2−). The carbonate ion consists of one carbon atom covalently bonded to three oxygen atoms, with a trigonal planar geometry |
| Appearance | White, odorless crystalline powder |
| Molecular weight (amu) | 73.89 |
| Melting point | 723°C (1333°F) |
| Boiling point | Decomposes before boiling; forms lithium oxide (Li2O) and carbon dioxide (CO2) at high temperatures |
| Solubility in water | Slightly soluble; 13.3 g/L at 20°C, decreasing with increasing temperature. Solubility is pH‐dependent due to the carbonate ion's basicity |
| pH in Aqueous solution | Approximately 11–12 (basic due to hydrolysis of the carbonate ion). The basic pH of lithium carbonate solutions results from the partial hydrolysis of the carbonate ion (CO3 2− + H2O ⇌ HCO3 − + OH−) |
| PK parameter | Lithium |
|---|---|
|
| 0.5–1.2 mmol/L dose dependent |
|
| 1–3 h (immediate release) |
|
| |
| Protein binding, % | Lithium crosses cell membranes slowly and does not bind significantly to plasma proteins. < 10% (Low plasma protein binding) |
| Vd/F, L/kg, range | Approximately 0.7–1.0 L/kg |
| Metabolism | N/A. Lithium does not suffer any significant liver metabolic transformation. Lithium is excreted unchanged by the kidneys |
|
| |
|
|
18–36 h (adults with an average renal function) 40–50 h (impaired renal function) |
| CL, %, urine vs. feces | 95% urine, less than 5% by feces |
| Steady‐state concentration | Steady‐state plasma concentrations are typically achieved within 4–7 days of consistent dosing. Therapeutic plasma concentrations for bipolar disorder are generally maintained between 0.6–1.2 mEq/L for acute mania and 0.4–1.0 mEq/L for maintenance therapy, monitored via trough levels (12 h post‐dose) |
| Factors affecting pharmacokinetics |
|
| Lithium Pharmacokinetics and therapeutic drug monitoring |
Continuous monitoring of serum lithium levels is essential due to its narrow therapeutic range (toxic levels > 1.5 mEq/L) Renal function (e.g., serum creatinine, estimated glomerular filtration rate), thyroid function, and electrolyte balance should also be assessed every 3 months to mitigate long‐term adverse effects |
| Year and author | Type of article | Monotherapy | Combination | Neuromodulation (mECT) | Adverse reactions | Duration | Lithium dosage (augmentation therapy) | Lithium blood concentration | Diagnosis | Clinical outcome | References |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Catalano et al. (2020) | Review of literature | NA | Lithium + SSRIs/TCAs | NA | NA | NA | 600 mg/daily | NA | TRD | Lithium has both, a low unit cost and low NNT to TRD response (5) compared to aripiprazole, lithium, quetiapine, liothyronine, buspirone, brexipiprazole | [ |
| Costi et al. (2019) | Double‐blind randomized controlled trial | NA | Lithium + Ketamine | NA | Nausea, headache, dry mouth, abdominal pain, constipation, pollakiuria | 42 days | 600–1200 mg/daily, 0.5 mg/kg infuse IV over 40 min | 0.6–0.9 mEq/L | TRD | Participants randomized to lithium failed to show a prolonged reduction in MADRS score compared to those randomized to placebo | [ |
| Osterland et al. (2023) | Multicenter Prospective Cohort Study | NA | Lithium + baseline treatment | NA | Dizziness, tremor, nausea | 6 weeks | NS | 0.5–0.9 mmol/L (≥ 65 year) 0.4–0.8 mmol/L (< 65 year) | Unipolar Depression | Both groups (≥ 65 year and < 65 year patients) showed a significant decline of eGFR under lithium augmentation | [ |
| Bauer et al. (2003) | Systematic Review | NA | Lithium + TCA and tetracyclines | NA | NS | 12–14 days | 900–1200 mg/daily | NA | Bipolar disorder | Patients who respond to lithium augmentation should be maintained on lithium for a minimum of 12 months, or even longer. Lithium augmentation significantly increased prolactin response, compared with placebo pretreatment and antidepressant treatment alone | [ |
| NA | 2 days | 900 mg/daily | Bipolar disorder | ||||||||
| Lithium + various TCA | NA | 2 days | 900 mg/daily | Unipolar disorder | |||||||
| NA | 14 days | 900–1200 mg/daily | Unipolar disorder | ||||||||
| NA | 1–21 days | 250 mg/daily | Unipolar disorder | ||||||||
| 22–42 | 250 mg daily vs. 750 mg/daily | ||||||||||
| Lithium + various TCA and MAOI | NA | 14 days | 300–900 mg/daily | Unipolar disorder | |||||||
| Litium + various AD | NA | 14 days | 600–800 mg/daily |
Bipolar disorder Unipolar disorder | |||||||
| Litium + SSRI and TCA | NA | 42 days | 400–800 mg/daily | Not reported | |||||||
| Litium + SSRI | NA | 14 days | 800 mg/daily |
Bipolar disorder Unipolar disorder | |||||||
| Woon et al. (2017) | Review | This review focuses on the use of lithium as monotherapy. | NA | NA | Hypothyroidism, hyperparathyroidism, and weight gain | NS | 0.5–1.2 mmol/L | 0.5–1.2 mmol/L (Therapeutic range) | Bipolar disorder | Neuroprotection, reduction in manic and depressive episodes, mood stabilization | [ |
| Bauer et al. (2014) | Narrative Review | NA | Lithium used as augmentation therapy with antidepressants | NA | Polyuria, weight gain, tremor, nausea, hypothyroidism, renal effects | Variable (studies reviewed; suggested at least 1 year for maintenance) | Ranges from 300 mg/day to 1500 mg/day | 0.5–0.8 mmol/L (recommended for augmentation) |
Major Depressive Disorder (MDD) Treatment‐Resistant Depression Bipolar Disorder | Improved response and remission rates, significant efficacy in augmentation therapy | [ |
| Rybakowski et al. (2020) | Narrative review | NA | NA | NA | Interstitial nephropaty, hypothyroidism | NA | Should not exceed 500 mg | 0.6–0.8 mmol/L | Hypomania | Lower number of episodes, significantly reduced risk of rehospitalization, reduce suicide risk | [ |
