Prevalence and factors associated with postpartum depressive symptoms among mothers who gave birth within the past 12 months in Ghana: mixed-method study
Leticia Tornyevah, Samuel Bosomprah, Anjali Sharma, Ank De Jonge, Jens Henrichs

TL;DR
This study found that nearly 30% of mothers in Ghana experience postpartum depressive symptoms, linked to factors like lack of support and low self-esteem.
Contribution
The study combines quantitative and qualitative methods to explore PPDS in Ghana, revealing psychosocial pathways and modifiable risk factors.
Findings
29.3% of surveyed mothers screened positive for postpartum depressive symptoms.
Factors like lack of partner support and low self-esteem were strongly associated with PPDS.
Thematic analysis identified social isolation and emotional stress as key themes influencing PPDS.
Abstract
Postpartum depressive symptoms (PPDS) are mental health concerns, characterised by sadness, anxiety and suicidal ideation. We aimed to estimate the prevalence of PPDS, identify its associated factors and explore the lived experiences of individuals with PPDS, to understand the psychosocial mechanisms involved. We surveyed 400 women aged 18 years and above and conducted in-depth interviews among 19 women who screened positive for PPDS at two urban hospitals and one peri-urban polyclinic in Ho, Ghana. We used multivariable binomial generalised linear models to identify factors independently associated with PPDS. We used thematic analysis (qualitative) to identify themes that highlight pathways through which these factors influence PPDS. Overall, 117 (29.3%) women screened positive for PPDS. Being unmarried (adjusted prevalence ratio (aPR) 1.33, 95% CI 1.02–1.72), lack of partner…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
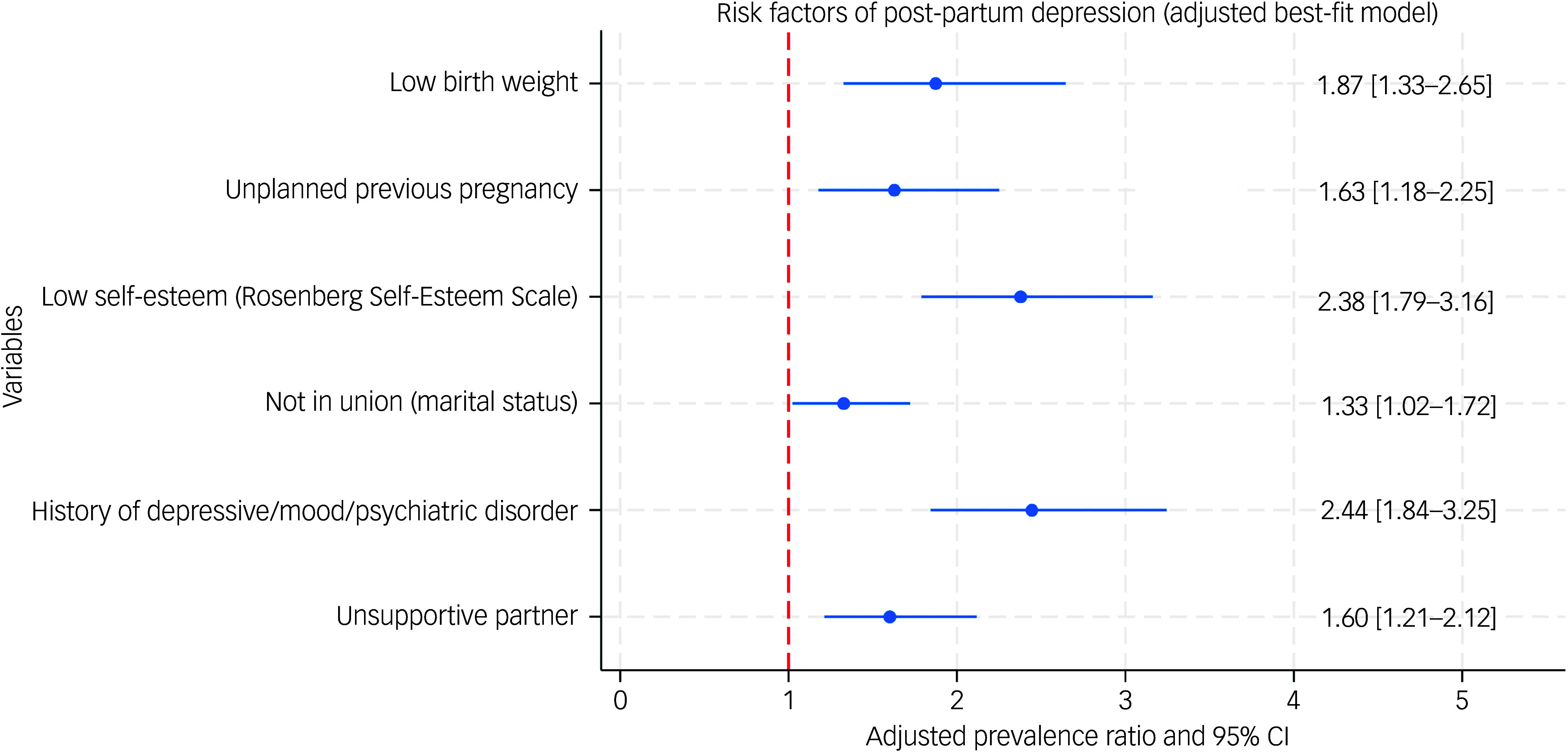 Figure 1
Figure 1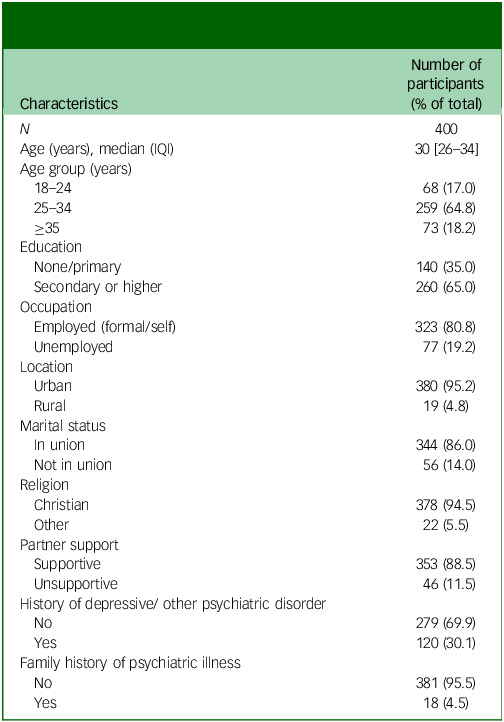 Figure 2
Figure 2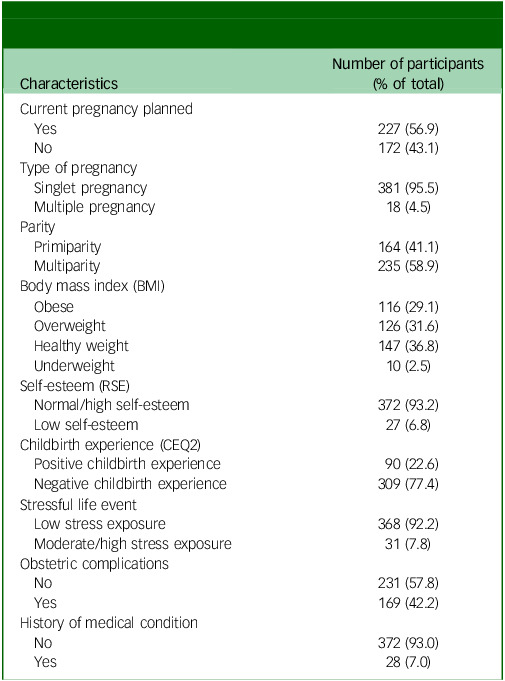 Figure 3
Figure 3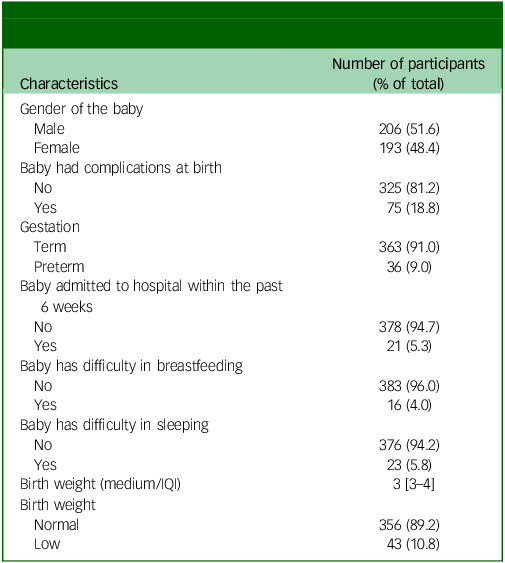 Figure 4
Figure 4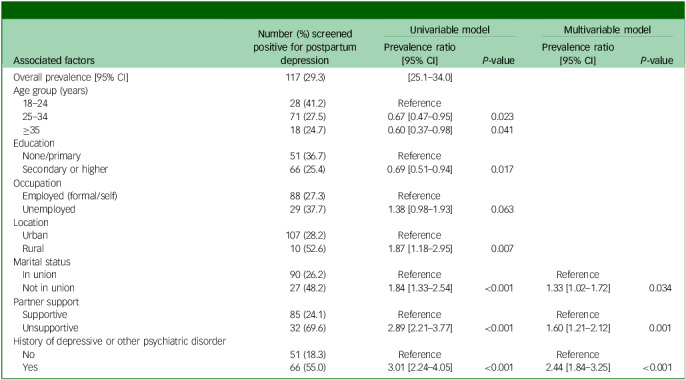 Figure 5
Figure 5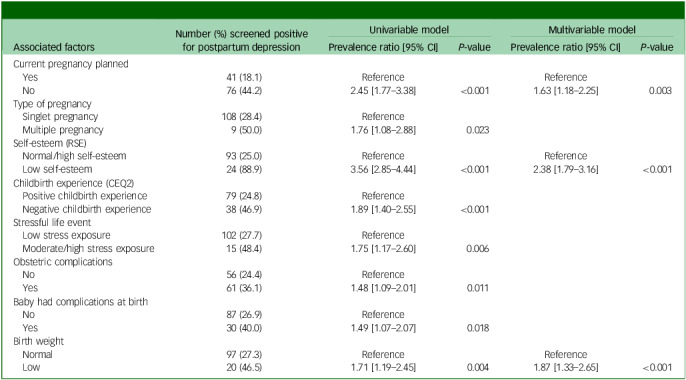 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Maternal and Perinatal Health Interventions · Attachment and Relationship Dynamics
