The Accuracy of Artificial Intelligence-Based Models Applied to 12-Lead Electrocardiograms for the Diagnosis of Acute Coronary Syndrome: A Systematic Review
Aly Fawzy, Aleena Malik, Juan Pablo Diaz-Martinez, Ani Orchanian-Cheff, Sameer Masood

TL;DR
This review assesses how well AI models can diagnose heart attacks using ECGs, finding high accuracy but also variability and transparency issues.
Contribution
The study systematically evaluates AI diagnostic accuracy for acute coronary syndrome using 12-lead ECGs and compares it to clinician performance.
Findings
AI models showed sensitivity ranging from 68% to 98% and specificity from 41% to 98% for diagnosing ACS.
AI outperformed clinicians in sensitivity and PPV but had lower NPV in most studies.
Only 3 out of 24 studies reported code availability, highlighting transparency challenges.
Abstract
This systematic review aims to evaluate the diagnostic accuracy of artificial intelligence (AI) algorithms in acute coronary syndrome (ACS) detection using 12-lead electrocardiograms (ECGs). Adhering to Preferred Reporting Items for Systematic Reviews guidelines, Ovid MEDLINE, Ovid Embase, Cochrane Central, and Cochrane Database of Systematic Reviews were searched up to June 15, 2023. Eligible studies involved adults with suspected ACS and employed AI for 12-lead ECG interpretation. The primary outcomes were sensitivity and specificity, with secondary outcomes including positive predictive value (PPV), negative predictive value (NPV), and accuracy. Risk of bias was evaluated using Prediction model Risk Of Bias Assessment Tool (PROBAST). From 2051 records, 24 studies were included. The sensitivity of AI-based diagnosis for ACS among the 24 studies varied from 68% to 98%, and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
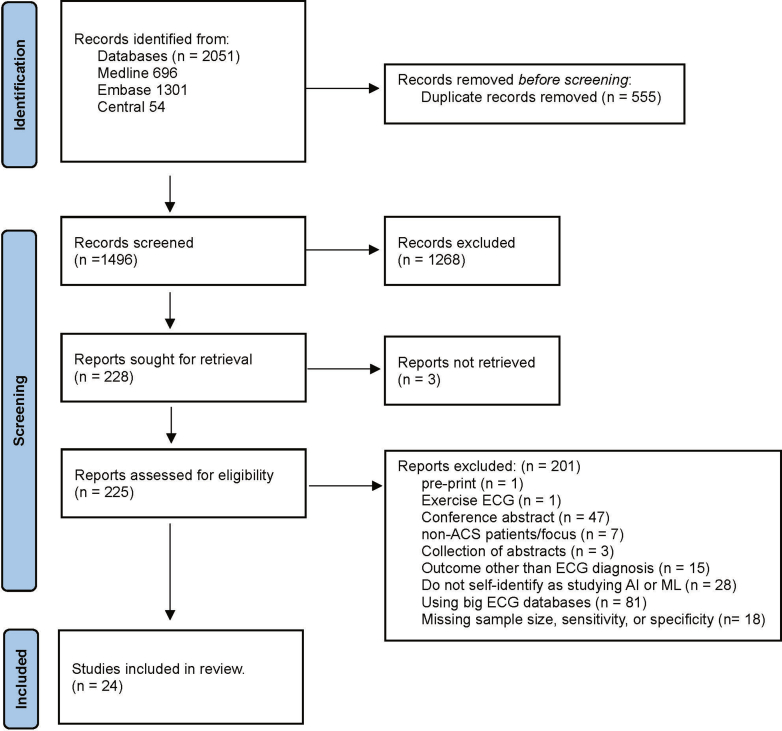 Figure 1