| 0.8–1.2 mmol/L | Mania | ||||||||||
| Lithium + MS | 0.6–0.8 mmol/L | Rapid cycling | |||||||||
| 0.6–0.8 mmol/L | Prophylactic (long‐term prevention recurrences) | ||||||||||
| Lithium + SSRIs/TCAs/SNRI | 0.6–0.8 mmol/L | Depression | |||||||||
| McKeown et al. (2022) | Qualitative | NA | Lithium ( | NA | Tremor, dry mouth, nausea | 52 weeks | NA | NA | TRD | Patient experiences of lithium and quetiapine augmentation ‘Initial concerns’, ‘Experience of side effects’, ‘Perception of treatment efficacy’ and ‘Positive perception of treatment monitoring’. More concerns with lithium, but less side effects | [ |
| Erci et al. (2023) | Narrative review | NA | Lithium + antidepressive agent | NA | tremor, GI, weight gain, hypothyroidism, hyperparathyroidism, nephrogenic diabetes insipidus, lithium nephropathy | NA | 600–900 mg/day | 0.5–0.8 mmol/L | TRD | Efficacy in prevention of relapses and recurrences of mood episodes and in TDR in patients who have responded to ECT. Reduced suicide risk | [ |
| Terao et al. (2024) | Systematic review and meta‐analysis | NA | Combination therapy (ketamine, esketamine, aripiprazole, lithium) | NA | Ketamine: more acceptable, fewer adverse events. Esketamine and aripiprazole: less tolerable than placebo. | 1 to 6 weeks depending on the study | Ketamine IV 0.5 mg/kg, Esketamine intranasal 28–84 mg, Aripiprazol variable, lithium variable | NS | Treatment‐resistant unipolar depression | IV ketamine more effective than esketamine and aripiprazole. Lithium not different from IV ketamine in efficacy, tolerability, and acceptance | [ |
| Edwards et al. (2013) | Systematic review and economic evaluation | NA | Fluoxetine + Olanzapine, Fluoxetine + Lithium (dose not specified) | NA | Olanzapine: increased discontinuation rate. Lithium: lowered discontinuation rate compared to SSRI alone. | 8 weeks of acute treatment and 10 months of maintenance | Fluoxetine + Olanzapine, Fluoxetine + Lithium (dose not specified) | NS | Treatment‐resistant unipolar depression | Olanzapine with SSRI showed superiority to SSRI alone. Lithium with SSRI showed positive trends but no significant differences | [ |
| Undurraga et al. (2019) | Systematic review | Yes | Monotherapy and combination therapy (lithium alone or with antidepressants) | NA | General adverse effects of lithium not specifically detailed. | From 2 weeks to more than 12 months, depending on the study | NS | 0.5–1.4 mEq/L in maintenance studies | Major unipolar depression, acute and long‐term treatment | Lithium effective in unipolar depression as an adjunct and for maintenance. Uncertain benefit in monotherapy | [ |
| Patel et al. (2020) | Observational Study | NA | Combination of Lithium + ECT | (ECT combined with lithium) compared to either treatment alone | Higher risk of delirium and cognitive impairment (11.7 times more likely) | Acute inpatient treatment during hospitalization | NS | NS | Treatment‐resistant major depressive disorder, bipolar disorder (depressive and manic) | Higher risk of delirium in MDD (7.8%) than in BD (3.4%). Caution with combination is advised | [ |
| Morlet et al. (2019) | Cross‐sectional Multicenter Study | NA | Monotherapy and combination with antidepressants | NA | Hypothyroidism, no increase in other medical comorbidities | Average of 12.5 years (SD = 11.6 years) in long‐term lithium users |
59.1%: 723.8 mg sustained‐release formulation 15.9% ~ 546.4 mg (immediate‐release formulation) 25%: 487.5 mg lithium as an adjunct (sustained‐release formulation) | NS | Bipolar disorder and treatment‐resistant major depressive disorder | Reduction in depressive symptoms, lower benzodiazepine use, no impact on cognitive function | [ |
| Bennabi et al. (2019) | Clinical Guidelines | NA |
1st Intention Lithium, Quetiapine 2nd Intention Aripiprazole, Tri‐iodothyronine, Lamotrigine | ECT in monotherapy or in combination | NS | At least 6 months after remission; longer duration for recurrent cases | NS | 0.5 to 0.8 mmol/L Measurement recommended | Treatment‐resistant depression | Recommendations for lithium treatment optimization, including plasma level monitoring | [ |
| Rybakowski (2021) | Narrative Review | Used for prophylaxis of affective episodes in bipolar disorders and recurrent depression | Used to enhance antidepressant efficacy in TRD | NS | Nephrotoxicity and thyroid alterations; risk of tolerance with prolonged use. | More than 5 years | 600–1800 mg daily (lithium carbonate) | 0.6–1.2 mmol/L | Bipolar disorder and treatment‐resistant depression. | Prevention of affective relapses; reduction of suicide risk | [ |
| Xiong et al. (2023) | Observational Genetic‐Based Study | NS | Used as an augmentation therapy for antidepressants in TRD | Used in severe cases of TRD resistant to antidepressants | No specific adverse events discussed. | No specific data on treatment duration. | NS | NS | Major depressive disorder (MDD) | Lithium shows genetic effectiveness in TRD patients; more favorable genetic profile for response | [ |
| Vasquez et al. (2021) | Systematic Review and Meta‐Analysis | NS | Antidepressants + lithium, antidepressants + second‐generation antipsychotics (aripiprazole, olanzapine, fluoxetine, risperidone, ziprasidone) | NS | Tremor, dizziness, antipsychotic somnolence, akathisia. | Average of 3.4 weeks for lithium; 4 weeks for esketamine and 7 weeks for antipsychotics | NS | NS | Major depressive episodes (MDD). | Lithium is more effective as a combination therapy (NNT = 5) and has better tolerability compared to esketamine and antipsychotics | [ |