Postpartum depressive symptoms (PPDS) are a significant but often overlooked mental health problem. Globally, about 10–25% of women experience significant depressive symptoms after childbirth.^ 1 ^ Sub-Saharan Africa appears to bear a particularly high burden, with a pooled prevalence around 22%;^ 1 ^ reported rates vary widely.^ 1 ^ In Ghana, studies likewise report highly variable rates of PPDS; community-based surveys in northern Ghana often find rates in the mid-20% range, whereas urban facility-based studies (e.g. in Greater Accra) tend to find much lower rates.^ 2 ^ Overall, reported prevalences of PPDS in Ghana have ranged from the single digits up to about 40%, with pooled estimates on the order of only 9–10%.^ 2 ^ These disparities may suggest that many cases go unrecognised. Cultural stigma and low awareness contribute to underdiagnosis; nearly half of Ghanaian mothers with PPDS may remain untreated because of stigma and privacy concerns.^ 2 ^ Mental health services are scarce and unevenly distributed in Ghana; all three large psychiatric hospitals are located on the southern coast,^ 3 ^ leaving rural and northern areas particularly underserved. Moreover, just recently, the Ghanaian Government started to invest more into mental healthcare services, and until the end of 2024, healthcare costs related to the treatment of major mental health problems, like depression or bipolar disorder, were not financially covered by health insurance in Ghana.^ 4 ^
Identifying the factors associated with PPDS and understanding how these factors contribute to PPDS are critical for optimising culturally sensitive screening tools, intervention strategies and support programmes to improve maternal and child health. Several factors, such as a lack of spousal support,^ 5 ^ low self-esteem,^ 6 ^ unplanned pregnancies^ 5 ^ and low birth weight,^ 7 ^ are known to increase the risk of developing PPDS. These factors often work together with social and psychological dynamics, placing significant emotional strain on mothers during the postpartum period. For example, women without a supportive partner often feel isolated and overwhelmed, harbouring persistent negative self-appraisal.^ 8,9 ^ Unplanned pregnancies can create additional financial and emotional pressures.^ 8 ^ Caring for a low-birth-weight baby may lead to increased anxiety and self-doubt about parenting abilities,^ 7 ^ further increasing their vulnerability to depressive symptoms.^ 10,11 ^ Most of the existing research in Ghana, however, has relied on surveys,^ 2 ^ with little exploration of the underlying mechanisms that can explain the quantitative data; for example, how mothers personally experience and cope with PPDS in their daily lives. There is a clear paucity of qualitative data on the lived experiences, social dynamics and cultural context underlying PPDS among Ghanaian women. This evidentiary gap in understanding why and how PPDS unfolds in the Ghanaian context suggests the need for a more holistic investigative approach. A mixed-methods study design is well suited to address this gap.
