Surgical repair for left ventricular apical aneurysm without coronary artery disease
Satoshi Numata, Tomohito Nakashima, Tatsuro Gondai, Takuma Kobayashi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
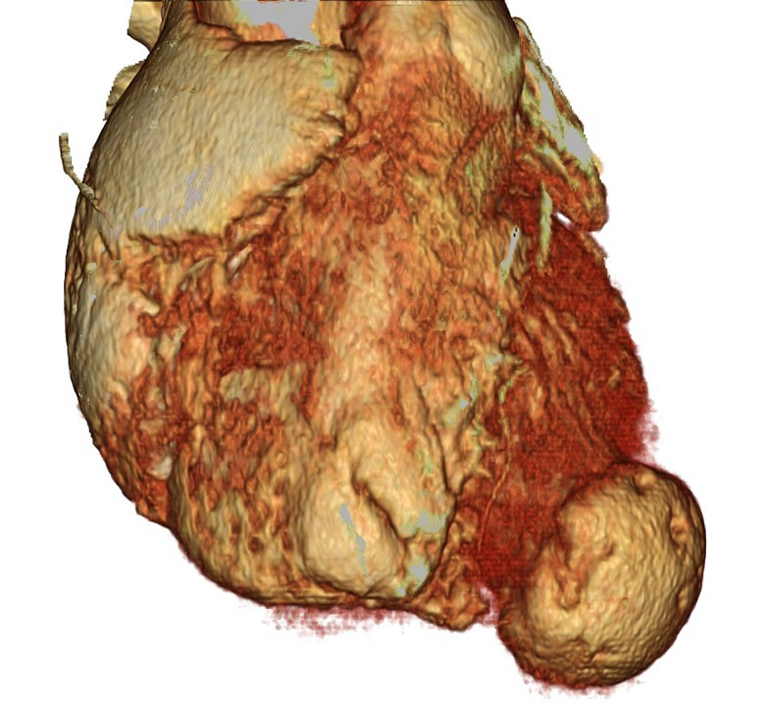 Figure 1
Figure 1 Figure 2
Figure 2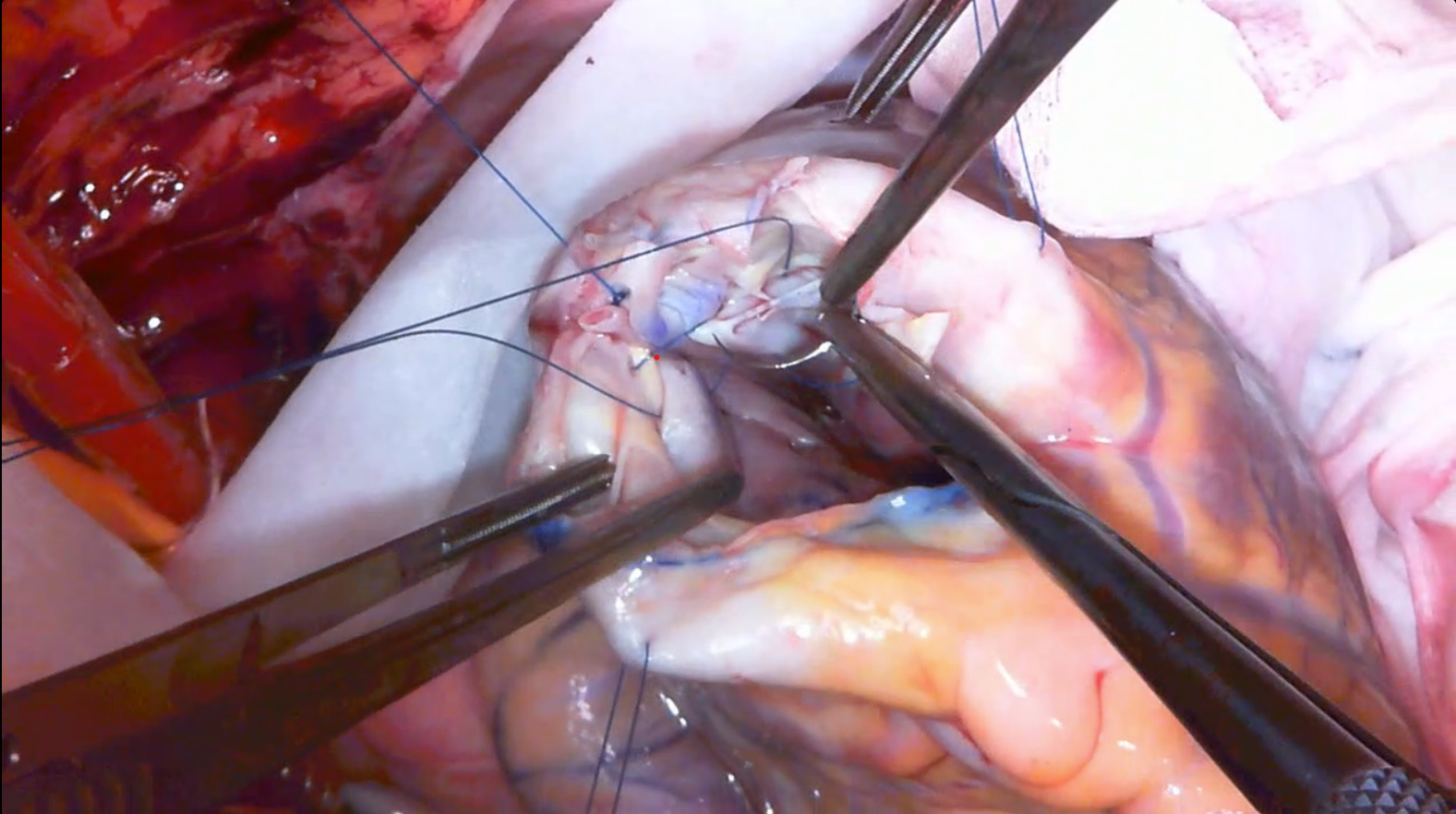 Figure 3
Figure 3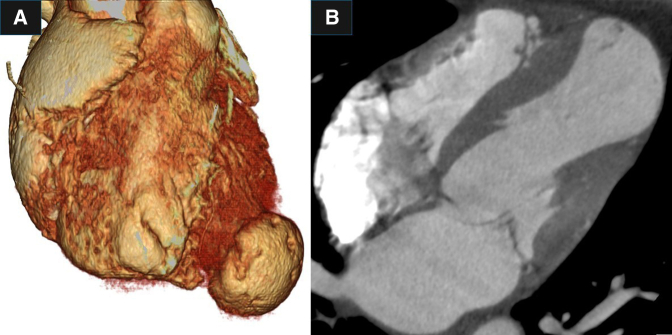 Figure 4
Figure 4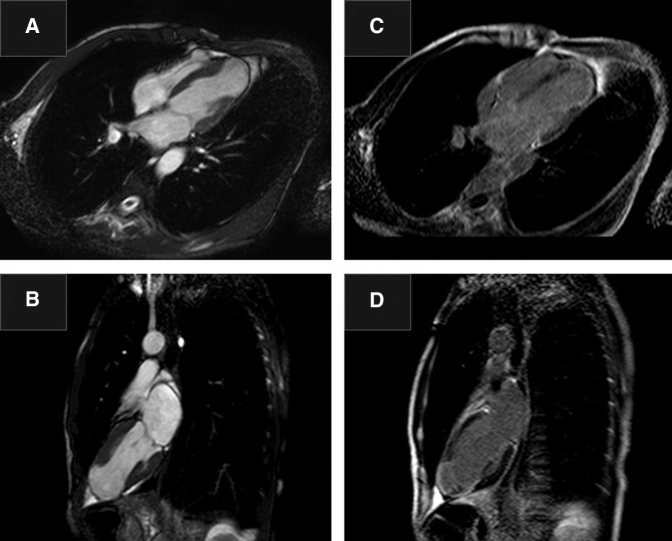 Figure 5
Figure 5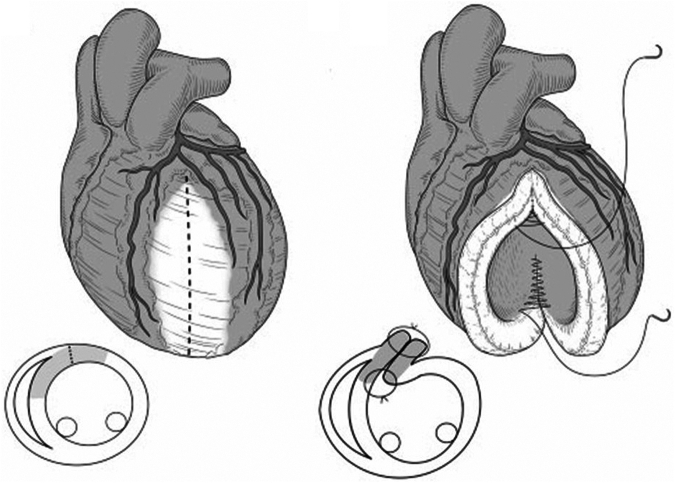 Figure 6
Figure 6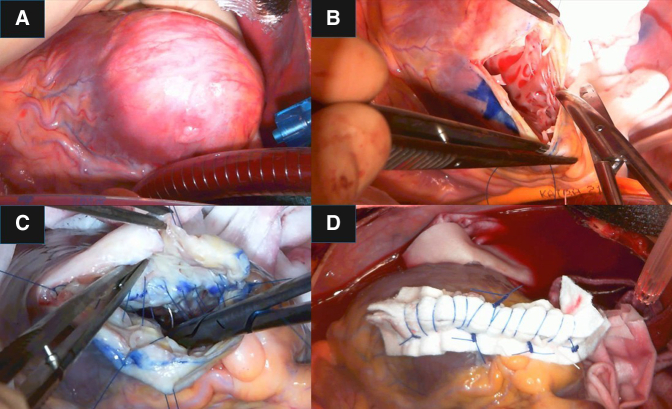 Figure 7
Figure 7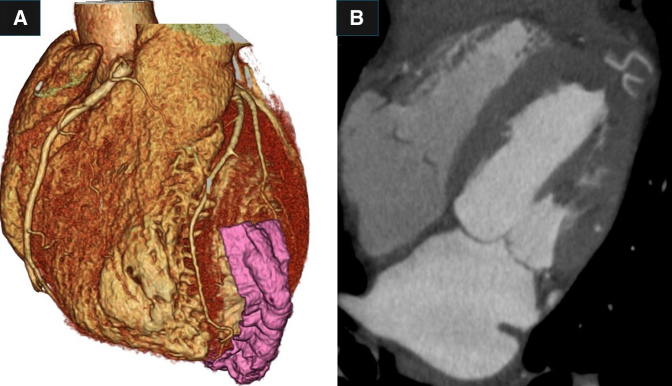 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac Valve Diseases and Treatments · Pericarditis and Cardiac Tamponade
