Rare Cutaneous Metastasis of Low-Grade Retroperitoneal Leiomyosarcoma
Kostandin Valle, Divya Pothuri, Sean Pirrone, Jordan Parker

TL;DR
This paper reports the first case of a low-grade retroperitoneal leiomyosarcoma metastasizing to the skin, challenging the assumption that low-grade tumors are less aggressive.
Contribution
The first documented case of cutaneous metastasis from a low-grade retroperitoneal leiomyosarcoma.
Findings
A low-grade retroperitoneal leiomyosarcoma metastasized to the skin in a patient 18 months after initial diagnosis.
Two cutaneous lesions showed identical histological features to the original tumor and were successfully excised.
No systemic metastasis was detected on follow-up PET scan, but a third lesion later developed on the patient's cheek.
Abstract
Retroperitoneal leiomyosarcoma (RPL) is a rare smooth muscle malignancy that often presents silently and is typically diagnosed at an advanced stage. Cutaneous metastases from RPL are uncommon and usually indicate high-grade disease with a poor prognosis. To date, there are no published reports of low-grade RPL metastasizing to the skin. We report the case of a 55-year-old female who initially presented with intermittent abdominal pain and was diagnosed with a 5.1 x 3.1 cm retroperitoneal mass. Following surgical resection, histopathologic examination confirmed low-grade leiomyosarcoma based on spindle cell morphology and low mitotic activity. The patient recovered well postoperatively, but 18 months later, she presented to dermatology with a firm, dusky, subcutaneous nodule on her right temporal hairline. A punch biopsy confirmed cutaneous metastasis of leiomyosarcoma. A subsequent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1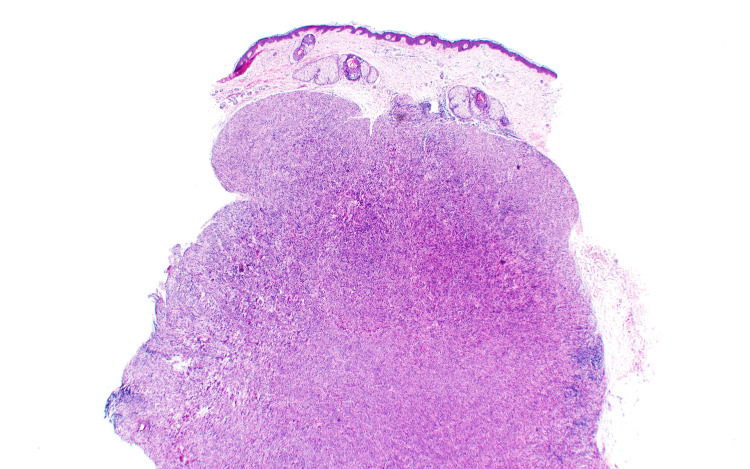 Figure 2
Figure 2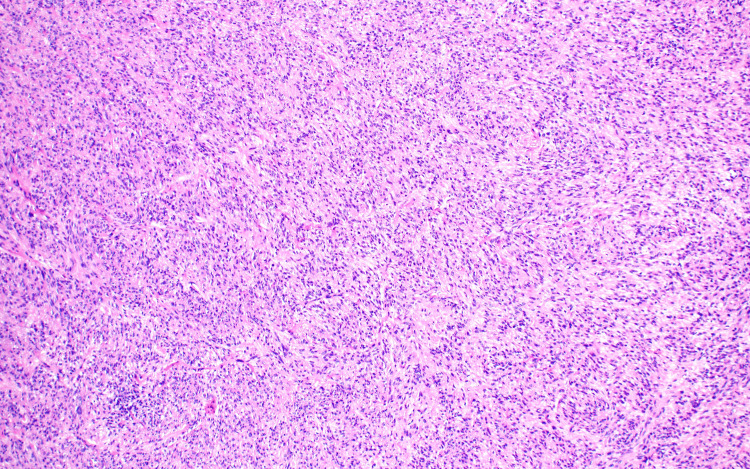 Figure 3
Figure 3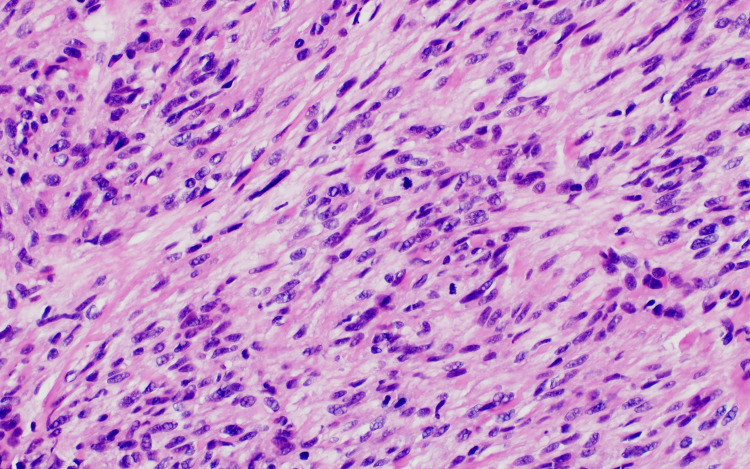 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Cancer Diagnosis and Treatment · CAR-T cell therapy research
Introduction
Retroperitoneal leiomyosarcoma (RPL) is a rare, malignant tumor that arises from smooth muscle cells within the retroperitoneal space [1]. Due to their location, most of these tumors can grow to significant sizes while remaining clinically silent. RPLs are frequently diagnosed as high-grade tumors with a poor prognosis [1]. Diagnostic measures for RPL include computed tomography (CT) scans or magnetic resonance imaging (MRI), but confirmation of the diagnosis requires a core needle biopsy [2]. Histopathologic examination is necessary to grade the tumor. The distinction between high-grade and low-grade tumors is determined based on the number of mitotic figures per 10 high-power fields (HPF). Greater than 10 mitotic figures per 10 HPF is deemed a high-grade tumor, and less than 10 mitotic figures per 10 HPF is considered a low-grade tumor [3]. When treatment is pursued, the gold standard remains en bloc resection of the mass, often requiring resection of surrounding tissue as well [4,5]. Various studies have additionally examined the use of radiation therapy in addition to surgical resection, either preoperative, postoperative, or intraoperative, but no clinical trials have demonstrated prospective efficacy [2].