The general aim of this study was to provide a better understanding of PPDS among mothers in Ghana. Specifically, we sought to estimate the prevalence of PPDS among mothers within a year postpartum; identify sociodemographic, psychosocial and maternal factors independently associated with its onset; and explore lived experiences of affected mothers to better understand the emotional, psychological and social challenges contributing to PPDS.
Method
Study design and settings
We conducted an explanatory sequential, mixed-methods, cross-sectional study, beginning with a cross-sectional survey followed by in-depth interviews, at the Ho Teaching Hospital, Ho Municipal Hospital and Ho Polyclinic, from September 2024 to November 2024. We selected the Ho Teaching Hospital and Ho Municipal Hospital (larger urban hospitals) and Ho Polyclinic (serving peri-urban/rural outskirts) because together they serve most births in the Ho area. Ho is the Volta regional capital situated in South Ghana. The design allows quantitative findings to guide qualitative exploration of underlying mechanisms.^ 12 ^
Participants and sampling
Eligible women were those aged 18 years and above, who delivered live infants between September 2023 and September 2024 (i.e. those with a child younger than 12 months). We recruited mothers as they attended postnatal or immunisation clinics at the three facilities. Research assistants informed all eligible women present during data collection days about the study and invited them to participate; those unable or unwilling to consent were excluded. We approached 405 mothers, of which five were excluded (one mother was below 18 years of age, and four mothers had a child older than 12 months), giving an eligibility rate of 98.8%. Of the 400 eligible mothers surveyed, one mother had missing data, leaving 399 (99.8% of those eligible) for analysis.
Sample size considerations
The sample size was calculated based on an assumed prevalence of PPDS in Ghana of 20.3%.^ 2 ^ We used a single-group design to obtain a two-sided 95% confidence interval for a single proportion. To produce a confidence interval with a width of no more than 0.1, at least 246 mothers were needed. The sample size was computed using PASS 2023, version 23.0.2.
We planned purposive sampling of mothers with elevated depressive symptoms. A sample size of 19 in-depth interviews was deemed adequate, as qualitative literature indicates thematic saturation is often reached with 12–15 interviews.^ 13 ^ Indeed, our coding process indicated no new themes emerging in the last few interviews.
