When the Heart Breaks in the Operating Room (OR): Intraoperative Arrest as a First Sign of Takotsubo Cardiomyopathy
Clara Pereira, Raquel Louzada, Bernardo Matias, Irene Ferreira

TL;DR
A patient had a heart attack during surgery, leading to the diagnosis of a rare heart condition called Takotsubo cardiomyopathy.
Contribution
Highlights Takotsubo cardiomyopathy as a possible cause of intraoperative cardiac arrest in otherwise healthy patients.
Findings
Intraoperative cardiac arrest can be the first sign of Takotsubo cardiomyopathy.
Early recognition and multidisciplinary management are crucial for favorable outcomes.
Takotsubo cardiomyopathy should be considered in differential diagnosis of perioperative cardiac arrest.
Abstract
Cardiac arrest in the operating room is a rare but potentially life-threatening event. This report discusses a case in which a seemingly healthy patient presented for elective total thyroidectomy and experienced intraoperative cardiac arrest requiring cardiopulmonary resuscitation. Takotsubo cardiomyopathy was diagnosed following resuscitation. This case underscores the need for heightened awareness and consideration of Takotsubo cardiomyopathy as a differential diagnosis in cases of perioperative cardiac arrest, particularly when initial findings do not align with typical causes such as myocardial infarction or arrhythmia. Multidisciplinary collaboration, early recognition, and appropriate management are crucial to ensuring patient safety and achieving favorable recovery in such complex clinical scenarios.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
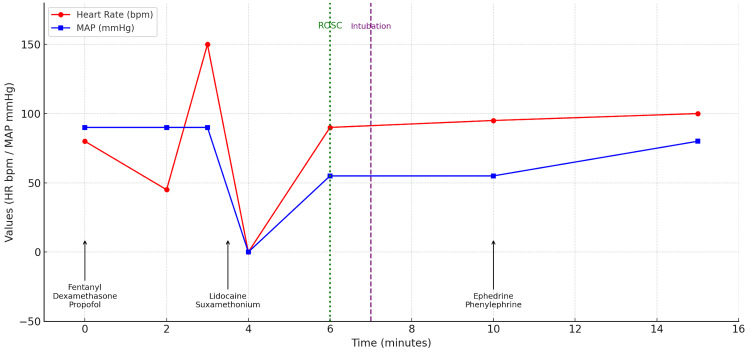 Figure 1
Figure 1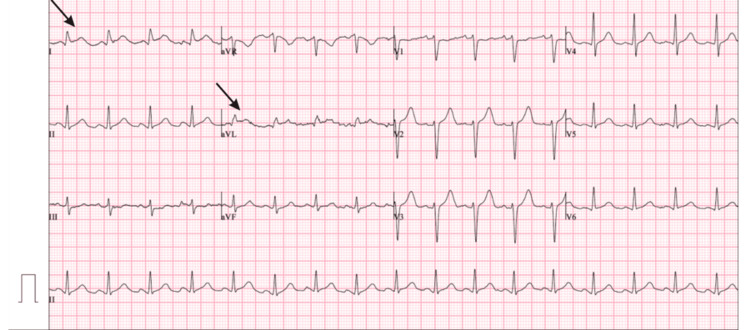 Figure 2
Figure 2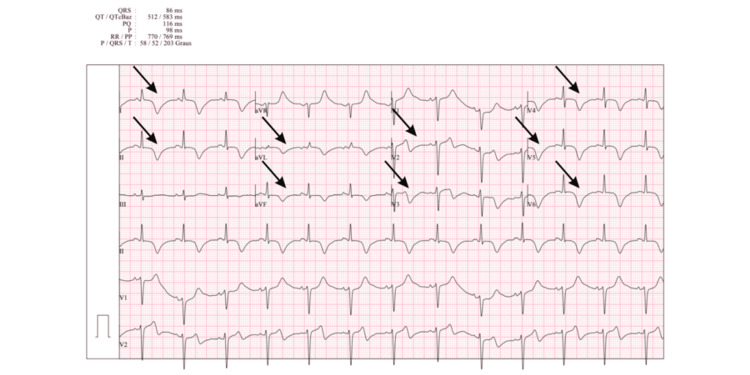 Figure 3
Figure 3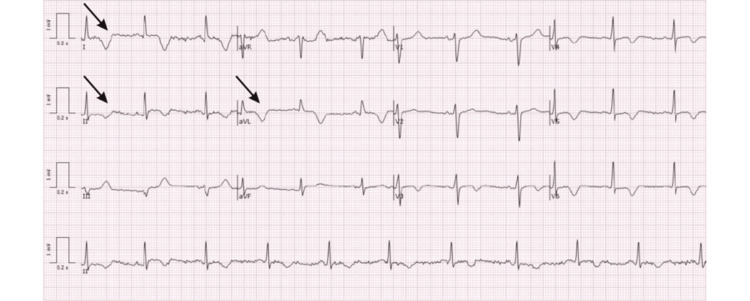 Figure 4
Figure 4| Parameter | Result | Normal range |
| pH | 7.39 | 7.35-7.45 |
| Partial pressure of carbon dioxide (PaCO₂) | 38 mmHg | 35-45 mmHg |
| Bicarbonate (HCO₃⁻) | 23 mmol/L | 22-26 mmol/L |
| Partial pressure of oxygen (PaO₂) | 106 mmHg | 80-100 mmHg |
| Sodium (Na⁺) | 135 mmol/L | 135-145 mmol/L |