Primary cutaneous leiomyosarcomas have been recognized in the literature, often signaling a better prognosis for patients [2,6]. These are divided into dermal or subcutaneous subtypes depending on the layer of origin. In contrast, cutaneous metastasis of RPL typically signifies a high-grade tumor and favors a worse prognosis [6]. A thorough review of the literature revealed no published case reports to date of low-grade RPL metastasizing to the skin. Histopathologic evaluation of cutaneous leiomyosarcomas is congruent with increased mitotic activity and spindle-shaped cells arranged in fascicles. Immunohistochemical staining can help further confirm the diagnosis and includes stains for desmin, vimentin, smooth muscle actin, or other muscle markers [4]. The clinical presentation of cutaneous leiomyosarcoma can be variable, but often includes a novel and evolving firm nodular lesion with pigmentary changes and tenderness to palpation [4]. Here, we present a case of this phenomenon in a 55-year-old female patient.
Case presentation
The patient first presented to the emergency department with intermittent abdominal pain in January 2023. A CT scan of the abdomen and pelvis at that time identified a right upper quadrant mass. Malignancy was suspected, and the patient was referred to surgical oncology. Surgical oncology ordered further imaging, including a repeat CT scan and an MRI. These confirmed a 5.1×3.1 cm mass adjacent to the patient's liver, which was causing a mass effect on her inferior vena cava, right adrenal gland, and liver. An exploratory laparotomy was performed in March 2023 with excision of the retroperitoneal tumor and right adrenal gland, as well as segmental resection of the suprarenal vena cava with a Dacron interposition graft. Surgical pathology reported the presence of hyperchromatic spindle-to-oval nuclei, moderate eosinophilic to clear cytoplasm, and indistinct cell borders arranged in fascicles with scattered lymphoid aggregates. There were up to seven mitotic figures per 10 HPF, and a Ki-67 demonstrated a 7% proliferative rate, both indicating low levels of cell division. As such, the tumor cells exhibited a low degree of atypia. Immunohistochemical stain was positive for desmin, caldesmon, and smooth muscle actin. This, coupled with a low degree of atypia, led to a histological diagnosis of low-grade leiomyosarcoma. The patient recovered well from the procedure and experienced no recurrence of abdominal symptoms.
