Coronary artery bypass grafting after deep inferior epigastric perforator flap breast reconstruction: A case report
AlleaBelle Bradshaw, Jessica B. Briscoe, Jace C. Bradshaw, Jennifer S. Lawton

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
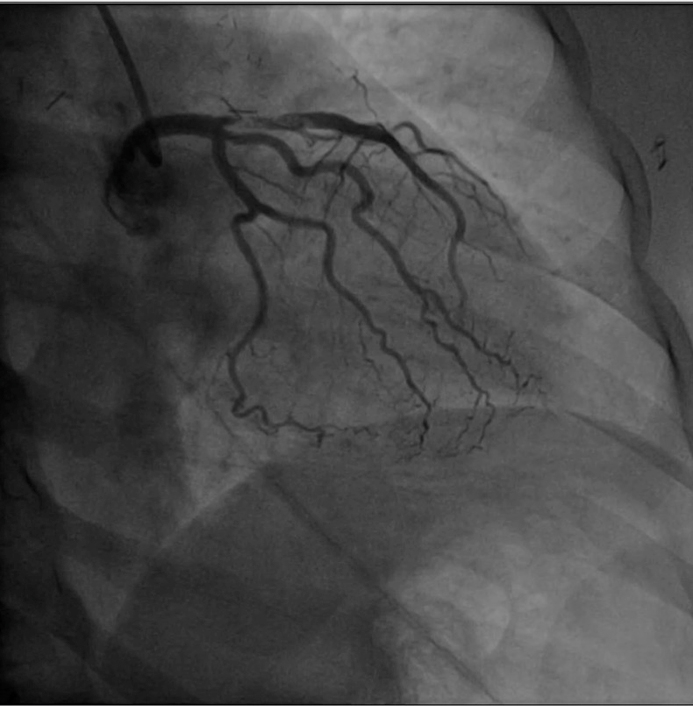 Figure 1
Figure 1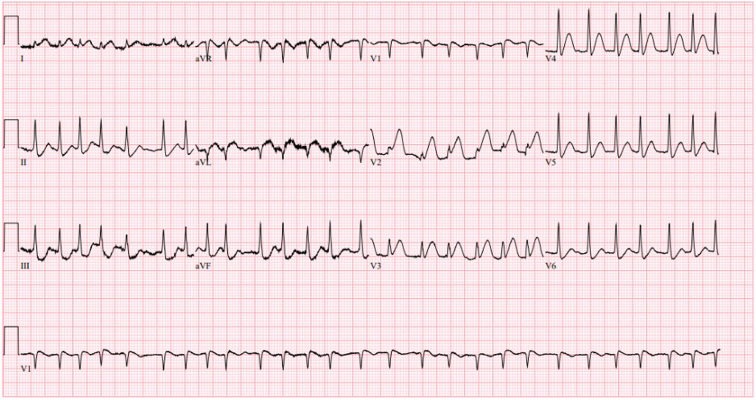 Figure 2
Figure 2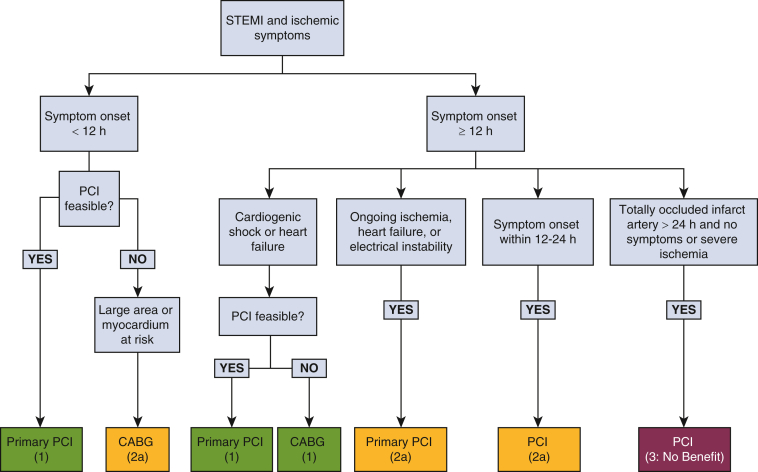 Figure 3
Figure 3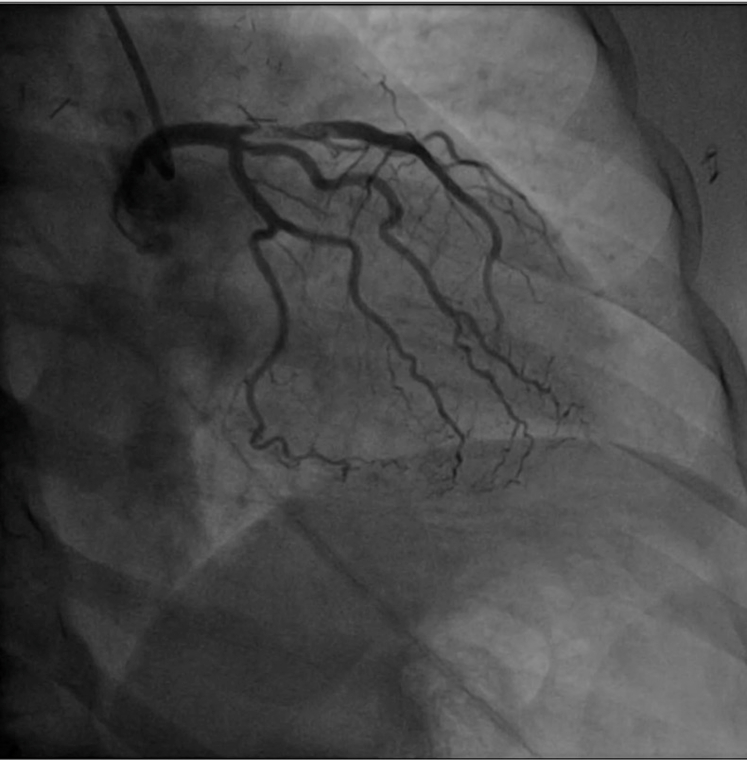 Figure 4
Figure 4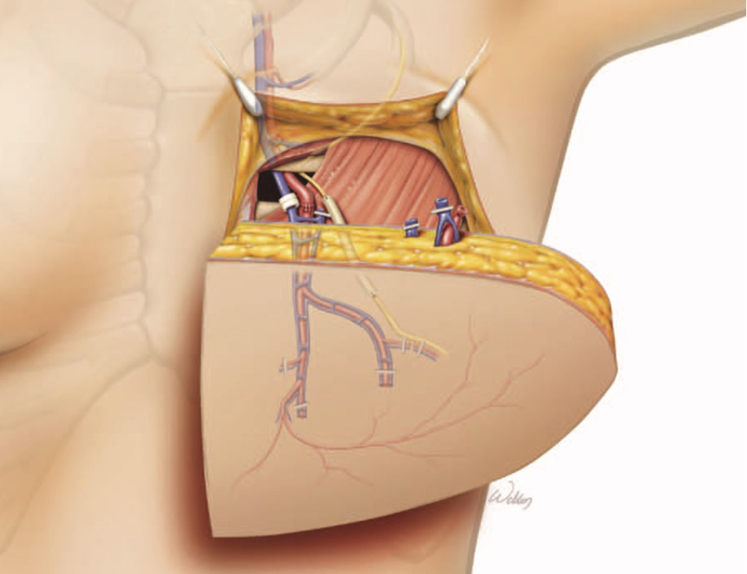 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac and Coronary Surgery Techniques · Cardiac, Anesthesia and Surgical Outcomes · Reconstructive Surgery and Microvascular Techniques
Coronary catheterization after cardiac arrest and resuscitation. Central MessageFamiliarity with deep inferior epigastric perforator (DIEP) flap reconstructions helps facilitate optimal coronary revascularization.
Conduit selection in a patient with a ST-segment elevation myocardial infarction (STEMI) who requires emergent coronary artery bypass grafting (CABG) is challenging when the patient has had previous breast reconstruction. Women in the United States undergo approximately 75,000 CABGs1^,^2 and 33,000 autologous breast reconstructions3 annually. These numbers indicate that a significant and increasing number of women will require both procedures, although data are needed that explore the combined incidence. This case highlights the need for surgeon awareness of breast-reconstruction strategies that eliminate the internal mammary artery (IMA) as a potential conduit. Institutional review board approval was not required; the patient provided informed consent for publication.
Case Report
A 51-year-old woman had sudden-onset chest pain. She had a history of breast cancer that was treated with chemotherapy and bilateral mastectomy with deep inferior epigastric perforator (DIEP) flaps.
In the emergency department, she had ongoing chest pain and experienced cardiac arrest attributable to ventricular fibrillation. She was defibrillated twice, with return of spontaneous circulation occurring. Findings on electrocardiogram after return of spontaneous circulation showed atrial fibrillation with rapid ventricular response and ST-segment elevation in V1-4 (Figure E1). Ticagrelor was administered before the patient was taken for left heart catheterization. She required norepinephrine (0.01-0.08 μg/kg/min) during the procedure. Angiography demonstrated left anterior descending (LAD) artery disease with proximal thrombus and Thrombolysis in Myocardial Infarction grade 2 flow (Figure 1). A ventriculogram showed minimal apical motion. Because of its proximity to the left circumflex ostium, retrieval of the clot from the LAD would risk lethal embolization down the left circumflex and LAD. Clot retrieval was aborted, an intra-aortic balloon pump was placed, and cardiac surgery was consulted.Figure 1. Coronary catheterization after arrest and resuscitation. Postarrest catheterization showing proximal left anterior descending artery disease with thrombus.