Left ventricular apical aneurysm without coronary artery disease. Central MessageFor repairing left ventricular aneurysm without coronary artery disease, left ventricular restoration procedure ELIET (endocardial linear infarct exclusion technique) is one useful option.
The most common cause of left ventricular aneurysm is coronary artery disease, but it also can occur due to trauma, sarcoidosis, and other factors. Here we report a case of surgical treatment of a left ventricular aneurysm located at the apex without significant coronary artery stenosis.
Case Report
A 52-year-old man was diagnosed with a left ventricular apical aneurysm following abnormal findings on chest X-ray. He did not complain of chest pain or shortness of breath on exertion. Twenty years ago, chest X-ray led to suspicion of sarcoidosis, but no further investigation was done, and no medication was administered. He did not have a history of chest trauma. His medical history included ulcerative colitis and type I diabetes. Electrocardiography showed a normal sinus rhythm with premature ventricular contraction, and coronary angiography revealed no significant stenosis. A computed tomography (CT) scan showed a left ventricular apical aneurysm (Figure 1, Video 1) without mural thrombus. Delayed-enhancement magnetic resonance imaging demonstrated a thin, transmurally enhanced aneurysmal wall (Figure 2). Serum blood tests did not indicate any inflammatory disease, such as sarcoidosis.Figure 1A, Three-dimensional reconstruction of preoperative computed tomography scan. B, Thin-slice image of preoperative computed tomography scan.Figure 2A, and B, Cardiac magnetic resonance imaging. C, and D, Delayed enhanced images.