Figure 1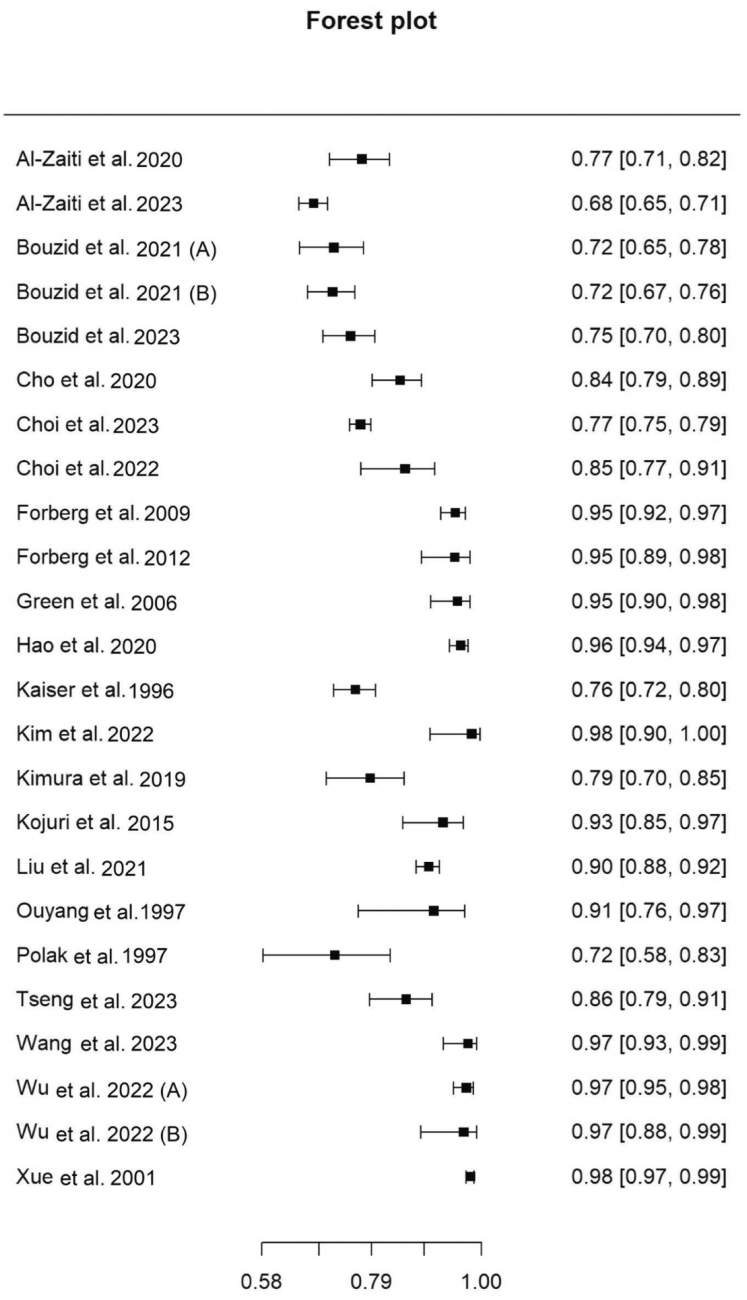 Figure 2
Figure 2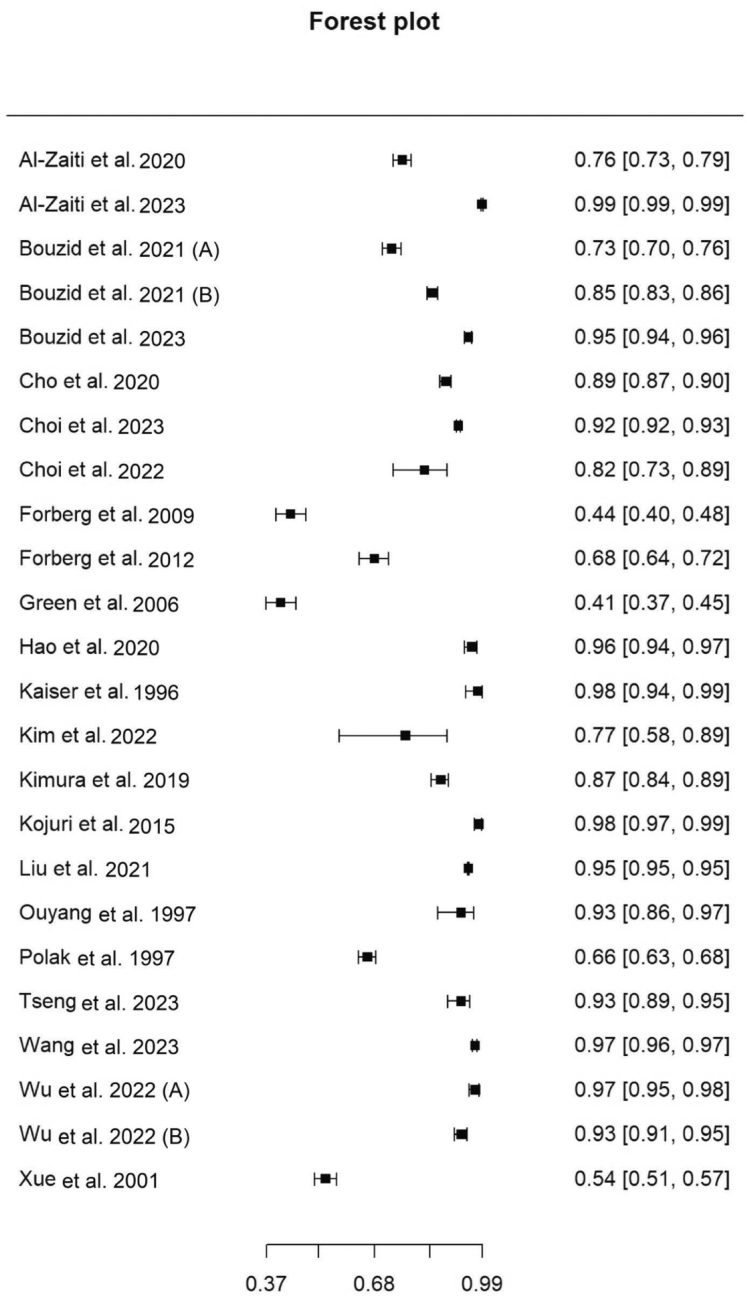 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsECG Monitoring and Analysis · Artificial Intelligence in Healthcare and Education · Artificial Intelligence in Healthcare
Introduction
1
Background
1.1
Artificial intelligence (AI) has been making significant strides in various domains, including healthcare. Its potential to revolutionize disease diagnosis, patient care, and health system management has been recognized globally.1 One of the areas in which AI has shown considerable promise is in the field of cardiology, particularly in the interpretation of 12-lead electrocardiograms (ECGs).2 ECG interpretation is a critical aspect in the diagnosis of acute coronary syndrome (ACS), and timely interpretation can impact the morbidity and mortality of patients with ACS.3
Importance
1.2
AI, particularly machine learning (ML) and deep learning (DL) algorithms, have been applied to ECG interpretation to facilitate ACS diagnosis.4 These AI techniques hold promise for enhancing the speed and accuracy of ECG interpretation and improving patient outcomes. Several studies have suggested that AI could potentially identify subtle patterns in ECG tracings that may not be easily recognized by physicians, enabling earlier detection of ACS and prompt initiation of treatment.4, 5, 6, 7, 8, 9, 10, 11
Despite these promising developments, the evidence base for AI’s effectiveness in this context is fragmented, and its real-world performance is yet to be systematically evaluated. A recent systematic review assessing the application of ML for the diagnosis of ACS using a 12-lead ECG suggested that AI algorithms tend to have better sensitivity in ECG interpretation.12 However, the review only included articles that had an AI performance comparator (ie, clinicians, software, or criteria).