Data collection
Following consent, trained research assistants administered the structured questionnaire using Android tablets, in the participant’s preferred language (Ewe or English). All survey data were collected using Castor EDC version 2024.3.4.0 (Castor, Philadelphia, PA, USA; see https://www.castoredc.com/), a certified electronic data capture tool hosted at a secure server of the Amsterdam University Medical Center, for macOS. We incorporated validation checks in the digital survey to optimise data quality assurance and control. The use of anonymous tablets for data collection helped minimise social desirability. We pilot-tested the questionnaire on a convenience sample of ten postpartum women at a nearby clinic and refined wording as needed.
Interview procedures and setting (Consolidated Criteria for Reporting Qualitative Research (COREQ): items 10–15, 17–23)
Interviews were conducted face-to-face in private space within the child welfare clinics at the three facilities, with only the participant and interviewer present; infants were present when breastfeeding was required (no other non-participants were present). After each survey, women with a Patient Health Questionnaire-9 (PHQ-9) score >9 (indicative of PPDS), as automatically identified by the electronic data capture tool, were asked about interest in a follow-up in-depth interview by the trained research assistants. The research assistant took contact and location details from interested women. Women signed an informed consent form before participating in the interview. We encouraged participants eligible for the interview to see a clinician or a nurse to discuss PPDS symptoms and to return to the clinic the next day for an in-depth interview (no repeat interviews). Participants were informed that their care would not be affected by their responses.
A semi-structured interview guide (developed from the literature and the study objectives) covered topics such as experiences during childbirth, postpartum emotional well-being, support from family and community, stressors and coping strategies (Supplementary Table 1 available at https://doi.org/10.1192/bjo.2025.10857). The guide was pilot-tested with two postpartum women from a non-study clinic to refine wording and flow. The average duration of the interview was 45 min. We recorded, with permission, all interviews with a Sony ICD digital voice audio recorder. Brief field notes were written immediately after each interview to capture contextual details and initial analytic impressions. We discussed data sufficiency at regular intervals and concluded that thematic saturation had been reached when no new themes emerged in the final interviews. Transcripts were not returned to participants for correction because of time constraints and to minimise participant burden. Instead, we prioritised clear in-interview summaries and probes to enhance credibility.
We gave GHC45 (approximately US$3) to all survey and interview participants as appreciation for their time. Their familiarity with the culture helped elicit the most accurate responses.^ 14 ^
Research team and reflexivity (COREQ: items 1–8)
Interviews were conducted by L.T. (female, PhD candidate in Mental Health), supported by two female research assistants fluent in Ewe and English. The core team comprised L.T. (PhD candidate), S.B. (PhD, biostatistics), A.S. (ScD, social science), A.D.J. (PhD, midwifery science) and J.H. (PhD, perinatal mental health). At the time of the study, team members were employed at academic or research institutions in Ghana, The Netherlands and Zambia. Interviewers received study-specific training on trauma-informed interviewing, confidentiality and reflexive practice. They conducted mock interviews and reviewed role-plays before data collection. No prior relationships existed with participants. During recruitment, the interviewer introduced herself as a researcher studying postpartum well-being, emphasising the voluntary nature of participation and that there were no right or wrong answers. We maintained a reflexive log to document positionality, assumptions and analytic decisions. The team’s clinical and public health backgrounds were acknowledged as potential sources of interpretive bias. To mitigate these, we used peer debriefs and multidisciplinary review of codes and themes.
Outcome and covariates
The PHQ-9 was used to measure our primary outcome, defined as screening positive for PPDS. The PHQ-9 is a nine-item scale with responses scored on a four-point scale (0 = not at all; 1 = several days; 2 = more than half the days; 3 = nearly every day). The total score ranges from 0 to 27. We used a PHQ-9 score >9 as the cut-off to indicate elevated depressive symptoms, based on evidence indicating this threshold provides strong predictive validity.^ 15 ^ Although the Edinburgh Postnatal Depression Scale (EPDS) is a widely recognised tool specifically designed for PPDS, we selected the PHQ-9 scale because of its broader applicability, strong correlation with the EPDS and demonstrated reliability and validity for detecting PPDS, with a sensitivity of 0.84 and specificity of 0.81.^ 16 ^ Similarly, the PHQ-9 has been validated in Ghana (e.g. Kintampo district) with satisfactory reliability (Cronbach’s alpha of approximately 0.75) and concordant performance with the EPDS.^ 17 ^ Importantly, the PHQ-9 offers practical advantages in this context, being simple, easy to administer and well-suited to Ghanaian women, particularly those with limited formal education, where its straightforward format and accessibility enhance its acceptability and feasibility.^ 17 ^
We collected sociodemographic data (e.g. age, education, marital status, employment, etc.), pregnancy and obstetric history (e.g. parity, pregnancy planning), and psychosocial factors (e.g. partner support, stressful life events, self-esteem) that are potentially related to PPDS based on the literature.^ 5,10 ^ We defined ‘in union’ as being married or cohabiting, and ‘not in union’ as women who were single, divorced, separated or widowed. Cohabiting women were grouped with married women because of sociocultural similarity in support structures in Ghana. We asked mothers a structured question, ‘Has your husband/partner been supportive since delivery? (e.g. providing emotional, financial or practical help)’. We defined ‘partner support’ as ‘supportive’ if moderate/strong support was reported, and ‘unsupportive’ if the mother reported no or poor support from husband/partner. Pregnancy was classified as planned if the mother reported intending the pregnancy; otherwise, it was ‘unplanned’. Low birth weight was defined as <2.5 kg. We asked women if they had any paid work (employment or self-employment) at the time of participating in the survey. Those answering ‘yes’ to any paid work were coded as ‘employed or engaged in paid work’; others (including housewives without income) were coded as ‘unemployed or not working’.