The patient underwent ventricular repair with our endocardial linear infarct exclusion technique (ELIET)1 and cryoablation of the ventricular wall (Figure 3). After transmural linear ventriculotomy at the center of the aneurysm, cryoablation was performed between the aneurysmal wall and intact myocardium (−60°C for 2 minutes). Then the inner layer was sutured longitudinally with continuous sutures to the border between the aneurysmal wall and intact myocardium. The outer layer was closed using double layers.Figure 3. Schema of the endocardial linear infarct exclusion technique (ELIET) procedure.
Intraoperatively, the aneurysmal wall was seen to be very thin, almost like tanned leather (Figure 4, Video 2). Histopathology showed that the aneurysm wall contained only fibrous tissue without myocardium and with no multinucleated giant cells.Figure 4A, Intraoperative findings. B, Longitudinal incision of the aneurysm. C, Linear running suture of the inner layer between the infarcted wall and intact myocardium. D, Closure of the outer layer.
The patient's postoperative course was uneventful. A CT scan showed a repaired ventricular wall. The left ventricular systolic volume index was decreased from 76.2 mL/m^2^ to 49.7 mL/m^2^, and the ejection fraction was improved from 36% to 41% (Figure 5).Figure 5A, Three-dimensional reconstruction of postoperative computed tomography scan. B, Thin-slice image of postoperative computed tomography scan.
Discussion
The cause of this patient's ventricular aneurysm remains unknown. In this case, there may have been a period of active inflammatory disease, such as sarcoidosis, in the past. It is known that sarcoidosis can be associated with cardiac lesions, which may resemble dilated cardiomyopathy and in some cases form left ventricular aneurysms.2 Lesions of cardiac sarcoidosis often occur in a patchy manner, and many of the nodules also appear in various parts of the left ventricle. The surgical indication for left ventricular aneurysm remains under debate.3 Treating the left ventricular aneurysm can improve LVEF, which may benefit for long-term survival. If the surgical risk is not high and the surgical procedure is expected to be reliable, we argue that surgical treatment can be considered even if the patient is asymptomatic. Additionally, with the coexistence of ulcerative colitis, it is preferable to avoid administering warfarin.
The surgical repair of ventricular aneurysms associated with sarcoidosis has been reported previously.4^,^5 Most approaches involve the use of a circular patch. In the present case, we used repaired using our method of left ventricular restoration, ELIET.1 The advantages are low bleeding risk, reproducibility, and coronary artery preservation. This technique can be applied not only to the anterior wall, but also to the lateral or posterior wall. As demonstrated in this case, the shape of the left ventricle improved, the risk of rupture was avoided, and the risk of left ventricular thrombus formation also decreased. Additionally, postoperative ventricular arrhythmias were no longer observed. The ELIET procedure is a useful option for left ventricular apical aneurysm without coronary artery disease.
Conclusions
The ELIET procedure has proven effective for left ventricular aneurysms not associated with coronary artery disease.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ohira S.Yamazaki S.Numata S.Ten-year experience of endocardial linear infarct exclusion technique for ischaemic cardiomyopathy Eur J Cardiothorac Surg 53220184404472902903410.1093/ejcts/ezx 343 · doi ↗ · pubmed ↗
- 2Iannuzzi M.C.Rybicki B.A.Teirstein A.S.Sarcoidosis New Engl J Med 357212007215321651803276510.1056/NEJ Mra 071714 · doi ↗ · pubmed ↗
- 3Hulten E.A.Blankstein R.Pseudoaneurysm of the heart Circulation 125152012192019252250884110.1161/CIRCULATIONAHA.111.043984 · doi ↗ · pubmed ↗
- 4Shimamoto T.Nishina T.Marui A.Dual left ventricular restorations in a patient with cardiac sarcoidosis J Thorac Cardiovasc Surg 13752009128612881938001110.1016/j.jtcvs.2008.04.007 · doi ↗ · pubmed ↗
- 5Miyahara S.Mukohara N.Morimoto N.Left ventricular restoration for cardiac sarcoidosis: report of two cases Surg Today 44320145685712327166610.1007/s 00595-012-0409-0 · doi ↗ · pubmed ↗