Goals of This Investigation
1.3
This systematic review will attempt to collate and synthesize the available evidence on the application of AI to ECG for the diagnosis of ACS, assessing its accuracy, reliability, and clinical usefulness. This review will also identify gaps in the current evidence base, providing guidance for future research in this area.
Through this systematic review, we aim to provide a comprehensive evaluation of AI’s role in ACS diagnosis through 12-lead ECG interpretation, potentially informing clinical practice and guiding the adoption of AI algorithms for ECG interpretation in the clinical domain.
Methods
2
Study Design and Registration
2.1
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines.13 The review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (ID: CRD42023432835). The main objective of this review was to investigate the effectiveness and accuracy of AI techniques in interpreting ECGs for diagnosing ACS.
Search Strategy
2.2
A comprehensive search strategy was developed in collaboration with an experienced reference librarian using a combination of database-specific subject headings and text words for the main concepts of AI, ECG, and ACS. Results were limited to adult human studies and the English language. No other limits were applied. We searched the following databases on June 15, 2023: Ovid MEDLINE, Ovid Embase, Cochrane Database of Systematic Reviews (Ovid), and Cochrane Central Register of Controlled Trials (Ovid). See https://doi.org/10.5683/SP3/XLFZCD for full search strategies. The reference lists of retrieved publications were also searched and considered for inclusion.
Selection of Studies
2.3
Studies were selected for our review based on a number of inclusion criteria. They were limited to adult patients (≥18 years) who underwent an ECG due to suspicion or diagnosis of ACS in acute care settings including the prehospital setting, emergency departments (EDs), in-patient wards, and intensive care units. The studies also employed AI techniques, as defined by the study authors, for interpreting ECGs in the context of ACS symptoms. Eligible comparators included clinician interpretation (retrospective or real time), commercial ECG software using rule-based criteria, or other AI models, as reported by each study.
The primary outcome of interest was the diagnostic accuracy of ACS, including ACS subtypes (ST-elevated myocardial infarction [STEMI], non-STEMI [NSTEMI], and occlusion MI [OMI]) as determined by AI techniques. We reported the sensitivity and specificity for the primary outcome(s) of diagnostic accuracy of ACS. Secondary outcomes included measures of diagnostic performance including, positive predictive value (PPV), negative predictive value (NPV), accuracy, area under the receiver operator curve (AUROC), and F1 scores. Secondary clinical outcomes included territory of infarct, time to diagnosis, diagnostic accuracy compared with physician decision making, and any reported adverse events.
These outcomes were selected as they represent standard diagnostic performance metrics in AI literature.1 Given the heterogeneity in outcome definitions and study methodologies, we did not apply fixed thresholds or conduct a meta-analysis; instead, we used a descriptive synthesis. Additionally, we conducted a subgroup analysis for studies specifically evaluating STEMI/OMI, given its clinical importance.
Studies were excluded if they were case reports, case series, review articles, editorials, or commentaries. Additionally, studies that were still in progress, were not in the English language, did not report on any outcomes or evaluation, did not identify themselves as studying AI or ML, or evaluated AI/ML in stable coronary artery disease were also excluded. Studies that included non-ECG data (ie, clinical or laboratory data) in their AI algorithms or those that used ECG data from large public databases were also excluded from this study. The focus was on studies using ECGs from clinical settings. Furthermore, studies missing basic statistical measures such as the sample size, number of patients with the condition (ie, ACS), sensitivity, or specificity were excluded.
Data Extraction and Synthesis
2.4
All records were initially managed through the Zotero reference management software, in which all citations from each database were imported. Two reviewers (AF and AM) independently assessed study titles and abstracts according to the established inclusion criteria. Subsequently, AF and AM examined full texts to assess for eligibility. Any disagreements between the 2 reviewers were resolved through discussion and consultation with a third reviewer (SM). All screening was done using Covidence. A standardized data extraction form was developed and pilot-tested on a sample of included studies (10 studies) to ensure its applicability. Data extraction was led by 1 reviewer (AF) and subsequently confirmed by the second reviewer (AM). Any disagreements in data extraction were resolved through discussion and consultation of the third reviewer (SM).
Data Analysis
2.5
Sensitivity and specificity values were extracted from the included studies and used to generate forest plots. Pooled estimates of sensitivity and specificity were calculated to summarize diagnostic performance across studies. To assess bias, the Prediction model Risk Of Bias Assessment Tool (PROBAST) was used to assess the risk of bias in the articles included.14 It systematically addressed the following domains: study participants, predictors, outcomes, and statistical analyses. In each of these 4 domains, a scoring scale was used to categorize the risk of bias and applicability concerns into “low,” “high,” or “unclear.” Two reviewers (AF and AM) independently assessed risk of bias using PROBAST. Any discrepancies were resolved by a third reviewer (SM).
Results
3
Study Selection
3.1
Our search strategy yielded a total of 2051 articles. After the removal of duplicates, 1496 articles remained for title and abstract screening. After the initial screening, 228 articles were assessed for eligibility through full-text review. For 3 articles, the full text was not retrievable, and these were excluded. After full-text review of the remaining 225 articles, 201 were excluded, with 24 studies meeting the inclusion criteria and were included in the final review (Table S1). The PRISMA flow diagram in Figure 1 provides a detailed overview of the study selection process.Figure 1PRISMA flow diagram for study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews.
