Management of cerebral ventriculoatrial shunt during pulmonary endarterectomy
Matthew Aizpuru, Benjamin D. Elder, Philip J. Spencer, Sahar A. Saddoughi, Hector R. Cajigas, Mauricio A. Villavicencio

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
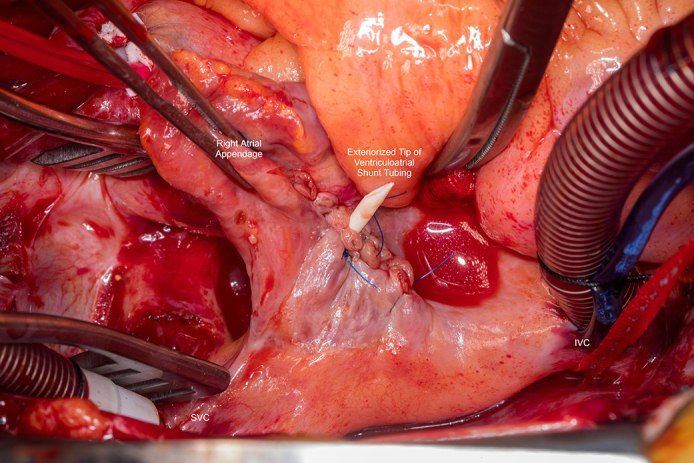 Figure 1
Figure 1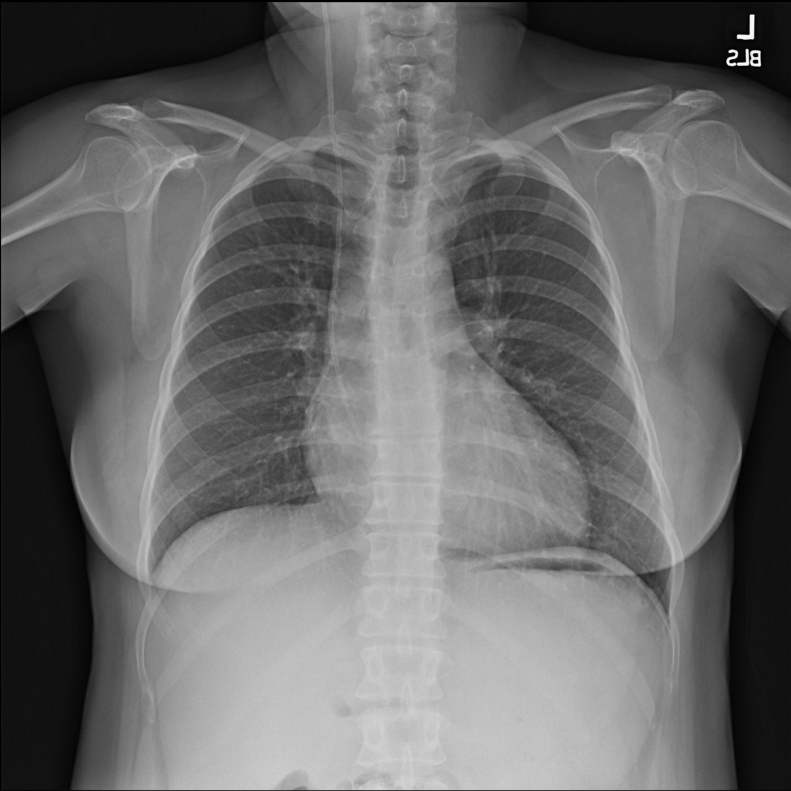 Figure 2
Figure 2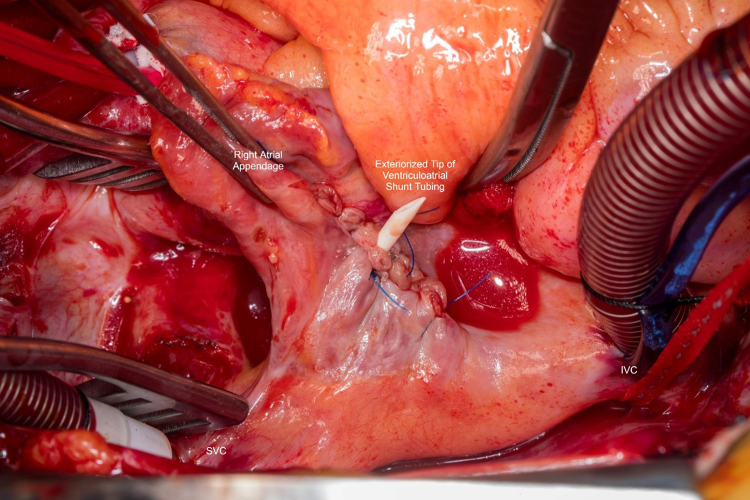 Figure 3
Figure 3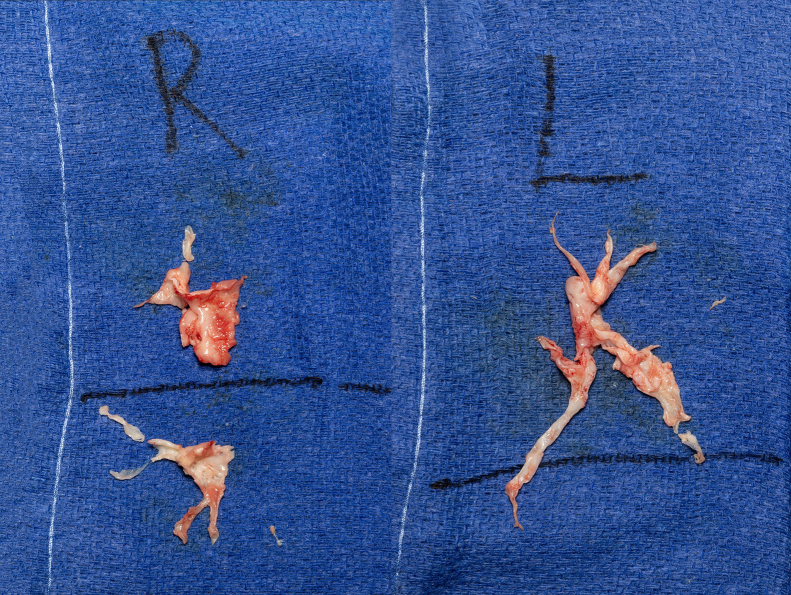 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurosurgical Procedures and Complications · Traumatic Brain Injury and Neurovascular Disturbances · Cerebrospinal fluid and hydrocephalus
Surgeon's view of the VA shunt tubing exteriorized through the right atrial free wall. Central MessageManagement of cerebral ventriculoatrial shunts during cardiopulmonary bypass requires careful planning. Here we describe our management of a VA shunt during pulmonary endarterectomy.
Case Report
Ventriculoatrial (VA) shunts are an option for management of hydrocephalus when the peritoneal cavity is not suitable. Previously reported complications associated with VA shunts include endocarditis, catheter fracture/migration, and intracardiac thrombosis.1^,^2 Optimal management of VA shunts during cardiopulmonary bypass is unclear. Here we describe our management of this complex situation with the express written consent of the patient; institutional review board approval was not required.
This is the case of a 40-year-old female patient with history of a VA shunt implanted in childhood, who presented with chronic thromboembolic pulmonary hypertension. Associations between chronic indwelling vascular devices and chronic thromboembolic pulmonary hypertension have been described.3 The patient underwent right heart catheterization, which revealed pulmonary arterial pressure of 62/25 (38) mm Hg, pulmonary vascular resistance of 18.6 WU, and a cardiac index of 1.71 L/min/m.^2^ The echocardiogram demonstrated moderate right ventricular dysfunction, and a chest radiograph revealed the VA shunt tip terminating in the right atrium (Figure 1). The VA shunt was a nonprogrammable, low-pressure, pressure-differential valve, originally placed in 1985. She has had multiple revisions of the distal atrial catheter, most recently in 1998. We were concerned that the