We used the Childbirth Experience Questionnaire 2 (CEQ2) to measure mothers’ experiences during childbirth and labour. The CEQ2 consists of 22 items. For 19 items, we used a four-point Likert scale (1 = totally agree, 2 = mostly agree, 3 = mostly disagree, 4 = totally disagree). Higher scores indicate a negative experience. We assessed three additional items (i.e. labour pain, sense of security and control) using a visual analogue scale (VAS). We categorised VAS scores as follows: 0–40 = 1, 41–60 = 2, 61–80 = 3 and 81–100 = 4, with higher scores indicating a more positive experience.^ 18,19 ^ We reversed items with increasing scores, indicating positive experience before calculating the total score, summing all individual four-point items, and expressed as a percentage. All 22 items (19 Likert items, three converted VAS items) were summed for a total score (minimum 22, maximum 88) and expressed as a percentage. Based on the CEQ2 manual and aligning with the four-point Likert scale, having a median of 50%, we classified CEQ2 scores >50% as negative childbirth experience and ≤50% as positive childbirth experience.^ 18,19 ^
We used the Stressful Life Event Screening Questionnaire to assess stressful life events experienced by mothers throughout their lives. This 13-item questionnaire includes binary (yes/no) responses, and a higher scores indicate greater exposure to stressful life events.^ 20 ^ Moderate-to-high stress was defined as scores ≥4. To measure self-esteem, we used the Rosenberg Self-Esteem Scale (RSE), a ten-item scale with four response options (strongly agree, agree, strongly disagree, disagree). We reversed negative items and calculated the total score by summing all individual four-point items, with higher scores indicating higher self-esteem.^ 21 ^ We defined low self-esteem as scores ≤14.^ 22 ^ We pre-tested the instruments for comprehension; however, formal validation of the CEQ2 in Ghana was not performed.
Data analysis
Quantitative data analysis
We summarised background characteristics of mothers by using frequency and proportions for categorical variables, whereas median and interquartile interval (IQI) were used for continuous variables. We used the Pearson chi-squared test or Fisher’s exact test, as appropriate, to assess the association of potential factors associated with PPDS. To develop a parsimonious model of factors independently associated with PPDS, variables with a P-value less than or equal to 0.05 were considered as candidates for inclusion in the multivariable binomial generalised linear model (GLM). Variables were removed if P-values were larger than 0.1. We chose the binomial GLM with a log-link to estimate the prevalence ratio because the odds ratio would overestimate the effect owing to the high prevalence of PPDS in our sample. Missing responses were rare (i.e. one item-nonresponse) because of electronic validation checks; analyses were performed on complete cases. All analyses were performed using Stata 18 MP for macOS.
Qualitative analysis and trustworthiness (COREQ: items 24–28; reporting 29–32)
We used reflexive thematic analysis following Braun and Clarke’s six steps: (1) familiarisation with data, (2) generation of initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes and (6) writing the report.^ 23 ^ Interviews (n = 2) were recorded in the local language (Ewe) and translated into English. All interviews were transcribed verbatim, and detailed notes were compiled, ensuring that all responses were labelled with unique participant identifiers. After familiarisation with the interview data, transcripts and notes, L.T. developed a coding framework. L.T. coded the data systematically, tagging relevant sections with descriptive codes, combining inductive development of data-driven codes with deductive attention to constructs identified a priori from the literature and the quantitative findings. These codes were then grouped into broader themes. A.S. independently reviewed a subset of the transcripts, and discrepancies were discussed with A.D.J., J.H. and S.B. until interpretive consensus was reached. Finally, L.T. synthesised the results into a coherent narrative, highlighting key themes illustrated by representative maternal quotes. We managed data and coding using Dedoose version 9.0 for macOS (Sociocultural Research Consultants, LLC, Los Angeles, California, USA; see https://www.dedoose.com).
We provided an excerpt of the coding tree with definitions and example quotations in Supplementary Table 2. We assessed credibility through integration with the quantitative results. We compared statistically significant factors with emergent qualitative themes, via a joint display and narrative, to interpret how these findings corroborate or extend one another.^ 12 ^ Although member-checking of full findings with participants was not undertaken to reduce burden, we incorporated in-interview summaries and clarification probes, and we present diverse and negative cases alongside the major themes to support dependability and confirmability. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplementary Table 3) in reporting the cross-sectional component,^ 24 ^ whereas the qualitative findings followed the COREQ checklist^ 25 ^ (Supplementary Table 4).