Article Characteristics
3.2
The 24 studies included in this review were published over a span of 26 years from 1997 to 2023. These studies originated from a variety of countries, with the majority coming from the United States of America (7 articles), followed by China and South Korean (4 articles each), Sweden (3 articles), Taiwan and Japan (2 articles each), and Germany and Iran (1 article each). The studies varied in terms of their design, specific ACS outcome, and reference standard for ACS diagnosis. Only 3 studies evaluated the AI algorithms’ diagnostic performance in localizing ACS diagnosis. The majority of articles, 75% (18/24), relied on physicians evaluating patient records, which included data from ECGs and laboratory results, to establish the diagnosis of ACS as their ground truth. More specifically, 6 articles mentioned the involvement of 2independent physicians for review, 3 articles reported a review process conducted by 3 independent cardiologists, and 3 articles referenced the discharge summary. A detailed summary of the characteristics of the included studies is provided in Table 1.15 Moreover, only 3 out of the 24 studies published their code publicly (Table S2).Table 1. Characteristics of included studies and their outcomes of interest.First author et alYearCountryStudy designACS outcome of interestAssess location of infarctionReference standard for ACS diagnosisDetails of ACS diagnosis by physiciansNon-ACS outcomes reviewed in the studyAl-Zaiti et al2020USAProspectiveMINoPhysician2 independent physiciansNoneAl-Zaiti et al2023USAProspectiveOMINoPhysician2 independent physiciansNoneBouzid et al2023USAProspectiveSTEMI and NSTEMINoPhysician2 independent physiciansNoneBouzid et al (a)2021USAProspectiveMINoPhysician2 independent physiciansNoneBouzid et al (b)2021USAProspectiveMIYesPhysician2 independent physiciansNoneCho et al2020South KoreaRetrospectiveMIYesCANANoneChoi et al2023South KoreaRetrospectiveMINoCANANoneChoi et al2022South KoreaRetrospectiveSTEMINoPhysician7 ED physicians and 3 cardiologistsNoneForberg et al152009SwedenRetrospectiveMINoPhysicianDischarge summaryNoneForberg et al2012SwedenRetrospectiveSTEMINoPhysician2 independent physiciansNoneGreen et al2006SwedenRetrospectiveMINoPhysicianDischarge summaryNoneHao et al2020ChinaRetrospectiveMINoPhysicianMultiple cardiologistsNoneKaiser et al1996GermanyRetrospectiveMIYesECHO or CANALVHKim et al2022South KoreaRetrospectiveSTEMINoPhysicianDischarge summaryNoneKimura et al2019JapanRetrospectiveMINoCANANoneKojuri et al2015IranProspectiveMINoPhysicianUnknownNoneLiu et al2021TaiwanRetrospectiveSTEMI and NSTEMINoCANANoneOuyang et al1997JapanRetrospectiveMINoPhysicianUnknownNonePolak et al1997USARetrospectiveMINoPhysicianUnknownNoneTseng et al2023TaiwanRetrospectiveSTEMINoCANANoneWang et al2023ChinaProspectiveMINoPhysician3 CardiologistsArrythmia and LVHWu et al (a)2022ChinaProspectiveSTEMINoPhysician3 CardiologistsNoneWu et al (b)2022ChinaProspectiveSTEMINoPhysician3 CardiologistsNoneXue et al2001USAProspectiveMINoPhysicianUnknownNoneACS, acute coronary syndrome; CA, coronary angiography; ECHO, echocardiogram; ED, emergency department; LVH, left ventricular hypertrophy; MI, myocardial infarction; NA, not applicable; NSTEMI, non-ST-elevated myocardial infarction; OMI, occlusion myocardial; STEMI, ST-elevated myocardial infarction.
AI Models and Patient Population
3.3
Sample size, patient population characteristics, and the specific AI techniques employed for ECG interpretation in the context of ACS are summarized in Table 2.15 The articles used a wide range of AI techniques, with 66.7% (16/24) of the articles employing DL methods (artificial neural networks and convoluted neural networks), 25.0% (6/24) employing traditional ML methods (logistic regression, gradient boosting machine, random forest, long short-term memory, and least absolute shrinkage and selection operator), and 3% (2/24) employing hybrid methods (adaptive logic computing network and fusions).Table 2. Patient demographics of included studies and AI models used.First author et alYearAI model usedSample size, nMean age, yFemales, %Patients with ACS, %(n)No. of ECGs, nECGs with ACS, %(n)Al-Zaiti et al2020Fusion: LR + GBM + ANN1224594216.8 (206)122416.8 (206)Al-Zaiti et al2023RF7313594714.9 (1087)731314.9 (1087)Bouzid et al2023RF2122595313.6 (288)NRNRBouzid et al (a)2021LR1244594916.6 (206)124416.6 (206)Bouzid et al (b)2021RF2400594715.8 (380)240015.8 (380)Cho et al2020DL1768626212.7 (225)176812.7 (225)Choi et al2023DL10,160622016.6 (1689)10,16016.6 (1689)Choi et al2022CNN187622551.3 (96)NRNRForberg et al2009ANN8614040.0 (344)861NRForberg et al152012ANN560704517.5 (98)56017.5 (98)Green et al2006ANN634654320.5 (130)NRHao et al2020CNN957NRNR50.5 (483)95750.5 (483)Kaiser et al1996Rule-based learning60570.9 (429)60570.9 (429)Kim et al2022CNN80652167.5 (54)8067.5 (54)Kimura et al2019Neural network - bidirectional LSTM792NRNR14.3 (113)NRNRKojuri et al2015ANN multilayer perceptron935NR568.8 (82)NRNRLiu et al2021DL77,799NRNR1.3 (1024)1420841.3 (1748)Ouyang et al1997ANN13250NR25.0 (33)NRNRPolak et al1997Adaptive logic computing network1367NR543.7 (50)NRNRTseng et al2023CNN384NR34.4 (132)NRNRWang et al2023CNN3392393.663.5 (118)NRNRWu et al (a)2022CNN-LTSM883NR3335.7 (315)NRNRWu et al (b)2022LASSO820NR347.2 (59)259NRXue et al2001Neural network2308NRNR58.0 (1339)NRNRACS, acute coronary syndrome; AI, artificial intelligence; ANN, artificial neural network; CNN, convolutional neural network; DL, deep learning; ECG, electrocardiogram; GBM, gradient boosting machine; LASSO, least absolute shrinkage and selection operator; LR, logistic regression; LSTM, long short-term memory; NR, not reported; RF, random forest.