| Cipriani et al. (2013) | Systematic Review and Meta‐Analysis | NA | Lithium + placebo or amitriptyline, carbamazepine, imipramine, lamotrigine, mianserin, maprotiline, nortriptyline, olanzapine, phenelzine, quetiapine, thyroid hormone | NA | NA | ≥ 12 weeks | NS | NS | Unipolar depression, bipolar disorder | Lithium was associated with a reduced risk of suicide when compared with placebo, and also a reduce risk of deliberate self harm compared with carbamazepine, reduces risk of suicide and total deaths with both unipolar and bipolar depressive disorder | [ |
| Baldessarini et al. (2006) | Meta‐Analysis | Lithium with or without other treatments | Lithium with or without other treatments | NS | NS | Any duration | Any dosages | NS | Major affective disorders | Lithium provides major reductions in the risk of completed and attempted suicides among BD and other major affective disorder patients during long‐term treatment with lithium | [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBipolar Disorder and Treatment · Treatment of Major Depression · Electroconvulsive Therapy Studies
Introduction
1
Depression is a major contributor to the global disease burden [1]. It is estimated that 350 million people worldwide suffer from this condition [2]. Depression is characterized by a persistent alteration in mood that affects multiple domains of mental functioning: sleep, attention, motivation, cognitive and motor patterns, eating behavior, energy levels, and so forth, which impair an individual's functioning and increase morbidity and mortality risks [3]. Within this group, around 100 million people are estimated to suffer from treatment‐resistant depression (TRD), which is associated with even greater disability, impaired quality of life, and economic and social impacts [4].
The causes of depression are incompletely understood; however, there is evidence that depression is a complex interaction of biological, genetic, psychosocial, and environmental factors [5]. Antidepressant medications and cognitive behavioral therapy (CBT) are the main treatments for major depressive disorder (MDD), but 30%–50% of patients do not respond sufficiently to first‐line treatment [6].
Patients with treatment‐resistant depression have a higher risk of mortality, including due to suicide. However, mortality in patients with treatment‐resistant depression is also increased by other medical conditions or unknown causes. This underscores the need to prevent these complications through timely treatment of major depressive disorders and, eventually, treatment‐resistant depression [7]. The years of life lost and the direct and indirect costs associated with the treatment of MDD and TRD have a negative impact on the health and well‐being of the affected population. These effects include educational aspects, relationship stability, fertility, quality of childcare, and family income, among others [8].
There is no single definition of TRD; however, many studies adopt the definition used by the United States Food and Drug Administration (FDA) and the European Medicines Agency (EMA), which requires a minimum of two prior treatment failures and confirmation of adequate dosage and treatment duration (4–6 weeks) [9]. Other proposals stratify TRD based on multiple variables, such as the number and type of treatments used, the number of treatments, the duration of the depressive episode, and the severity of depression, as well as functional, personality, and contextual factors, among others [10]. This highlights the complexity of TRD, in which multiple risk factors, such as early‐life trauma, symptom severity, episode duration, psychotic symptoms, cognitive impairments, and comorbid disorders including personality and anxiety symptoms, play a role [4].
Several pharmacotherapeutic options to treat TRD have been studied, including increasing the dose of ongoing antidepressants, switching to another antidepressant, combining antidepressants, or augmentation with another medication with antidepressant effects.
However, evidence shows that augmentation with a second non‐antidepressant drug, such as lithium, second‐generation antipsychotics (SGA), thyroid hormones, ketamine, and dopaminergic agents, is the most effective option for TRD, with quetiapine and lithium being the most studied and well known [11].
Lithium Carbonate (Li2CO3) as a Therapeutic Agent
2
Lithium has been the cornerstone of treatment for bipolar disorder, for acute manic episodes, and long‐term prophylaxis to prevent new illness episodes [12]. Though lithium has shown similar efficacies in acute manic episodes when compared to other mood stabilizers, including valproate and SGA, such as olanzapine and haloperidol [13], its prophylactic properties have been demonstrated. An observational study comparing monotherapy with lithium and monotherapy with other mood stabilizers found that prophylactic lithium monotherapy was more effective as maintenance therapy than valproate, lamotrigine, olanzapine, and quetiapine [14]. In addition, lithium can reduce mortality by reducing the risk of suicide. The antisuicidal effect of lithium was shown in several meta‐analyses [15, 16], including one study that found that the risk of committing suicide was five times lower among patients with bipolar disorder, schizoaffective disorder, or major depressive disorder who received lithium therapy compared to patients who received other treatments (e.g., antidepressants, anticonvulsants, antipsychotics, or placebo) [15].