In November 2024, the patient presented to the dermatology clinic due to concerns of a skin lesion that had been present for an indeterminate amount of time, but was evolving. The lesion was a 1.1 cm firm, subcutaneous, slightly dusky nodule with central darkening located in the right temporal hairline, associated with pruritus and irritation (Figure 1).
Gross clinical findings Firm, skin-colored subcutaneous nodule located on the right temple.
Due to the patient's history and inconclusive presentation, a 5 mm punch biopsy was performed at this time and sent to pathology for evaluation using hematoxylin and eosin (H&E) (Figure 2). Histopathology showed proliferation composed of fascicles of spindled cells with blunt-ended nuclei, alongside neoplastic cells with hyperchromatic nuclei and scattered mitotic figures (Figures 3, 4).
Low-power H&E stain image of the patient's metastatic lesionA punch biopsy consists of neoplastic cells with scattered lymphoid aggregates.H&E: hematoxylin and eosin
Medium power H&E stain image of the patient's metastatic lesionNeoplastic cells exhibit abundant eosinophilic activity, which helps to clear cytoplasm and lymphoid aggregates.H&E: hematoxylin and eosin
High-power H&E stain image of the patient's metastatic lesionNeoplastic proliferation composed of fascicles of spindled cells with blunt-ended, hyperchromatic nuclei and scattered mitotic figures.H&E: hematoxylin and eosin
The histopathological findings, confirmed by positive immunohistochemical staining for smooth muscle actin, led to a diagnosis of metastatic low-grade leiomyosarcoma. At her follow-up appointment 11 days later, the patient endorsed an additional 0.3 cm mobile subcutaneous nodular lesion in the right antecubital fossa. A 4 mm punch excision of the lesion was performed and sent to pathology, which confirmed it to be metastatic low-grade leiomyosarcoma, with identical histologic features as the first cutaneous specimen. The patient underwent excision of both cutaneous nodules, and a follow-up PET scan by oncology revealed no sign of further metastatic disease. A watchful waiting approach was recommended, as low-grade leiomyosarcoma responds poorly to systemic therapy.
At her most recent visit to the dermatology clinic in May 2025, the patient endorsed a new lesion on her right cheek. Physical examination revealed a 1 cm firm subcutaneous nodule overlying the right masseter. Due to concerns about deep connections to underlying structures, the procedure was deferred at this time, and the patient elected to follow up with oncology for further imaging.
Discussion
RPLs are generally associated with a poor prognosis due to their aggressive nature and ability to metastasize. While the literature supports metastatic disease in high-grade RPL, we present a novel case highlighting cutaneous metastatic disease in a low-grade RPL, thereby challenging established paradigms. Although low-grade RPLs are typically prognostically favorable, the presence of metastasis, even from a low-grade primary, is associated with a significantly increased risk of mortality [7]. Factors that may contribute to metastasis in these low-grade tumors include their location, as in this patient, whose tumor caused mass effect on her inferior vena cava, with which direct contact could have provided a rapid way for the tumor to disseminate despite its low histologic grade. Furthermore, the gross size of the lesion may be linked to its aggressive behavior and metastatic ability, despite its low histologic grade. Other factors may include common genetic mutations observed in leiomyosarcomas, among them being PTEN, RB1, and TP53 [8]. With all of these other potential factors in mind, we urge clinicians to carefully consider the prognostic significance of low histologic grade in such tumors. Additionally, for patients who undergo surgical resection, as in this case, the most significant predictors for mortality include tumor size, tumor location, and mitotic rate [9].