Table 3 summarizes the diagnostic performance metrics for the 24 studies. The sensitivity of AI-based diagnosis for ACS among the 24 studies varied from 68% to 98%, and the specificity varied from 41% to 98% (Figs 2 and 3, respectively).Table 3. Diagnostic performance metrics of artificial intelligence models for acute coronary syndrome diagnosis using electrocardiogram interpretation.First author et alYearSensitivity, %Specificity, %AUROC, %F1 score, %Accuracy, %PPV, %NPV, %Al-Zaiti et al2020777682NRNR43NRAl-Zaiti et al20236898.979NRNR82.592.5Bouzid et al2023759583NRNRNRNRBouzid et al (a)2021727379NRNR3892Bouzid et al (b)202171.7184.7385NRNR36.1396.13Cho et al202084.488.590.1NRNR51.897.5Choi et al202376.992.192.375.888.5NRNRChoi et al202285.482.491.9NRNR83.784.3Forberg et al152009954486NRNR5394Forberg et al2012956893NRNR1899Green et al20069541.180.2NRNR29.597.2Hao et al20209696NR9495NRNRKaiser et al19967698NRNRNR99NRKim et al2022987795NRNR9095Kimura et al2019798788NR83NRNRKojuri et al20159398NRNR969982Liu et al2021909598NRNRNRNROuyang et al199790.293.3NRNR91.8NRNRPolak et al19977266NRNR67NRNRTseng et al202385.992.9NRNR83.7NRNRWang et al202397.196.88NRNR97.2NRNRWu et al (a)2022979710098989999Wu et al (b)2022979398NR959397Xue et al20019854NRNRNRNRNRAUROC, area under receiver operating curve; NPV, negative predictive value; NR, not reported; PPV, positive predictive value.Figure 2. Forest plot of sensitivity of included studies. Pooled sensitivity, 88.9% (95% CI, 84.1%-92.4%).Figure 3. Forest plot of specificity of included studies. Pooled specificity, 88.7% (95% CI, 82.1%-93.1%).
Subgroup Analysis
3.4
Among the 24 studies reviewed, 7 specifically evaluated AI’s diagnostic performance for STEMI/OMI. The sensitivity of AI-based diagnosis for STEMI/OMI among the 7 studies varied from 68% to 97%, and the specificity varied from 68% to 99% (Figs S1 and S2, respectively).
Comparative Analysis of Diagnostic Performance
3.5
Out of the 24 articles, 75.0% (n = 18/24) compared their AI algorithm’s diagnostic performance to another modality. The comparative diagnostic performance is summarized in Table 4.15 The most common comparison was against the performance of a group of expert clinicians in diagnosing ACS events (MI, STEMI, and OMI) based on ECGs (33%, 8/24). These evaluations were conducted retrospectively and blinded to clinical outcomes to minimize bias. Only 1 study (Forberg et al 2012) compared their AI model with the real-time interpretation of ECGs by coronary care unit physicians.15 One study (Kim et al 2022), in addition to expert clinician performance, also reported real-time performance of emergency medicine physicians.16 Twenty-five percent of articles (6/24) compared their AI performance with commercial non-ML software. These tools rely on predefined rules or criteria, such as the HEART score17 and classical ECG criteria,15 rather than advanced ML techniques. Three articles (12.5%) compared their AI model’s diagnostic performance with that of other AI articles.Table 4. Diagnostic performance metrics of clinicians and non-AI commercial software for ACS diagnosis using electrocardiogram interpretation.First author et alYearACS event assessedAI comparatorExpert cliniciansSoftwareSensitivity, %Specificity, %AUROC, %PPV, %NPV, %Sensitivity, %Specificity, %AUROC, %PPV, %NPV, %Al-Zaiti et ala2020Any ACS eventClinicians + software + criteria40946763872598627985Al-Zaiti et al2023OMIClinicians + softwareNRNR72NRNRNRNR68NRNRBouzid et al2023Any ACS eventClinicians35.785.86227.889.7NRNRNRNRNRBouzid et al (a)2021Any ACS eventClinicians + software4094NR63882598NR7985Bouzid et al (b)2021Any ACS eventSoftwareNRNRNRNRNR31.2195.61NR50.5392.66Cho et alb2020MISoftwareNRNRNRNRNR81.981.4NR15.899.1Choi et al2023MISoftwareNRNRNRNRNR72.862.272.8NRNRChoi et al2022STEMIClinicians87.558.285.668.881.6NRNRNRNRNRForberg et al15c2009Any ACS eventClinician + criteria8263783991NRNRNRNRNRForberg et ale2012STEMIClinicians7498NR7698NRNRNRNRNRGreen et al2006NAOther AI modelsNRNRNRNRNRNRNRNRNRNRHao et al2020NANoneNRNRNRNRNRNRNRNRNRNRKaiser et al1996NANoneNRNRNRNRNRNRNRNRNRNRKim et alf2022STEMIClinicians9458768283NRNRNRNRNRKimura et al2019NANoneNRNRNRNRNRNRNRNRNRNRKojuri et al2015NANoneNRNRNRNRNRNRNRNRNRNRLiu et al2021STEMIClinicians + softwareNRNRNRNRNRNRNRNRNRNROuyang et al1997NANoneNRNRNRNRNRNRNRNRNRNRPolak et al1997MISoftwareNRNRNRNRNR7654NRNRNRTseng et al2023NAOther AI modelsNRNRNRNRNRNRNRNRNRNRWang et al2023NAOther AI modelsNRNRNRNRNRNRNRNRNRNRWu et al (a)d2022STEMIClinicians9292929292NRNRNRNRNRWu et al (b)2022STEMIClinicians7293837594NRNRNRNRNRXue et al2001NANoneNRNRNRNRNRNRNRNRNRNRACS, acute coronary syndrome; AI, artificial intelligence; AUROC, area under receiver operating curve; MI, myocardial infarction; NA, not applicable; NPV, negative predictive value; NR, not reported; OMI, occlusion myocardial infarction; PPV, positive predictive value; STEMI, ST-elevated myocardial infarction.aCriteria AUROC: 84.bSoftware F1 and accuracy scores: 67 for both.cCriteria AUROC, sensitivity, specificity, PPV, and NPV; 76, 75, 36, 39, and 91, respectively.dClinician F1 and accuracy scores: 92 for both.eReal-time interpretation by coronary care unit physicians.fComparison to real-time interpretation by emergency medicine physicians; sensitivity, specificity, PPV, and NPV; 57, 85, 89, and 49, respectively.