Lithium carbonate (Li_2_CO_3_) is an inorganic salt widely used in medical practice (Table 1). It has been employed as a treatment for mood‐related psychiatric disorders, earning recognition as a mood‐stabilizing agent since 1949 [17, 18]. Lithium has a narrow therapeutic index, necessitating careful monitoring to prevent adverse effects [19]. Lithium orotate, a dietary supplement available without a prescription, has reemerged as a potential therapeutic option for bipolar disorder and depression. However, there is insufficient evidence to confirm its effectiveness or establish clinical guidelines for its use, and it is not approved by the FDA [20].
Pharmacodynamic
2.1
The mechanism of action of lithium remains incompletely understood, although various theories have been proposed. One of the most extensively described mechanisms is the inhibition of glycogen synthase kinase‐3 (GSK‐3), an enzyme that plays a critical role in regulating numerous cellular functions, including dopaminergic and glutamatergic neurotransmission, synaptic plasticity, inflammation, circadian rhythm regulation, and apoptosis. Lithium‐induced inhibition of GSK‐3 may contribute to its antidepressant effects by modulating these pathways, enhancing neuronal plasticity, and promoting neuronal survival [21].
Additionally, lithium promotes the expression of brain‐derived neurotrophic factor (BDNF), a key factor for neurogenesis and neuronal repair [22]. BDNF acts on the mesocortical dopaminergic circuit, which may mediate its antidepressant effects. Evidence from animal models demonstrates that this mechanism involves the activation of dopaminergic neurons in the ventral tegmental area projecting to the medial prefrontal cortex [23].
Furthermore, lithium modulates intracellular signaling by displacing cations such as sodium and magnesium at specific binding sites, which can alter the function of key proteins involved in neuronal signal transmission. This displacement may stabilize inactive conformations of certain receptors, thereby reducing hyperactive signaling associated with mood disorders [24]. Lithium has extensive effects on intracellular calcium second messenger signaling.
Lithium also modulates neurotransmitters by inhibiting excitatory neurotransmission mediated by dopamine and glutamate while enhancing inhibitory neurotransmission mediated by gamma‐aminobutyric acid (GABA). Regarding serotonin, some studies suggest that lithium potentiates serotonergic neurotransmission, contributing to its antidepressant effect. This potentiation is particularly observed when lithium is combined with tricyclic antidepressants (TCAs) [25].
Finally, lithium exhibits immunomodulatory effects, suggesting that its ability to modify immune responses may be part of its mechanism of action in mood disorders and has effects on mitochondrial energy generation [26, 27, 28, 29, 30, 31] (Figure 1).
Representative schematic of the main mechanisms of action of lithium (Li+), including its specific molecular targets and the pathways it affects [27, 28, 29, 30, 31]. Lithium (Li+) exerts five principal mechanisms across distinct molecular pathways: (1) it inhibits GSK3, thereby disinhibiting the CREB pathway and potentiating Wnt/β‐catenin, which promotes expression of neuroprotective factors (BDNF, BCL‐2), while simultaneously suppressing pro‐inflammatory signals mediated by NFκB and STAT3, activating Nrf2 and modulating autophagy, stimulating the PI3K/Akt complex to further reinforce GSK3 inhibition, and activating the clock proteins CLOCK and REV‐ERBα to regulate circadian rhythms; (2) it regulates mTOR and AMPK—initially activating mTOR following GSK3 inhibition but, under metabolic stress, triggering AMPK to inhibit mTOR and thereby promote nuclear protein synthesis and selective endoplasmic reticulum autophagy; (3) it acts complementarily on NFκB by directly inhibiting this pro‐inflammatory complex; (4) it further enhances the CREB pathway and miRNA‐mediated regulatory mechanisms to boost transcription of neuroprotective factors; and (5) it blocks the IPPase and IMPase enzymes, reducing generation of IP3 and DAG, which diminishes PKC and MARCKS activation, retains PIP2 in the membrane, reduces Ca2+ release from the endoplasmic reticulum, and dampens synaptic neurotransmitter release—collectively contributing to decreased ER stress, protein misfolding, apoptosis, and inflammation. AC, adenylate cyclase; Akt, protein kinase B; AMPK, AMP‐activated protein kinase; BCL‐2, B‐cell lymphoma 2; BDNF, brain‐derived neurotrophic factor; Ca2+, calcium; cAMP, cyclic adenosine monophosphate; CHOP, C/EBP homologous protein; CLOCK, Circadian Locomotor Output Cycles Kaput; CREB, cAMP response element‐binding protein; DAG, diacylglycerol; eIF2α, eukaryotic initiation factor 2 alpha; ERS/UPR, endoplasmic reticulum stress/unfolded protein response; G, G protein–coupled receptor; GRP78, glucose‐regulated protein 78; GRP94, glucose‐regulated protein 94; GSK3, glycogen synthase kinase‐3; IFNγ, interferon gamma; IGF, insulin‐like growth factor; IL‐1β, interleukin‐1 beta; IMPase, inositol monophosphatase; IP, inositol monophosphate; IP₂, inositol 1,4‐bisphosphate; IP₃, inositol 1,4,5‐trisphosphate; IP₃R, inositol 1,4,5‐trisphosphate receptor; IPPase, inositol polyphosphate phosphatase; IRE1, inositol‐requiring enzyme 1; Li+, lithium ion; MARCKS, myristoylated alanine‐rich C‐kinase substrate; MI, myo‐inositol; miRNAs, microRNAs; mTOR, mechanistic target of rapamycin; NFκB, nuclear factor kappa B; Nrf2, nuclear factor erythroid 2‐related factor 2; PI3K, phosphatidylinositol 3‐kinase; PIP₂, phosphatidylinositol 4,5‐bisphosphate; PIP₃, phosphatidylinositol 3,4,5‐trisphosphate; PKC, protein kinase C; PLC, phospholipase C; REV‐ERBα, nuclear receptor subfamily 1 group D member 1; ROS, reactive oxygen species; STAT3, signal transducer and activator of transcription 3; TCF/LEF, T‐cell factor/lymphoid enhancer factor; TLR4, Toll‐like receptor 4; TNF‐α, tumor necrosis factor alpha; VEGF, vascular endothelial growth factor; Wnt/β‐cat, Wnt/β‐catenin pathway; XBP1, X‐box binding protein 1.