Results
Background characteristics of mothers
We approached 405 mothers, of whom five were excluded (one mother was under 18 years of age, and four mothers had a child younger than 12 months), giving an eligibility rate of 98.8%. Of the 400 mothers who participated in the survey, one had no survey data, leaving a total of 399 (99.8%) for analysis. For these, the median age was 30 years (IQI: 26.0–34.0). Two-thirds (n = 260, 65.0%) had at least a secondary education, 323 (80.8%) were engaged in paid work (including self-employment) and 343 (86.0%) were married (Table 1). Furthermore, 120 (30.1%) had a history of depressive or psychiatric disorder (Table 2). In total, 75 (18.8%) women had a baby with complications at birth (Table 3).
Table 1. Sociodemographic and social characteristics of mothers who gave birth within the past 12 monthsCharacteristicsNumber ofparticipants(% of total) N 400Age (years), median (IQI)30 [26–34]Age group (years) 18–2468 (17.0) 25–34259 (64.8) ≥3573 (18.2)Education None/primary140 (35.0) Secondary or higher260 (65.0)Occupation Employed (formal/self)323 (80.8) Unemployed77 (19.2)Location Urban380 (95.2) Rural19 (4.8)Marital status In union344 (86.0) Not in union56 (14.0)Religion Christian378 (94.5) Other22 (5.5)Partner support Supportive353 (88.5) Unsupportive46 (11.5)History of depressive/ other psychiatric disorder No279 (69.9) Yes120 (30.1)Family history of psychiatric illness No381 (95.5) Yes18 (4.5)IQI, interquartile interval.
Table 2. Maternal characteristics of mothers who gave birth within the past 12 monthsCharacteristicsNumber of participants(% of total)Current pregnancy planned Yes227 (56.9) No172 (43.1)Type of pregnancy Singlet pregnancy381 (95.5) Multiple pregnancy18 (4.5)Parity Primiparity164 (41.1) Multiparity235 (58.9)Body mass index (BMI) Obese116 (29.1) Overweight126 (31.6) Healthy weight147 (36.8) Underweight10 (2.5)Self-esteem (RSE) Normal/high self-esteem372 (93.2) Low self-esteem27 (6.8)Childbirth experience (CEQ2) Positive childbirth experience90 (22.6) Negative childbirth experience309 (77.4)Stressful life event Low stress exposure368 (92.2) Moderate/high stress exposure31 (7.8)Obstetric complications No231 (57.8) Yes169 (42.2)History of medical condition No372 (93.0) Yes28 (7.0)RSE, Rosenberg Self-Esteem Scale; CEQ2, Childbirth Experience Questionnaire version 2.
Table 3. Characteristics of babies born to mothers who gave birth within the past 12 monthsCharacteristicsNumber of participants(% of total)Gender of the baby Male206 (51.6) Female193 (48.4)Baby had complications at birth No325 (81.2) Yes75 (18.8)Gestation Term363 (91.0) Preterm36 (9.0)Baby admitted to hospital within the past 6 weeks No378 (94.7) Yes21 (5.3)Baby has difficulty in breastfeeding No383 (96.0) Yes16 (4.0)Baby has difficulty in sleeping No376 (94.2) Yes23 (5.8)Birth weight (medium/IQI)3 [3–4]Birth weight Normal356 (89.2) Low43 (10.8)IQI, interquartile interval.
Prevalence and factors associated with PPDS
Of 399 mothers, 117 (29.3%) screened positive for PPDS (Table 4). The multivariable binary regression results showed that several demographics, psychosocial and perinatal factors were independently associated with PPDS (Fig. 1, Tables 4 and 5). Being unmarried was associated with an increased risk of developing PPDS (adjusted prevalence ratio (aPR) 1.33, 95% CI 1.02–1.72; P = 0.034). Additionally, lack of partner support was linked with a higher likelihood of developing PPDS (aPR = 1.60, 95% CI 1.21–2.12; P = 0.001) (Table 4). A history of depressive or psychiatric disorder was also associated with PPDS (aPR = 2.44, 95% CI 1.84–3.25; P < 0.001) (Table 4). Furthermore, unplanned pregnancy (aPR = 1.63, 95% CI 1.18–2.25; P = 0.003) and low self-esteem was associated with an increased risk of PPDS (aPR = 2.38, 95% CI 1.79–3.16; P < 0.001) (Table 5). Finally, low birth weight was also associated with a higher risk of PPD (aPR = 1.87, 95% CI 1.33–2.65; P < 0.001) (Table 5).