| Potassium (K⁺) | 3.9 mmol/L | 3.5-5 mmol/L |
| Chloride (Cl⁻) | 106 mmol/L | 98-106 mmol/L |
| Ionized calcium (Ca²⁺) | 1.21 mmol/L | 1.12-1.32 mmol/L |
| Glucose | 134 mg/dL | 70-140 mg/dL |
| Lactate | 0.9 mmol/L | 0.5-2.2 mmol/L |
| Oxygen saturation (SaO₂) | 99% | ≥95% |
| Parameter | Result | Normal range |
| Hemoglobin (Hb) | 12.8 g/dL | 12.0-16.0 g/dL |
| White blood cell count (WBC) | 6.1 x 10⁹/L | 4.0-11.0 × 10⁹/L |
| Platelet count | 121 x 10⁹/L | 150-400 × 10⁹/L |
| Creatinine | 0.91 mg/dL | 0.6-1.2 mg/dL |
| TSH | 2.6 mIU/L | 0.4-4.0 mIU/L |
| FT4 | 1.1 ng/dL | 0.8-2.0 ng/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTakotsubo Cardiomyopathy and Associated Phenomena · Cardiovascular Issues in Pregnancy · Cardiac Imaging and Diagnostics
Introduction
Cardiac arrest in the operating theater, although uncommon, remains a serious and potentially life-threatening event that demands immediate attention and coordinated intervention. The perioperative period is a vulnerable time for patients, as surgical stress, anesthesia, and underlying comorbidities contribute to an elevated risk of cardiopulmonary complications, such as cardiac ischemia and arrhythmias. Even in patients deemed low-risk or undergoing elective procedures, unanticipated cardiovascular events may occur with minimal or no warning signs. Cardiac arrest during surgery presents a unique diagnostic and therapeutic challenge, particularly when the cause is not immediately evident [1].
Among the various potential etiologies of perioperative cardiac arrest, Takotsubo cardiomyopathy (TC), also known as stress-induced cardiomyopathy or "broken heart syndrome," has gained increasing recognition in recent years as a reversible cause of acute cardiac dysfunction. TC is characterized by transient systolic dysfunction of the left ventricle, often with apical ballooning, in the absence of significant coronary artery obstruction. While the syndrome mimics acute coronary syndrome both clinically and electrocardiographically, coronary angiography typically reveals no obstructive lesions, and cardiac function usually recovers within days to weeks [1,2].