AI models were more sensitive (90% of studies, n = 9/10) and had better PPV (100% of studies, n = 10/10) compared with clinicians. However, specificity varied, with only 50% of the studies (n = 5/10) showing that AI models were more specific compared with clinicians, whereas the remaining studies showed comparable or superior clinician specificity. Clinicians had better NPV (70% of studies, n = 7/10) compared with AI models. Additionally, AI models had better AUROC compared with clinicians in all 8 studies that reported on that metric.
In the comparison of AI models to commercial non-ML software across 7 studies, AI models consistently demonstrated higher sensitivity in diagnosing ACS (86% of studies, n = 6/7). Specificity results were mixed, with 57% of studies (n = 4/7) reporting superior specificity of AI models. AI models had better PPV compared with software in 83% of studies (n = 5/6). However, software had better NPV compared with AI models in 60% of studies (n = 3/5).
Risk of Bias Assessment
3.6
Table S3 delineates the PROBAST evaluation of risk of bias and applicability considerations for the articles included in the systematic review. The analysis revealed that the majority of studies demonstrated an unclear risk of bias in at least 1 domain—most notably within predictors, outcome, and analysis. The overall risk of bias was pronounced, with a high concern identified in 38% of the studies (n = 9/24) and an unclear concern observed in half of the studies (Fig S3). The participant domain, along with the analysis domain—specifically regarding the adequacy of participant numbers and the handling of missing data—were recurrent sources of high risk. The high risk of bias was not apparent in the outcome and predictors domain, with none of the studies receiving a rating of high risk, and only 17% (n = 4/24) and 21% (n = 5/24), respectively, marked as unclear. This suggests that biases related to outcome determination and predictor selection were less prevalent. Applicability concerns were minimal, reflecting the studies’ alignment with the populations, predictors, and outcomes detailed in the review question; only a small fraction exhibited high (13%, n = 3/24) or unclear (8%, n = 2/24) overall applicability risk (Fig S4).
Limitations
4
Our systematic review is not without limitations. We excluded studies that used ECGs from databases, which several articles have used to develop AI models. This approach was taken to focus on real-world data at the expense of excluding some of these AI models. Moreover, we excluded articles with missing sensitivities and specificities. The evaluation of a model’s performance cannot be fully encapsulated merely by its sensitivity and specificity, as some models offer the ability to adjust the threshold, thus balancing the trade-off between sensitivity and specificity.
Additionally, our literature search was conducted in June 2023. Given the rapid pace of advancement in the field of AI, particularly in ECG interpretation, it is possible that relevant studies published after this date were not captured. As such, our findings may not fully reflect the most recent developments in AI-based diagnostic tools for ACS.
In the comparative analysis between AI performance and clinician performance, the majority of articles used a group of physicians that retrospectively annotated the ECGs. This might have overestimated the diagnostic performance of clinicians as compared with AI and may not reflect real-world performance. Only 1 study compared their model with real-time ED physician interpretation.15 Future research should explore this comparison to provide a more comprehensive understanding of AI’s practical utility in dynamic clinical environments.
In assessing the clinical significance of AI models in the diagnosis of ACS using ECGs, our analysis revealed considerable heterogeneity in outcomes, underscoring an imperative limitation in directly comparing various AI approaches. This variability stems from a multitude of factors, including the distinct design methodologies of AI models and the diverse patient populations studied. Variability in reference standards for diagnosing STEMI or OMI across studies, including differences in criteria such as complete occlusion, thrombosis in myocardial infarction flow grades, and the identification of culprit lesions, may have also influenced the consistency and comparability of reported diagnostic performance metrics.