Pharmacokinetics
2.2
Lithium primarily follows linear or first‐order kinetics, meaning its elimination is proportional to its plasma concentration. As the dose increases, lithium plasma concentrations rise in a quasi‐linear manner [32]. Regarding lithium pharmacokinetics, the following parameters describe the processes by which the ion is released, absorbed, distributed, metabolized, and eliminated. This drug transformation process is recognized by the acronym LADME, which stands for liberation, absorption, distribution, metabolism, and excretion. In this model, liberation refers to the release of the active pharmaceutical ingredient from its dosage form prior to absorption. Lithium is administered orally in the form of lithium carbonate, available in immediate‐ or extended‐release capsules, tablets, and oral solution (Table 2) [37].
Absorption
2.2.1
Lithium absorption occurs rapidly in the gastrointestinal tract, specifically in the small intestine. (3) Standard‐release formulations reach peak plasma concentrations within 1–2 h, whereas sustained‐release formulations do so in 4–5 h [38].
Distribution
2.2.2
Lithium has a large volume of distribution (0.5–0.9 L/kg in adults), distributing throughout the body similarly to total body water. This indicates extensive tissue penetration and widespread distribution [39]. One of the most important characteristics of lithium is its slow cellular uptake, with some degree of accumulation observed in tissues such as bones and the thyroid gland, with an initial distribution half‐life of, on average, 5 h [40]. This drug does not significantly bind to plasma proteins and is unevenly distributed among different body compartments, including the brain, kidneys, and muscles [39]. Notably, lithium follows a bicompartmental pharmacokinetic profile, with rapid distribution in a central compartment (blood and highly perfused organs) followed by slower distribution in peripheral tissues (e.g., muscles and fat) [41]. For accurate therapeutic monitoring, serum lithium levels should be measured after the distribution phase is complete, generally 8–10 h after oral administration.
Metabolism and Elimination
2.2.3
Lithium is not metabolized by the liver or any other organ; it undergoes no biotransformation in the human body, remaining unchanged. This distinguishes it from many other drugs that undergo hepatic metabolism [33]. Because lithium is not metabolized, its elimination does not depend on liver function. Instead, it is excreted unchanged, primarily through the kidneys, accounting for more than 95% of its clearance. Renal clearance ranges between 0.51 and 1.59 L/h and is closely related to kidney function [42].
Although lithium exhibits linear pharmacokinetics within the therapeutic range, its clearance can behave nonlinearly under clinical conditions. This is because, although it is eliminated primarily by glomerular filtration (a linear process), it also undergoes tubular reabsorption in the proximal nephron, competing with sodium. Factors such as sodium depletion, dehydration, or the concomitant use of diuretics, non‐steroidal anti‐inflammatory drugs (NSAIDs), or angiotensin‐converting enzyme (ACE) inhibitors can increase lithium reabsorption, reducing its elimination and causing disproportionate plasma accumulation. Therefore, although its basic kinetics are linear, its elimination can become nonlinear under common physiological or pharmacological influences. Additionally, lithium clearance may vary throughout the day, with lower rates observed at night compared to daytime [43]. The plasma elimination half‐life of lithium is 18–36 h and can vary depending on the patient's renal function [40]. During pregnancy, lithium clearance increases significantly (up to 63% in the third trimester) due to an increase in the glomerular filtration rate, further reinforcing its strong dependence on renal function [44].
Understanding Lithium's Potential as an Antidepressant Augmentation Agent
3
Lithium is a drug of choice for maintenance treatment of bipolar disorder; however, it has also shown efficacy in unipolar depressed patients as an augmentation therapy. Lithium augmentation was first reported in the 1980s to be effective in treating patients with depression who failed to respond to TCAs [45]. The effectiveness of lithium augmentation for depression was evaluated in the STAR*D (sequenced treatment alternatives to relieve depression) trial [46], where different antidepressant switching and augmentation therapies were examined [47]. The effectiveness of lithium augmentation was compared to triiodothyronine (T (3)) augmentation as a third‐step treatment for patients with MDD who had initially failed to remit to treatment with citalopram and subsequently failed to remit after a second antidepressant or augmentation strategy prior to randomization to lithium (up to 900 mg/day; N = 69) or T (3) (up to 50 μg/day; N = 73) for up to 2 weeks. In this trial, the remission rates were 15.9% with lithium augmentation and 24.7% with T (3) augmentation; the difference was not statistically significant. T (3) augmentation was concluded to be superior to lithium augmentation due to better tolerability of T (3) compared to lithium. However, this trial had limitations such as the lack of a placebo comparator, the open‐label administration of the augmentation therapies, and a study design that selects participants who have progressed through previous steps [46].
In a recent meta‐analysis, the efficacy and safety of SGA, esketamine, and lithium as antidepressant augmentation agents were compared. Randomized, placebo‐controlled trials were reviewed using meta‐analysis to compare the odds ratio (OR) to achieve response versus placebo [48]. They calculated the numbers needed to treat (NNT) and numbers needed to harm (NNH) when adding a SGA, esketamine, or lithium to antidepressants during major depressive episodes. The NNT for lithium was 5 (95% confidence interval (CI) 4–10) compared to SGAs with a NNT of 11 (95% CI: 9–15) and esketamine with a NNT of 7 (95% CI 4–10). Tolerability to lithium had a NNH of 9 (95% CI: 5–106); for SGAs, NNH was 5 (95% CI 4–6), and for esketamine, NNH was 5 (95% CI 4–6). Finally, the risk/benefit ratio was highest for lithium with an NNH/NNT of 1.80 (95% CI 1.25–10.60). The study demonstrates that SGA and esketamine are effective in combination with other antidepressants for acute major depressive episodes. However, lithium showed slightly higher efficacy and better tolerability compared to the other drugs [47].