The precise pathophysiology of TC remains a subject of ongoing research. Several mechanisms have been proposed, including multivessel coronary vasospasm, microvascular dysfunction, and the presence of occult coronary artery disease. However, the prevailing hypothesis involves a surge in catecholamines in response to acute physical or emotional stress, which leads to calcium overload and subsequent myocardial stunning. This excess adrenergic stimulation is thought to impair myocardial contractility, particularly in the apical segments of the left ventricle, through both direct toxic effects on cardiomyocytes and alterations in coronary microcirculation. The perioperative setting, with its inherent physiological stressors, including pain, anxiety, hemodynamic fluctuations, and pharmacologic agents, creates an environment conducive to the development of TC [2].
Although TC is generally considered a transient condition with a favorable prognosis, its presentation during the perioperative period can be dramatic and may mimic life-threatening conditions such as myocardial infarction. The risk of misdiagnosis or delayed diagnosis is considerable, especially in the acute intraoperative phase, when standard diagnostic tools may not be immediately available. Furthermore, the condition may precipitate or coincide with arrhythmias, hypotension, heart failure, or even cardiac arrest, as highlighted in the case presented in this report [1].
This article presents a case of intraoperative cardiac arrest in a previously healthy patient undergoing elective thyroid surgery, where subsequent investigations revealed TC as the underlying cause. The case highlights the importance of considering TC in the differential diagnosis of unexplained cardiac arrest during surgery and underscores the need for heightened awareness, prompt recognition, and appropriate management to optimize patient outcomes.
Case presentation
A 40-year-old woman, classified as American Society of Anesthesiologists (ASA) Physical Status II, presented for elective total thyroidectomy for toxic multinodular goiter. Her medical history included class I obesity and a known penicillin allergy. She had no history of previous surgeries or cardiovascular or respiratory disease, and no family history of anesthetic complications. Her only regular medication was methimazole 5 mg daily. Preoperative laboratory investigations, including thyroid function tests, were within normal reference ranges.
General anesthesia was planned with standard monitoring. Immediately prior to induction, the patient received intravenous fentanyl 150 µg, dexamethasone 8 mg, and target-controlled infusion of propofol, given according to the Schneider pharmacokinetic model, with a target blood concentration of 5 μg/mL.
Shortly after propofol administration, she developed bradycardia (heart rate decreased to 45 bpm), followed by abrupt sinus tachycardia with a peak heart rate of 150 bpm. During this period, the mean arterial pressure (MAP) ranged between 80 and 100 mmHg, and oxygen saturation remained at 100%. Following the administration of intravenous lidocaine 100 mg and suxamethonium 50 mg, the patient developed ventricular tachycardia progressing rapidly to ventricular fibrillation.
Advanced Life Support (ALS) protocols were immediately initiated, resulting in return of spontaneous circulation (ROSC) after approximately two minutes, without shocks or any drugs. Postresuscitation management included orotracheal intubation with a size 6.5 tube and placement of a radial arterial catheter. The patient remained in sinus rhythm, with a heart rate ranging between 80 and 110 bpm. The initial MAP was 55 mmHg, improving to 80 mmHg following administration of ephedrine 6 mg and phenylephrine 50 µg (Figure 1).
Intraoperative timeline.Red circles/line: heart rate (HR); blue squares/line: mean arterial pressure (MAP); black arrows with text: timing of drug administrations; green dotted line: return of spontaneous circulation (ROSC); purple dashed line: intubation.
Twelve-lead electrocardiogram (ECG) showed sinus rhythm (heart rate 102 bpm), 1 mm ST-segment elevation in leads I and aVL, narrow QRS complexes with normal PR interval, preserved R-wave progression (V1-V3), and a corrected QT interval (QTc) of 454 ms. No features of pre-excitation or Brugada pattern were identified (Figure 2).
First 12-lead electrocardiogram after resuscitation.Arrows: 1 mm ST-segment elevation in leads I and aVL.