Transparency in AI development remains a significant challenge, particularly with the prevalence of proprietary licensing and limited code availability. As noted in Table S2, although several models showed superior performance in the detection of ACS, most studies did not disclose their algorithms, which could impede validation and integration into clinical practice. This introduces an additional layer of opacity, restricting the reproducibility and validation of the reported AI algorithms. Overcoming this barrier will require a commitment to open science and standardization of reporting protocols. Additionally, although AI tools for ECG interpretation may initially be limited to cardiologists, developing accessible systems for ED settings can help frontline physicians leverage AI for faster, more accurate decision making, enhancing workflows without disruption.
Although this study did not include a cost analysis of AI technologies, the economic implications are critical for their widespread adoption in clinical settings. Adopting AI tools requires addressing the learning curve through Continuing Medical Education programs that teach clinicians to understand predictions, limitations, and effective integration into patient care. Future studies should evaluate the cost effectiveness of these technologies, including an analysis of particular brands and their performance, to better understand their potential for integration into healthcare systems.
Lastly, there is also a need to test if these AI models led to a change in outcome and any associated adverse events, including time to diagnosis. It is assumed that early and timely diagnosis of ACS would lead to better outcomes; however, this has to be explored and quantified. Similarly, the impact of AI models on identifying the territory of infarct was also not adequately addressed in this review, as very few studies addressed this outcome. Territory of infarct is a critical aspect of ACS diagnosis and can have implications on emergent management.
Discussion
5
Our Study
5.1
Our study is the largest study to examine the application of ML algorithms, not limited to DL, for diagnosing ACS using ECGs in real-world clinical settings. Our review incorporates studies from multicenter populations presenting with suspected ACS in emergency care settings, thereby enhancing external validity and generalizability. We chose to include studies that also compare the diagnostic accuracy of their algorithms with other published articles and not only limit it to articles with direct AI-to-clinician comparisons.
AI in 12-Lead ECG Interpretation to Diagnosis ACS
5.2
Our systematic review included 24 articles, which collectively demonstrated that AI algorithms exhibit high diagnostic performance in detecting ACS using ECGs in acute care settings. Across the studies, reported sensitivities ranged from 68% to 98% and specificities from 41% to 98%, highlighting the variability in performance across different AI models and study designs. In comparison, the sensitivity and specificity of manual acute MI diagnosis have been reported as 91% and 51%, respectively.18 This shows the potential for AI in enhancing diagnostic speed and potentially reducing human error when it comes to ACS. Similar work has been conducted in which AI ECG analyses were evaluated for their prediction of structural cardiac pathologies, including, left ventricular systolic dysfunction, myocardial hypertrophy, heart failure, silent atrial fibrillation, hypertrophic cardiomyopathy, and bundle branch blocks.4^,^19, 20, 21, 22, 23 Two recent studies by Herman et al,24^,^25 published after the conclusion of our search, examined 2 large patient populations and demonstrated that an AI-powered ECG system outperformed current computerized interpretations in diagnostic accuracy across various cardiac conditions. These studies, achieving high F1 scores, align with our conclusions, reinforcing the potential of AI-powered ECG systems as reliable clinical tools.
STEMI/OMI
5.3
Subgroup analysis revealed that AI’s diagnostic performance for STEMI/OMI showed higher sensitivity and specificity, suggesting that AI might be more effective in this context. However, this improvement does not fully explain the heterogeneity observed in the overall results, indicating that other factors contribute to the variability across studies. Although AI appears better suited for diagnosing STEMI/OMI, further research is needed to understand the sources of heterogeneity and to validate these findings across broader clinical scenarios. Future advancements in AI algorithms should prioritize this subset, as timely detection of OMIs is critical to optimizing patient outcomes in acute care settings.
Comparative Analysis: AI vs Clinician and Software Performance
5.4
Our review showed that for the diagnosis of ACS, AI models had higher sensitivity than clinicians while maintaining similar specificity. Similarly, AI models showed superior PPV; however, those gains were balanced by decreases in NPV. The gains in sensitivity and PPV show AI’s potential to be used for ruling out ACS in acute care settings. Furthermore, the higher AUROC values seen in ECG-based AI models, positions it well to be used as a discriminatory tool for ACS.
When AI models were compared with commercial software, the results were similarly encouraging for AI, with gains in sensitivity, and PPV while maintaining specificity and NPV. Overall, however, NPV and AUROC results were less consistently reported for software comparisons, suggesting that more research is needed to fully understand the performance of AI vs non-ML commercial software. These findings indicate that AI holds considerable promise for enhancing the diagnosis of ACS. It may improve early detection and reduce false negatives, which are critical in acute settings. Yet, the importance of clinician expertise remains, particularly in avoiding false positives and providing comprehensive patient care that considers the nuances AI might miss. These aspects highlight crucial considerations for integrating AI into clinical practice, especially regarding how AI could augment clinician judgment.
Risk of Bias Assessment
5.5
The PROBAST evaluation conducted in this systematic review serves to highlight key areas within the current body of literature on AI algorithms for ACS diagnosis via ECG that require careful consideration. Notably, the prevalence of unclear risk of bias across several domains raises concerns about the methodologic transparency in these studies. Specifically, the high risk of bias in 38% of the included studies underscores a critical need for more rigorous methodologic design and reporting, particularly in participant recruitment and the statistical handling of data. Although none of the studies showed a high risk of bias for outcome and predictors, a significant proportion exhibited unclear risk (17% for outcomes and 21% for predictors), indicating that there are still gaps in how these aspects are being reported. Without clear and comprehensive reporting of how outcomes and predictors are determined, the potential for bias cannot be adequately assessed, which casts doubt on the reliability and applicability of the findings.