In any case, close multidisciplinary follow-up is vital to the overall health and well-being of these patients. The healthcare team must work together to manage these complex cases and should include, but not be limited to, surgery, oncology, dermatology, and mental health resources. For isolated cutaneous metastasis, surgical excision is preferred in addition to palliative care. For widespread metastatic lesions, systemic therapy combining doxorubicin with either dacarbazine or ifosfamide remains first-line. However, other systemic agents have been noted in the literature, including but not limited to methotrexate, trabectedin, and olaratumab [10,11]. However, it is important to note that systemic options are limited and their efficacy is not well supported in low-grade leiomyosarcoma. Ultimately, in patients with a history of low-grade RPL presenting with new-onset skin lesions, it is imperative to maintain a high index of suspicion for metastatic disease to provide appropriate and effective care.
Conclusions
Cutaneous metastasis of RPL is a recognized phenomenon in the literature; however, these metastases are typically high-grade, aggressive tumors. In contrast, we present a novel case of low-grade primary RPL metastasizing to the skin. Clinical findings were non-specific, but histopathologic examination revealed characteristic findings of a low-grade leiomyosarcoma with fewer than seven mitotic figures per 10 HPF and a Ki-67 index of 7%. En bloc resection remains the mainstay of therapy for RPL, with surgical excision preferred for cutaneous metastases. Adjuvant chemotherapeutic agents and radiation have been discussed in the literature, but no conclusive evidence has been found to support their use. We emphasize that low-grade differentiation should not preclude clinicians from being suspicious of metastatic disease in patients with RPL. Thus, multidisciplinary follow-up and ongoing vigilance are crucial for a thorough workup of metastasis in patients with low-grade RPL and the development of new skin lesions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giant retroperitoneal leiomyosarcoma: a case report J Surg Case Rep Hermi A Boussaffa H Saadi A Bel Hadj Kacem L Chakroun M Slama RB 2023202310.1093/jscr/rjad 172PMC 1009755237064072 · doi ↗ · pubmed ↗
- 2Soft-tissue sarcoma Gunderson & Tepper’s Clinical Radiation Oncology Alektiar KM 13591385 Philadelphia, PA Elsevier 752021 https://www-clinicalkey-com.proxy.mul.missouri.edu/#!/content/book/3-s 2.0-B 978032367246700075 X?scroll To=%233-s 2.0-B 978032367246700075 X-f 075-016-9780323672467
- 3Prognostic value of mitotic count in leiomyosarcoma: a comprehensive monocentric retrospective study Hum Pathol Grimaudo MS Renne SL Colombo P 172314320243800068210.1016/j.humpath.2023.11.009 · doi ↗ · pubmed ↗
- 4First and further-line multidisciplinary treatment of retroperitoneal sarcomas Curr Opin Oncol D'Ambrosio L Van Houdt W Stelmes JJ Gronchi A 3283343420223583770410.1097/CCO.0000000000000851 · doi ↗ · pubmed ↗
- 5Histology-based classification predicts pattern of recurrence and improves risk stratification in primary retroperitoneal sarcoma Ann Surg Tan MC Brennan MF Kuk D 59360026320162591591010.1097/SLA.0000000000001149 PMC 4619189 · doi ↗ · pubmed ↗
- 6Cutaneous leiomyosarcoma: a 20-year retrospective study and review of the literature An Bras Dermatol Soares Queirós C Filipe P Soares de Almeida L 2782839620213377548110.1016/j.abd.2020.10.003PMC 8178579 · doi ↗ · pubmed ↗
- 7Retroperitoneal leiomyomas. A clinicopathologic and immunohistochemical study of 56 cases with a comparison to retroperitoneal leiomyosarcomas Am J Surg Pathol Paal E Miettinen M 135513632520011168495110.1097/00000478-200111000-00002 · doi ↗ · pubmed ↗
- 8Targeting the molecular and immunologic features of leiomyosarcoma Cancers (Basel) Cope BM Traweek RS Lazcano R Keung EZ Lazar AJ Roland CL Nassif EF 15202310.3390/cancers 15072099 PMC 1009307837046760 · doi ↗ · pubmed ↗