Table 4. Sociodemographic and social factors of postpartum depression among mothers who gave birth within the past 12 monthsAssociated factorsNumber (%) screenedpositive for postpartumdepressionUnivariable modelMultivariable modelPrevalence ratio[95% CI] P-valuePrevalence ratio[95% CI] P-valueOverall prevalence [95% CI]117 (29.3)[25.1–34.0]Age group (years) 18–2428 (41.2)Reference 25–3471 (27.5)0.67 [0.47–0.95]0.023 ≥3518 (24.7)0.60 [0.37–0.98]0.041Education None/primary51 (36.7)Reference Secondary or higher66 (25.4)0.69 [0.51–0.94]0.017Occupation Employed (formal/self)88 (27.3)Reference Unemployed29 (37.7)1.38 [0.98–1.93]0.063Location Urban107 (28.2)Reference Rural10 (52.6)1.87 [1.18–2.95]0.007Marital status In union90 (26.2)ReferenceReference Not in union27 (48.2)1.84 [1.33–2.54]<0.0011.33 [1.02–1.72]0.034Partner support Supportive85 (24.1)ReferenceReference Unsupportive32 (69.6)2.89 [2.21–3.77]<0.0011.60 [1.21–2.12]0.001History of depressive or other psychiatric disorder No51 (18.3)ReferenceReference Yes66 (55.0)3.01 [2.24–4.05]<0.0012.44 [1.84–3.25]<0.001
Table 5. Maternal and paediatric factors of postpartum depression among mothers who gave birth within the last 12 monthsAssociated factorsNumber (%) screened positivefor postpartum depressionUnivariable modelMultivariable modelPrevalence ratio [95% CI] P-valuePrevalence ratio [95% CI] P-valueCurrent pregnancy planned Yes41 (18.1)ReferenceReference No76 (44.2)2.45 [1.77–3.38]<0.0011.63 [1.18–2.25]0.003Type of pregnancy Singlet pregnancy108 (28.4)Reference Multiple pregnancy9 (50.0)1.76 [1.08–2.88]0.023Self-esteem (RSE) Normal/high self-esteem93 (25.0)ReferenceReference Low self-esteem24 (88.9)3.56 [2.85–4.44]<0.0012.38 [1.79–3.16]<0.001Childbirth experience (CEQ2) Positive childbirth experience79 (24.8)Reference Negative childbirth experience38 (46.9)1.89 [1.40–2.55]<0.001Stressful life event Low stress exposure102 (27.7)Reference Moderate/high stress exposure15 (48.4)1.75 [1.17–2.60]0.006Obstetric complications No56 (24.4)Reference Yes61 (36.1)1.48 [1.09–2.01]0.011Baby had complications at birth No87 (26.9)Reference Yes30 (40.0)1.49 [1.07–2.07]0.018Birth weight Normal97 (27.3)ReferenceReference Low20 (46.5)1.71 [1.19–2.45]0.0041.87 [1.33–2.65]<0.001RSE, Rosenberg Self-Esteem Scale; CEQ2, Childbirth Experience Questionnaire version 2.
Fig. 1. Forest plot of factors independently associated with postpartum depression.
Qualitative findings
We conducted 19 in-depth interviews with mothers experiencing depressive symptoms to explore how various factors contribute to PPDS within the context of their lived experiences. The background characteristics of interview participants is presented in Supplementary Table 5. Our analysis identified four key themes that highlight the interconnected social, psychological and emotional pathways through which these factors influence PPDS. The themes included (a) social isolation and limited support, (b) emotional stress and vulnerability, (c) self-image and identity challenges, and (d) resilience resources.
Social isolation and limited support
Women frequently described experiencing profound social isolation because of a lack of physical, emotional and financial support from their partners. Some mothers shared feelings of abandonment during critical moments such as labour, delivery and postpartum recovery, as their husbands were often absent. One mother remarked, ‘He wasn’t there when I needed him most, especially during labour and those first few weeks after birth’ (P01, 34 years, married). Emotional unavailability from partners further compounded feelings of loneliness, as mothers struggled to deal with the challenges of motherhood without a confidant. As one mother reflected, ‘I needed someone to talk to, someone to understand how I feel, but my partner just wasn’t there emotionally’ (P02, 32 years, cohabiting). This lack of emotional support often left mothers overwhelmed, showing their sense of helplessness during recovery and newborn care.
Financial strain also contributed to feelings of isolation and vulnerability, particularly for unmarried mothers. One unmarried mother shared, ‘I’m unmarried, and my partner doesn’t provide enough. I feel like I’m carrying everything on my own’ (P11, 27 years, not in union), and another, who was breastfeeding twins, lamented, ‘My partner barely supports us financially. I feel overwhelmed and alone’ (P03, 42 years, married). These challenges often left mothers without the essential support they needed, increasing their susceptibility to mental and emotional distress.
For unmarried mothers, the isolation was exacerbated by societal criticism of being unmarried before giving birth. Many spoke of judgement, shame, rejection and stigma because of social expectations of marriage before motherhood and experiences of rejection by their own family. One mother revealed, ’Society expects us to marry first, then have children. Because I didn’t, people insult me. It hurts me every day’ (P18, 22 years, not in union), and another shared, ‘My family said I’m a disgrace for giving birth without being married. It makes me feel so alone and ashamed. (P11, 27 years, not in union).
Some women expressed being confronted with family disappointment, which deepened their feelings of failure, as one mother explained, ‘My family said I disappointed them because I got pregnant before finishing school. They made me feel like a failure’ (P19, 20 years, not in union). Younger mothers also experienced social exclusion, often feeling judged and alienated by their peers. One younger mother explained, ‘When I got pregnant at 19, my friends started avoiding me. They insulted me, and I felt ashamed’ (P05, 19 years, cohabiting). This distancing by friends intensified feelings of loneliness and social exclusion.
Emotional distress and vulnerability
Mothers described emotional distress, often exacerbated by the lack of support, the demands of caregiving and the physical recovery process. These challenges were particularly pronounced among mothers with a history of mental health conditions. Many mothers recounted, ‘I’ve had depression before, but this time it feels worse because my family has rejected me, and I’m doing everything alone’ (P05, 19 years, cohabiting). Moreover, many mothers described how pre-existing mental health challenges resurfaced during the postpartum period, intensified by the emotional and physical demands of motherhood. One mother reflected, ‘I was already struggling mentally before I got pregnant. After the baby came, it became worse because I had no one to talk to’ (P06, 31 years, separated).