Furthermore, the minimal concerns regarding applicability are promising, suggesting that the studies are relevant to the populations, predictors, and outcomes of interest. This relevance is paramount for the translation of research findings into clinical practice. Nevertheless, the presence of any high risk of applicability (13%) cannot be overlooked as it may signal a disconnect between the research settings and real-world clinical environments.
The identified areas of high and unclear risk in our PROBAST analysis reflect a broader issue in the field of AI research in healthcare—namely the necessity for a standardized approach to the reporting and validation of AI models. As AI continues to advance, it is imperative that these models are developed and reported with a level of rigor that instills confidence in their predictive capabilities and their potential for integration into clinical decision-making processes.
Clinical Significance
5.6
The broader implications of these findings suggest that AI could play a critical role in settings in which immediate expert interpretation of ECG is not available in real time, thus supporting timely clinical decision making. As we consider the integration of AI into clinical workflows, it is imperative to recognize the balance required between AI’s high sensitivity and the need to mitigate potential false positives, which could be informed by the clinician’s expertise and consideration of the patient’s overall clinical picture. AI’s role in ECG interpretation is not intended to replace the clinical judgment of ED physicians but rather to complement their expertise. By providing high sensitivity and rapid assessments, AI can enhance decision making while allowing physicians to focus on holistic patient care. Maintaining this balance is essential for maximizing AI’s benefits without diminishing the critical contributions of human clinicians. Although our study elucidates the strengths of AI in ACS diagnosis, it also identifies critical areas for future investigation, particularly concerning the integration of AI in the clinical decision-making process and the consequent impact on patient outcomes. It is this potential to contribute to earlier and more accurate ACS diagnoses, ultimately leading to timely and effective patient management, that underpins the clinical significance of our systematic review.
Our systematic review suggests that AI-based algorithms perform well in the diagnosis of ACS using ECGs. Notably, AI has demonstrated superior performance to clinicians and standard software in many instances, albeit with considerable variability in specificity and NPV. Such variability calls for judicious use of AI, complementing rather than supplanting clinician judgment. The heterogeneity of outcomes limits direct comparison of the various AI techniques, emphasizing the need for standardized protocols, publishing of ML codes publicly, and clear interpretability in AI solutions. The risk of bias assessment underscored the importance of addressing methodologic and reporting inconsistencies in AI research. Moving forward, further research is crucial to fine-tune AI tools for consistent and transparent clinical application, ultimately improving patient outcomes. By improving these areas, future studies can enhance the strength of evidence for AI applications in diagnosing ACS and ultimately aid in the advancement of precision medicine.
Author Contributions
All authors have made substantial contributions to this study. AF was the first reviewer, contributing to the study design and protocol creation. AM was the second reviewer. Both AF and AM were involved in full-text screening, with AF taking the lead in data extraction. AO and JM were responsible for the development and execution of the search strategy. SM conceptualized the study, provided supervision throughout the review process, and resolved screening conflicts. All authors were involved the preparation and review of the manuscript.
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
Conflict of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Topol E.J.High-performance medicine: the convergence of human and artificial intelligence Nat Med 2512019445610.1038/s 41591-018-0300-730617339 · doi ↗ · pubmed ↗
- 2Raghunath S.Ulloa Cerna A.E.Jing L.Prediction of mortality from 12-lead electrocardiogram voltage data using a deep neural network Nat Med 266202088689110.1038/s 41591-020-0870-z 32393799 · doi ↗ · pubmed ↗
- 3Bhatt D.L.Lopes R.D.Harrington R.A.Diagnosis and treatment of acute coronary syndromes: a review JAMA 3277202266267510.1001/jama.2022.035835166796 · doi ↗ · pubmed ↗
- 4Hassannataj Joloudari J.Mojrian S.Nodehi I.Application of artificial intelligence techniques for automated detection of myocardial infarction: a review Physiol Meas 438202208 TR 0110.1088/1361-6579/ac 7fd 935803247 · doi ↗ · pubmed ↗
- 5Xiao R, Ding C, Hu X, et al. Integrating multimodal information in machine learning for classifying acute myocardial infarction. Physiol Meas. 44(4):044002. https://doi.org/10.1088/1361-6579/acc 77f.10.1088/1361-6579/acc 77f PMC 1011187736963114 · doi ↗ · pubmed ↗
- 6Jahmunah V.Ng E.Y.K.San T.R.Acharya U.R.Automated detection of coronary artery disease, myocardial infarction and congestive heart failure using Gabor CNN model with ECG signals Comput Biol Med 134202110445710.1016/j.compbiomed.2021.10445733991857 · doi ↗ · pubmed ↗
- 7Gibson C.M.Mehta S.Ceschim M.R.S.Evolution of single-lead ECG for STEMI detection using a deep learning approach Int J Cardiol 3462022475210.1016/j.ijcard.2021.11.03934801613 · doi ↗ · pubmed ↗
- 8Tadesse G.A.Javed H.Weldemariam K.Deep MI: deep multi-lead ECG fusion for identifying myocardial infarction and its occurrence-time Artif Intell Med 121202110219210.1016/j.artmed.2021.10219234763807 · doi ↗ · pubmed ↗