Transthoracic echocardiography revealed a non-dilated left ventricle with moderate systolic dysfunction (estimated ejection fraction 35%-40%) and regional wall motion abnormalities involving the apex, all apical segments, and the mid-anterior and mid-lateral walls. Right ventricular size and function were preserved. Mild mitral and mild-to-moderate tricuspid regurgitation were noted; there was no pericardial effusion.
Following neurological recovery, the patient resumed spontaneous ventilation and was extubated safely. She was alert, cooperative, and asymptomatic, with no evidence of pain or cardiorespiratory distress. Arterial blood gas analysis showed the results presented in Table 1, which were within normal limits.
The patient was transferred to the coronary intensive care unit (CICU) for further management. Coronary angiography revealed no evidence of obstructive coronary artery disease. Laboratory investigations demonstrated the results presented in Table 2, which were within normal limits. Peak serum troponin I concentration was 1,380 pg/mL (normal range: <40 pg/mL), with a downward trend thereafter. N-terminal prohormone of brain natriuretic peptide (NT-proBNP) was markedly elevated at 9,413 pg/mL (normal range: <125 pg/mL). Serial ECGs showed progressive T-wave inversions and QTc prolongation, peaking at approximately 583 ms (Figure 3).
Twelve-lead electrocardiogram showing T-wave inversions and QTc prolongation (583 ms).Arrows: T-wave inversions.
β-Blocker therapy with bisoprolol was initiated and was well tolerated. Clinical status and imaging findings improved progressively. Repeat echocardiography showed complete recovery of left ventricular ejection fraction and resolution of regional wall motion abnormalities. Cardiac magnetic resonance imaging (MRI) with adenosine stress perfusion (140 µg/kg/min) performed more than two weeks after the event demonstrated preserved biventricular function, with no evidence of myocardial necrosis, fibrosis, or ischemia.
The history of penicillin allergy may indicate a tendency to hypersensitivity reactions, but it does not necessarily imply an increased predisposition to anaphylaxis from unrelated agents. Therefore, an evaluation by the immunoallergology service was performed, and the test results were negative. The clinical, electrocardiographic, and echocardiographic features were consistent with TC triggered by anesthetic induction.
The patient’s subsequent 31-day hospital stay was uneventful, with no recurrence of arrhythmias, ischemic symptoms, or signs of fluid overload. She remained hemodynamically stable. At discharge, the ECG demonstrated sinus rhythm at 60 bpm; persistent T-wave inversions in leads I, II, aVL, and V4-V6; biphasic T-waves in V3; and a QTc of 477 ms (Figure 4).
Twelve-lead electrocardiogram at discharge.Arrows: T-wave inversions in leads I, II, and aVL.
The patient remained asymptomatic from a cardiovascular perspective.
Discussion
The prevention and successful management of cardiac arrest during anesthesia require high clinical vigilance, early recognition, and a well-coordinated response [1,2]. Even patients with a low predicted risk of perioperative cardiovascular events may suffer unexpected intraoperative cardiac arrest, which underscores the need for preparedness in all cases. Despite growing awareness and improved recognition of TC, predicting which patients are at risk of adverse outcomes remains a major clinical challenge. While most cases are transient and resolve with supportive care, a subset of patients develops severe complications such as cardiogenic shock, arrhythmias, or recurrence. At present, no universally accepted prognostic models exist to identify these high-risk individuals early in the disease course [1].
Recent research highlights the potential role of biomarkers and advanced imaging techniques in improving risk stratification. Elevated troponin and brain natriuretic peptide (BNP) levels have been associated with more severe left ventricular dysfunction, reflecting the degree of myocardial injury and stress. Inflammatory markers such as C-reactive protein (CRP) and leukocyte count may also provide insight into systemic responses linked to poorer outcomes. Equally promising are echocardiographic and electrocardiographic strain imaging modalities, which can detect subtle myocardial abnormalities not visible on standard imaging or ECG. Global longitudinal strain (GLS) on echocardiography, for example, may reveal persistent dysfunction even when left ventricular ejection fraction has normalized, guiding decisions on monitoring, pharmacotherapy, and patient counseling. The integration of biomarkers with advanced imaging parameters could eventually allow more accurate prognostication and individualized care pathways, although further prospective studies are needed to validate their utility across diverse populations and to establish standardized thresholds for clinical application [3].