Lithium is widely recognized for its ability to prevent relapse and recurrence of mood episodes, reduce aggression, impulsivity, and suicide risk, as well as reducing all‐cause mortality [49, 50]. Randomized clinical trials and meta‐analyses estimate a reduction in suicidal death of approximately 60%–70% with lithium and a reduction in all‐cause mortality of around 60% compared to placebo or other active treatments [16]. Lithium augmentation therapy is recommended in patients with TRD (see Table 3) and high risk of suicide; other indications include history of more than three major depressive episodes, psychomotor retardation, and weight loss. It also seems to be more effective in patients with a first‐degree relative with mood disorders [19].
A systematic review of lithium to treat unipolar major depressive disorder documented six trials of lithium monotherapy and 12 trials of lithium augmentation to antidepressants for acute depression as well as 21 trials of lithium as monotherapy or adjunct to antidepressant treatment for long‐term prophylaxis [55]. Randomized trials included lithium as monotherapy or adjunctive with an antidepressant, compared to placebo or antidepressant monotherapy. Short‐term trials were defined as at least 1 week and up to 12 weeks of follow‐up, and long‐term trials as ≥ 12 weeks of follow‐up. Lithium monotherapy was not effective for the treatment of acute depressive episodes, where it was equivalent to placebo treatment. However, the efficacy of lithium as an augmentation agent to antidepressants favored lithium over placebo (OR 2.34 (95% CI 1.57–3.51); p < 0.0001). Interestingly, lithium monotherapy was superior to placebo, and lithium adjunctive therapy was superior to antidepressant monotherapy for long‐term prophylactic treatment (OR 2.80 (95% CI: 1.59–4.92); p < 0.0001).
One of the most recent meta‐analyses aimed to compare antidepressants (selective serotonin reuptake inhibitors (SSRIs), serotonin‐norepinephrine reuptake inhibitors (SNRIs), TCAs, monoamine oxidase inhibitors (MAOIs), norepinephrine‐dopamine reuptake inhibitors (DNRIs), agents targeting the glutamatergic system (e.g., ketamine and esketamine)), and augmentation agents (mood stabilizers, SGAs, thyroid hormones, anticonvulsants, and 5‐hydroxytryptamine (HT) partial agonist) on the basis of their efficacy, tolerability, and speed of symptom relief in TRD; the meta‐analyses included a total of 66 articles. Lithium was an augmentation agent in 16 articles (TCA: 9; SSRIs/SNRIs/NDRIs: 7). The study found that ketamine and esketamine, as well as lithium augmentation and combining antidepressants, were effective treatments for patients with TRD [60].
The use of lithium in combination with other augmentation agents, such as ketamine, has been studied in TRD. A randomized, double‐blind clinical trial conducted between 2013 and 2016 compared ketamine infusions plus lithium versus ketamine infusions with a placebo in patients with treatment‐resistant unipolar depression. Following an initial session of ketamine infusion, patients were randomized to receive lithium or placebo, as well as three additional sessions of ketamine. The results indicated no significant difference in depression severity between the two groups, as measured by the Montgomery–Åsberg Depression Rating Scale (MADRS), suggesting no additional improvement with the addition of lithium [52].
The presence of some adverse effects such as weight gain, tremor, thyroid dysfunction, and gastrointestinal dysfunction could influence adherence to lithium therapy. In a qualitative assessment aimed at evaluating opinions of lithium and quetiapine augmentation in patients with TRD, four main themes were generated as follows: initial concerns, experience of side effects, perception of treatment efficacy, and positive perception of treatment monitoring. Participants indicated a positive experience of lithium and quetiapine augmentation, although some patients held beliefs that suggested greater apprehension towards lithium than quetiapine [54]. This suggests that appropriate education should be provided to every patient and their families before initiating lithium therapy, addressing questions, doubts, and the possible fears patients might have.
The combination of neuromodulation therapies, such as electroconvulsive therapy (ECT) with lithium, has generated conflicting data. Although this approach appears to be more effective than either lithium or ECT alone, evidence suggests an increased risk of delirium and neurocognitive side effects. An observational study of 64,728 patients, examining the association between these adverse effects and the combined use of ECT and lithium, compared to ECT alone, found a higher risk of acute delirium with ECT and lithium in patients with major depressive disorder (7.8%) compared to those with bipolar disorder (3.4%). Cognitive impairment was also higher for all patients pooled who received a combination of lithium and ECT (2.4%) versus ECT only (0.5%). Therefore, clinicians should exercise caution when using this combination. However, available data remain limited [56].
On the other hand, following a successful course of ECT for depression, continuation ECT combined with lithium has been shown to reduce the risk of relapse. A systematic review and meta‐analysis that included 14 studies and 9748 patients receiving continuation ECT (N = 1571 with lithium and N = 8177 without lithium), with follow‐up durations ranging from 15 to 58 weeks, found that the group treated with lithium had significantly lower relapse rates, with a weighted OR of 0.53 and a NNT of 7 [61].