negative distal pressure associated with vacuum-assist cardiopulmonary bypass would result in a significant pressure differential across the shunt system in the absence of an antisiphon device, and therefore severe overdrainage of cerebrospinal fluid (CSF) and neurologic consequences. We therefore planned for pulmonary endarterectomy with exteriorization of the shunt tip and drainage of CSF into the pericardial well while on cardiopulmonary bypass.Figure 1. Chest radiograph demonstrating ventriculoatrial shunt tubing terminating in the right atrium.
The patient was brought to the operating room, underwent median sternotomy, distal aortic arterial and bicaval venous cannulation with snares. After initiating cardiopulmonary bypass without vacuum-assist, the right atrium was opened and the shunt tip was exteriorized. The atriotomy was closed with 4-0 Prolene (Ethicon) around the shunt tubing, allowing for free flow of the CSF into the pericardial well (Figure 2). The pulmonary endarterectomy was then completed using vacuum-assist cardiopulmonary bypass and deep hypothermic circulatory arrest, 26 minutes on the right side and 16 on the left (Figure 3). The shunt tip was returned to the right atrium at completion of the case. Pulmonary artery pressures normalized in the operating room. The patient recovered well and was discharged from the hospital on the fifth postoperative day without any neurologic sequelae.Figure 2. Surgeon's view of the right atrium. The ventriculoarterial shunt tubing has been exteriorized through the free wall of the right atrium. SVC, Superior vena cava.Figure 3. Intraoperative specimen photographs. R, Right; L, left.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dziarmaga M.Puslecki M.Stefaniak S.Right atrial mass of unclear origin in patient with ventriculoatrial shunt Kardiol Pol 821020241017101810.33963/v.phj.10180539140663 · doi ↗ · pubmed ↗
- 2Passey S.Tidwell J.Soares Pinho De Carvalho L.M.Zeman J.Kim A.S.Infective endocarditis as a complication of a ventriculoatrial shunt JACC Case Rep 303202510309710.1016/j.jaccas.2024.103097 PMC 1183024239963232 · doi ↗ · pubmed ↗
- 3Yang J.Madani M.M.Mahmud E.Kim N.H.Evaluation and management of chronic thromboembolic pulmonary hypertension Chest 1642202349050210.1016/j.chest.2023.03.02936990148 PMC 10410247 · doi ↗ · pubmed ↗