This case reinforces the importance of considering TC in the differential diagnosis of perioperative cardiac arrest, particularly in patients without underlying coronary artery disease. Emotional stressors are classically implicated in approximately 27% of the cases of TC, physical triggers such as surgery and anesthesia accounted for 36%, combined physical and emotional triggers for 7.8%, and 28.5% had an unknown origin [4]. In addition, there are a few documented reports of the onset of TC during the perioperative period [5-8].
The underlying pathophysiology remains incompletely understood but is thought to involve catecholamine-mediated myocardial stunning. The condition has a marked female predominance, with approximately 90% of cases occurring in women [9]. In the perioperative setting, TC may manifest as acute heart failure, malignant arrhythmias, or cardiac arrest [10,11]. In patients without pre-existing cardiovascular disease, the diagnosis may only become apparent after intraoperative events, as in the present case [11].
The InterTAK diagnostic criteria provide the most widely accepted framework for establishing the diagnosis of TC. These include (1) transient left ventricular dysfunction-characterized by hypokinesia, akinesia, or dyskinesia-typically involving apical ballooning or midventricular, basal, or focal wall motion abnormalities; right ventricular involvement may also be observed; (2) the presence of an emotional, physical, or combined trigger, although not mandatory; (3) neurologic disorders or pheochromocytoma as potential precipitating factors; (4) new electrocardiographic abnormalities, such as ST-segment elevation or depression, T-wave inversion, and QTc prolongation, although rare cases may occur without ECG changes; (5) moderate elevation of cardiac biomarkers, including troponin and creatine kinase, with significantly elevated levels of BNP being common; (6) coexisting coronary artery disease that is not considered exclusionary; and (7) absence of evidence for infectious myocarditis [12].
Several conditions must be carefully excluded in the acute setting. Acute myocardial infarction is the most immediate consideration, but the absence of angiographic evidence of obstructive coronary lesions makes this unlikely. Acute myocarditis is another important differential, yet the lack of systemic inflammatory markers, the rapid clinical recovery, and the absence of necrosis or fibrosis on cardiac MRI argue against this diagnosis. Anesthetic-induced anaphylaxis warrants consideration, especially in the presence of drug allergy, but was excluded given the absence of cutaneous features, bronchospasm, or refractory hypotension requiring high-dose adrenergic support. The observed QTc prolongation and ventricular arrhythmias could raise suspicion for congenital or acquired long QT syndrome, but the transient nature of the findings and the absence of family history or exposure to QT-prolonging drugs favor a secondary phenomenon. Thyroid storm is also a relevant differential diagnosis in the perioperative context of thyroidectomy, as it can present with tachyarrhythmias, cardiovascular collapse, and fever; however, the absence of hyperpyrexia and abnormal thyroid function tests ruled it out in this case [12]. Electrolyte abnormalities were also excluded by arterial blood gas and serum chemistry results.
Postoperative care was undertaken in close collaboration with cardiology. Although no universally accepted therapy for TC exists, β-blockers and angiotensin-converting enzyme inhibitors are generally considered beneficial given the suspected role of catecholamine-mediated cardiotoxicity in the pathogenesis of the disease. The overall prognosis of TC is favorable, with more than 95% of patients achieving full recovery of left ventricular function [13-16].