Although lithium is used more cautiously in geriatric patients because of the differences in efficacy and tolerability among older patients compared to young patients [57], it is important to know how to use it and what care needs to be taken when it is used in older patients. Adults ≥ 65 years of age require lower doses of lithium to achieve similar plasma concentrations because of age‐related changes, such as a reduced glomerular filtration rate. A prospective multicenter cohort study investigated the estimated glomerular filtration (eGFR) rate changes and number of acute kidney injuries (AKI) following lithium augmentation therapy in adults ≥ 65 years compared with patients < 65 years of age. The study showed that two variables, age ≥ 65 years and serum lithium levels, had a negative effect on eGFR. Two AKIs were observed in the ≥ 65‐years group when serum lithium exceeded the therapeutic range of > 0.8 mmol/L. [53] The recommended target serum lithium levels should be < 0.6 mmol/L in this population.
Key Factors Influencing Lithium Treatment Response
4
About half of individuals with depression show an inadequate response to lithium augmentation, even though it has demonstrated greater efficacy compared to placebo [6]. Several biological variables include a higher cortisol–adrenocorticotropic hormone (ACTH) ratio in the dexamethasone suppression‐corticotropin‐releasing hormone stimulation test (DEX‐CRH) in poorer responders, in which, after stimulation of the hypothalamus–pituitary–adrenocortical (HPA) system by ACTH, cortisol and ACTH are raised due to a sensitivity to the adrenal cortex. Evidence demonstrates a higher ratio of non‐response in patients with a more chronic depression course, given that one of the biological changes associated with chronic illness is the enlargement of the adrenal gland with an increased sensitivity to ACTH. Studies in rats showed an increase in the neuroprotective protein B‐cell lymphoma 2 (bcl‐2) in the frontal cortex and hippocampus and an increased expression of the major protein kinase C (PKC) substrate, myristoylated alanine‐rich C‐kinase substrate (MARCKS) [6, 58].
Patients who present with severe depressive symptomatology, weight loss, psychomotor retardation, a history of more than three major depressive episodes, and a first‐degree relative with mood disorders may have shown better outcomes from lithium therapy [45].
In 2009, the International Consortium on Lithium Genetics (ConLiGen) was established with the goal of conducting the first genome‐wide association study (GWAS) on lithium response in 2563 individuals with bipolar disorder. This landmark study identified genetic markers associated with long noncoding RNAs. More recent research has demonstrated that polygenic scores for certain psychiatric disorders, such as MDD and schizophrenia, are linked to poor lithium response [58]. These findings highlight lithium's limited effectiveness in patients with a genetic predisposition to psychotic symptoms.
Ying Xiong et al. conducted a study to explore the relationship between polygenic risk scores (PRS) and treatment resistance in MDD. They analyzed 4500 individuals with MDD, defining two phenotypes: TRD and non‐resistant depression (non‐TRD). PRS were generated for both antidepressant and lithium responses. Although no significant differences were found in PRS for antidepressant responses between the two groups, TRD cases showed significantly higher PRS for lithium response compared with non‐TRD cases [59]. These results suggest a genetic predisposition influencing lithium sensitivity in TRD.
Advantages of Lithium in the Clinical Context
5
Edwards et al. conducted a systematic review and economic evaluation of lithium and SGA in the management of TRD. In this study, costs generally included laboratory monitoring—such as lithium plasma level determinations and renal and thyroid function tests—along with other clinical assessments and related visits. They identified four economic evaluations in the management of TRD and five studies that reported utility values for different levels of depression severity and treatment response. The systematic review showed that the annual cost per patient treated with SSRI + lithium was estimated to be €4739 compared with €5644 for those treated with SSRI + SGA [5], supporting lithium as an option for long‐term treatment for either bipolar disorder or TRD.
These results align with a review by Catalano et al. in 2020, which examined the cost‐effectiveness of lithium combined with thyroid hormones, aripiprazole, brexpiprazole, quetiapine, and buspirone. The study concluded that lithium offered both a low unit cost (140.40 quetiapine vs. $96.30 lithium) [51].
Evidence supports the use of lithium in the prevention of hospitalization for patients with mood disorders. In a cohort study which aimed to assess the risk of rehospitalization of 123,712 patients with severe recurrent depression between 1996 and 2012, lithium was associated with a reduced risk of rehospitalization. In addition, treatment with lithium plays a crucial role in reducing mortality, particularly by preventing suicide [13]. A meta‐analysis conducted by Baldessarini et al. included 45 studies with data on suicides that occurred during an average of 1.5 years of lithium treatment as well as 34 studies reporting suicides among individuals who did not receive lithium. The results showed that the risk of suicide was five times lower in patients treated with lithium compared to those who received other treatments [15].
In recent years, the neuroprotective effect of lithium has been studied in mood and neurocognitive disorders [13]. Retrospective studies have demonstrated that patients on long‐term lithium therapy were much less likely to develop neurological disorders such as dementia, seizures, or amyotrophic lateral sclerosis. This has been associated with lithium's role in modulating autophagy as well as its ability to mitigate neuroinflammation and to preserve and even increase telomere length [62, 63].
To maximize safety, before starting treatment with lithium, every patient should have a baseline thyroid hormone evaluation including thyroid‐stimulating hormone (TSH). Kidney function tests also should be measured, including sodium levels, given their direct relationship with lithium and electrocardiogram (EKG) if patients have cardiovascular risk factors or are ≥ 40 years of age. An empirical starting dose of 300 mg twice daily is frequently used for lithium augmentation in clinical practice; however, individualized dose calculations based on pharmacokinetic principles may allow faster attainment of therapeutic concentrations, optimizing both clinical outcomes and resource use. Because of the toxicity risk with a prolonged treatment duration and high doses, lithium serum levels should be monitored every 3–6 months, unless another medication that can alter lithium levels is initiated, in which case lithium serum levels should be monitored more frequently. More frequent monitoring is also recommended in cases of dose adjustments, changes in renal function, or when clinical signs of toxicity appear. Target lithium serum levels are 0.5–0.8 mEq/L [19].