The patient was transferred from the catheterization laboratory to the operating room for emergent CABG. Preoperative transesophageal echocardiography demonstrated an ejection fraction of 20% to 25%. During dissection of the left IMA, it was found to be scarred to the chest wall, and the vessel was clipped distally. The clips were from previous breast-reconstruction surgery, so its use was abandoned. The right IMA was also assumed to be unusable, and using a radial artery would have required increased time in this critically ill patient. There was also concern that she would require significant vasoactive support postoperatively, increasing the risk of vasospasm. Therefore, the saphenous vein was expeditiously harvested and used.
The patient had no complications postoperatively. Postoperative transthoracic echocardiography demonstrated an improved ejection fraction of 45% to 50%. Her DIEP flaps showed no signs of ischemia, and her sternotomy wound healed well. She was discharged home on postoperative day 7 on dual antiplatelet therapy. At follow-up, she was doing well with no signs or symptoms concerning for compromised graft patency or breast tissue perfusion.
Discussion
In patients who experience STEMI but cannot safely undergo percutaneous coronary intervention, urgent or emergent CABG is recommended (Figure E2).4^,^5 Only approximately 6.3% patients with STEMI require CABG during the initial admission, and the mortality risk can be as high as 13%.5 When deviation from normal care pathways is required and mortality risk is high, a Heart Team approach is recommended.E1
This case was further complicated by previous breast reconstruction in which both IMAs were used. In patients with significant LAD stenosis, the LIMA is the best choice for revascularization and is a Society of Thoracic Surgeons quality metric. Use of an IMA graft is contraindicated in patients with breast reconstruction with DIEP or free transverse rectus abdominis myocutaneous flaps, as these require arterial inflow and venous outflow via the internal mammary artery and vein, respectively (Figure 2).E2^,^E3 There are limited data on patients undergoing CABG after breast reconstruction, largely attributable to small case samples at single institutions.E4 However, this challenging scenario will increase as rates of complex breast-reconstruction procedures increase.E5 Addressing this increasingly relevant issue may involve alternative techniques or decision-making algorithms for plastic surgeons.E6 Strategies for cardiac surgeons encountering patients after DIEP flaps are discussed in Appendix E1.Figure 2DIEP flap reconstruction anatomy. The internal mammary vessels are brought through the second intercostal space in a DIEP flap. The mammary artery is thus not available for CABG. The distal mammary vessels are ligated or clipped during this reconstruction. Permission obtained (license 6047201466970, June 13, 2025).E3DIEP, Deep inferior epigastric perforator.
Cardiac surgeons should be familiar with anatomical aspects of breast reconstructions. Preoperative imaging of the IMAs in patients with previous breast reconstruction may help to prevent compromising blood supply to reconstructed breast tissue during CABG. Careful planning, including Heart Team discussions, is recommended for nonemergent cases.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Esmaeilzadeh S.Vinzant N.Ramakrishna H.Outcomes in women undergoing coronary artery bypass grafting: analysis of new data and operative trends J Cardiothorac Vasc Anesth 392202553253710.1053/j.jvca.2024.10.03139547868 · doi ↗ · pubmed ↗
- 2Tsao C.W.Aday A.W.Almarzooq Z.I.Heart disease and stroke statistics—2023 update: a report from the American Heart Association Circulation 14782023 E 93E 62110.1161/CIR.000000000000112336695182 PMC 12135016 · doi ↗ · pubmed ↗
- 3Hong S.E.Kang D.Navigating the pandemic: shifts in breast reconstruction trends and surgical decision-making in the United States J Clin Med 13142024416810.3390/jcm 1314416839064208 PMC 11278449 · doi ↗ · pubmed ↗
- 4Pi Y.Roe M.T.Holmes D.N.Utilization, characteristics, and in-hospital outcomes of coronary artery bypass grafting in patients with ST-segment-elevation myocardial infarction: results from the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network Registry-Get with the Guidelines Circ Cardiovasc Qual Outcomes 1082017 e 00349010.1161/CIRCOUTCOMES.116.00349028794118 · doi ↗ · pubmed ↗
- 5Darwazah A.K.Islim I.Hanbali B.Emergency coronary artery bypass surgery after failed percutaneous coronary intervention J Cardiovasc Surg 502009795800 https://proxy 1.library.jhu.edu/login?url=https://www.proquest.com/scholarly-journals/emergency-coronary-artery-bypass-surgery-after/docview/224400309/se-219935612 · pubmed ↗
- 6Lawton J.S.Tamis-Holland J.E.Bangalore S.2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol 7922022 e 21e 12910.1016/j.jacc.2021.09.00634895950 · doi ↗ · pubmed ↗
- 7Maher J.L.Mahabir R.C.Roehl K.R.Addressing the potential need for coronary artery bypass grafting after free tissue transfer for breast reconstruction: an algorithmic approach Ann Plast Surg 752201514014310.1097/SAP.000000000000007026165568 · doi ↗ · pubmed ↗
- 8Spiegel A.J.Menn Z.K.Eldor L.Kaufman Y.Lee Dellon A.Breast reinnervation: DIEP neurotization using the third anterior intercostal nerve Plast Reconstr Surg Glob Open 182013 e 7210.1097/GOX.000000000000000825289267 PMC 4186303 · doi ↗ · pubmed ↗