Conclusions
This case is unique in that it documents the occurrence of TC precipitating a cardiac arrest during anesthetic induction in a previously healthy patient undergoing elective surgery-a rare and unexpected clinical scenario. While TC is increasingly recognized in various stress-related contexts, its manifestation at the critical juncture of anesthetic induction remains exceedingly uncommon and poses a significant diagnostic and therapeutic challenge. The absence of pre-existing cardiac pathology in this patient further underscores the unpredictability and potential severity of TC in the perioperative setting. The case emphasizes the importance of early recognition and prompt intervention when TC occurs during anesthetic induction. The physiological stressors associated with induction, including sympathetic activation, hemodynamic shifts, and exposure to anesthetic agents, may act as powerful triggers in susceptible individuals, even in the absence of identifiable risk factors.
It also underscores the need for anesthesiologists and perioperative teams to maintain a high index of suspicion for atypical cardiac events such as TC, particularly when the clinical course deviates from expectations. Early diagnosis and a rapid, coordinated response by a multidisciplinary team comprising anesthesia, cardiology, and intensive care specialists are crucial for improving outcomes and minimizing complications. This report contributes to the limited body of literature describing TC during anesthetic induction and reinforces the need for vigilance, preparedness, and interdisciplinary collaboration in managing unexpected cardiac events in the perioperative period. In the present case, the constellation of reversible apical akinesia, troponin elevation, transient ECG changes, and absence of obstructive coronary artery disease was most consistent with TC triggered by anesthetic induction. Alternative diagnoses-including acute coronary occlusion, myocarditis, anaphylaxis, and thyroid storm-were carefully evaluated and systematically excluded. The operative context justified a comprehensive diagnostic workup with coronary angiography, cardiac MRI, arterial blood gas and serum chemistry results, and immunoallergology assessment, all of which supported conservative management with supportive care, β-blockade, and close monitoring, ultimately leading to a favorable outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cardiac arrest in the perioperative period: a consensus guideline for identification, treatment, and prevention from the European Society of Anaesthesiology and Intensive Care and the European Society for Trauma and Emergency Surgery Eur J Trauma Emerg Surg Hinkelbein J Andres J Böttiger BW 203120464920233743017410.1007/s 00068-023-02271-3PMC 10520188 · doi ↗ · pubmed ↗
- 2Takotsubo cardiomyopathy (broken-heart syndrome): a short review S D Med Potu KC Raizada A Gedela M Stys A 169171692016 https://pubmed.ncbi.nlm.nih.gov/27263165/27263165 · pubmed ↗
- 3LAD electromechanical mismatch index: comparative analysis of EKG and left ventricular strain in stress cardiomyopathy and LAD-territory STEMIJACC Borkowski P Hanif W Torrado J 2053852025
- 4Clinical features and outcomes of Takotsubo (stress) cardiomyopathy N Engl J Med Templin C Ghadri JR Diekmann J 92993837320152633254710.1056/NEJ Moa 1406761 · doi ↗ · pubmed ↗
- 5A case of undiagnosed ‘Takotsubo’ cardiomyopathy during anesthesia (Article in Japanese)Masui Takigawa T Tokioka H Chikai T Fukushima T Ishizu T Kosogabe Y 11041106522003 https://pubmed.ncbi.nlm.nih.gov/14598678/14598678 · pubmed ↗
- 6Takotsubo cardiomyopathy following cholecystectomy: a poorly recognized cause of acute reversible left ventricular dysfunction Int J Cardiol Jensen JB Malouf JF 39039110620061633704810.1016/j.ijcard.2004.11.040 · doi ↗ · pubmed ↗
- 7Takotsubo cardiomyopathy after general anesthesia for eye surgery Anesthesiology Gavish D Rozenman Y Hafner R Bartov E Ezri T 62162310520061693199810.1097/00000542-200609000-00029 · doi ↗ · pubmed ↗
- 8Takotsubo syndrome during induction of general anaesthesia Anaesthesia Jabaudon M Bonnin M Bolandard F Chanseaume S Dauphin C Bazin JE 5195236220071744806710.1111/j.1365-2044.2007.05061.x · doi ↗ · pubmed ↗