Conclusions
6
The evidence reviewed in this article suggests that lithium augmentation is a suitable option for the treatment of TRD, as it helps enhance the effects of other antidepressant agents and offers advantages such as reducing hospitalizations and lowering mortality by reducing suicide. However, strict monitoring is required to reduce adverse reactions and complications from long‐term use. Lithium is a cost‐effective drug that may have a role in the management of TRD. Nevertheless, many studies evaluating lithium augmentation in TRD were conducted in the past decades using older antidepressants. More updated studies that include newer antidepressants are needed to evaluate lithium augmentation and its nuances in TRD.
Author Contributions
Angela Acero‐González: writing – original draft, writing – review and editing. Yahira Guzman: supervision, writing – original draft, writing – review and editing. Nadia Juliana Proaños: writing – original draft, writing – review and editing. Rosa‐Helena Bustos: writing – original draft, writing – review and editing. María Aconcha: writing – original draft, writing – review and editing. Ivan Guerrero: writing – original draft, writing – review and editing. Laura Alejandra Martinez: writing – original draft, writing – review and editing. Michael Berk: writing – original draft, writing – review and editing. Seetal Dodd: writing – original draft, writing – review and editing.
Conflicts of Interest
M.B. is supported by a NHMRC senior principal research fellowship and leadership 3 investigator grant (1156072 and 2017131), has received grant funding from Wellcome Trust, MRFF, Victorian Government Department of Jobs, Precincts and Regions, Cooper University USA, Janssen Lundbeckfonden Copenhagen, St. Biopharma, Psychscene.com, WFSBP, NeuroSAS, CINP, Shanghai Mental Health Center, Penn State College of Medicine, Precision Psych Fondamental, ISBD, Milken Baszucki Brain Research Fund, Stanley Medical Research Institute, Danmarks Frie Forskningsfond Psykiatrisk Center Kovenhavn, Patient‐Centered Outcomes Research Institute (PCORI), Australian Eating Disorders Research and Translation Centre AEDRTC, USA Department of Defense Office of the Congressionally Directed Medical Research Programs (CDMRP), Equity Trustees Limited, and has provided lectures for Global Congress of Biological Psychiatry India, Otsuka CNS, RANZCP New Zealand, Eisai Australia, Sandoz, Allori, Lundbeck, World Congress of Psychiatry, African College of Neuropsychopharmacology, SVI Inaugural Health Matters Webinar Series, Argeninte Association of Psychiatrists Congress of Psychiatry and Mental Health, Global Bipolar Cohort (GBC). S.D. has received grant support from the Stanley Medical Research Institute, NHMRC, Beyond Blue, ARHRF, Simons Foundation, Geelong Medical Research Foundation, Harry Windsor Foundation, Fondation FondaMental, Eli Lilly, Glaxo SmithKline, Organon, Mayne Pharma and Servier, speaker's fees from Eli Lilly, advisory board fees from Eli Lilly and Novartis, and conference travel support from Servier. All other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. J. Ferrari , D. F. Santomauro , A. Aali , et al., “Global Incidence, Prevalence, Years Lived With Disability (YL Ds), Disability‐Adjusted Life‐Years (DAL Ys), and Healthy Life Expectancy (HALE) for 371 Diseases and Injuries in 204 Countries and Territories and 811 Subnational Locations, 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021,” Lancet 403, no. 10440 (2024): 2133–2161.38642570 10.1016/S 0140-6736(24)00757-8PMC 11122111 · doi ↗ · pubmed ↗
- 2World Health Organization , “World Mental Health Report: Transforming Mental Health for All,” accessed January 13, 2025, https://www.who.int/publications/i/item/9789240049338.
- 3Association AP , Diagnostic and Statistical Manual of Mental Disorders, vol. 21, 5th ed. (Association AP, 2022), 591–643.
- 4R. S. Mc Intyre , M. Alsuwaidan , B. T. Baune , et al., “Treatment‐Resistant Depression: Definition, Prevalence, Detection, Management, and Investigational Interventions,” World Psychiatry: Official Journal of the World Psychiatric Association 22, no. 3 (2023): 394–412.10.1002/wps.21120 PMC 1050392337713549 · doi ↗ · pubmed ↗
- 5S. J. Edwards , V. Hamilton , L. Nherera , and N. Trevor , “Lithium or an Atypical Antipsychotic Drug in the Management of Treatment‐Resistant Depression: A Systematic Review and Economic Evaluation,” Health Technology Assessment 17, no. 54 (2013): 1–190.10.3310/hta 17540 PMC 478129824284258 · doi ↗ · pubmed ↗
- 6M. Bauer , M. Adli , C. Baethge , et al., “Lithium Augmentation Therapy in Refractory Depression: Clinical Evidence and Neurobiological Mechanisms,” Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie 48, no. 7 (2003): 440–448.12971013 10.1177/070674370304800703 · doi ↗ · pubmed ↗
- 7G. Li , D. Fife , G. Wang , et al., “All‐Cause Mortality in Patients With Treatment‐Resistant Depression: A Cohort Study in the US Population,” Annals of General Psychiatry 18 (2019): 23.31583010 10.1186/s 12991-019-0248-0PMC 6771113 · doi ↗ · pubmed ↗
- 8R. D. Sousa , M. Gouveia , C. Nunes da Silva , et al., “Treatment‐Resistant Depression and Major Depression With Suicide Risk‐The Cost of Illness and Burden of Disease,” Frontiers in Public Health 10 (2022): 898491.36033799 10.3389/fpubh.2022.898491 PMC 9402971 · doi ↗ · pubmed ↗