Self-image and identity challenges
Mothers frequently described emotional strain linked to feelings of self-blame, guilt and anxiety about the way of cared for their babies. For some, this manifested as persistent worry about their child’s health. One mother reflected, ‘I felt like it was my fault, like I hadn’t done enough to take care of myself during pregnancy. I kept wondering if my baby would ever catch up’ (P07, 30 years, married). Another mother shared the emotional toll of her baby’s stay in the neonatal intensive care unit (NICU), saying, ‘My baby was in the NICU, and I couldn’t see him for 3 days. I kept thinking he wouldn’t survive, and it broke me’ (P08, 27 years, married). Physical changes following childbirth further compounded these struggles, with many mothers reporting diminished self-esteem and feelings of unattractiveness owing to postpartum weight gain and other bodily changes. One mother explained, ‘I look at my body now, and I don’t recognise myself. It makes me feel unattractive and unworthy’ (P10, 28 years, married). The caregiving challenges and low self-esteem, particularly among mothers of low-birthweight babies, contributed to heightened anxiety, self-blame and feelings of failure.
Moreover, some women compared their perceived shortcomings to the successes of their peers, which intensified feelings of inferiority. As one mother explained, ‘I see my friends doing so well, and I feel like I’m struggling just to get through the day. It makes me feel like I’ll never be good enough’ (P12, 39 years, cohabiting). These narratives underscore the impact of negative self-perception on mothers’ emotional well-being, increasing their vulnerability to postpartum depression.
Resilience resources
Many mothers exhibited resilience in the presence of postpartum struggles. Despite a lack of support, some mothers expressed resilience and determination to raise their babies. For instance, one mother stated, ‘Even though I am alone in this, I find joy in caring for my baby. Every moment I spend with her makes me feel complete. I may not have support, but I will not let that affect her well-being’ (P11, 27 years, not in union).
Furthermore, some mothers found moments of healing and emotional renewal through their connection with their babies. For some, the experience of caring for their child brought a sense of purpose and improved their mental well-being. One mother remarked, ‘After birth, I felt better. Even though the depression had set in, holding my baby and caring for him brought me a sense of peace and purpose. I felt I could do it, despite my history of depression’ (P12, 39 years, cohabiting). Similarly, others found solace in the support of family members and healthcare workers. This support included emotional encouragement from nurses during hospital visits and practical help from family (e.g., a relative caring for the infant or household duties), which mothers said gave them strength. A participant shared that, ‘The support from the nurses and my family helped me feel strong again. I began to find joy in motherhood despite my history’ (P13, 21 years, married).
Other mothers also expressed a sense of pride and self-worth as they came to appreciate their postpartum body. One mother remarked, ‘It took time, but I’m starting to appreciate my body for what it has done. I carried life, and that makes me proud’ (P14, 28 years, married). Encouragement from partners also played a role in fostering emotional resilience, as one mother shared, ‘My partner reminded me every day that I looked beautiful even with the stretch marks. It helped me see myself differently, not just for how I looked but for what my body had accomplished’ (P15, 31 years, cohabiting). Although some mothers remain deeply affected by social and emotional vulnerabilities, others find pathways to healing and resilience through meaningful connections and support systems.
Integration of findings
We combined the quantitative and qualitative results. We found that factors that were significantly associated with PPDS (i.e. highest aPRs and P < 0.05) aligned with mothers’ narratives. For example, lack of partner support (aPR = 1.60) corresponded closely to the ’social isolation and limited support’ theme, and low self-esteem (aPR = 2.38) matched the ’self-image and identity challenges’ theme. Conversely, qualitative themes such as personal resilience added context beyond the survey. In this way, meta-integration showed that the main statistical correlates were echoed in lived experiences, reinforcing their importance.
Discussion
Main findings
Our findings showed a high PPDS prevalence of 29.3%, with key factors including being unmarried, lack of partner support, history of depressive or psychiatric disorders, unplanned pregnancy, low self-esteem and low-birth-weight infants. In-depth interviews further identified themes of social isolation, emotional stress, self-perception challenges and resilience. These offer insights into the mechanisms linking these factors to PPDS. Our results highlight the need for robust support systems and culturally sensitive interventions to prevent and reduce PPDS.
Strengths and limitations
We combined quantitative analysis with rich qualitative insights, which provided a comprehensive understanding of these factors and mechanisms of PPDS. We used validated and practical psychometric instruments like the PHQ-9. However, the cross-sectional design limits determining causality. Also, our sample was predominantly urban (95%), reflecting the facility locations in Ho. This urban bias may limit generalisability to rural Ghana; rural mothers often face additional stressors and access barriers. Future research should also include rural communities to capture potential differences. Additionally, social desirability bias may have influenced responses on sensitive topics. Although the PHQ-9 has shown acceptable psychometric properties in Ghana (Cronbach’s alpha = 0.75),^ 21 ^ not all instruments (e.g. CEQ2, Rosenberg Self-Esteem Scale) were validated in Ewe. Translation issues arising from a lack of cultural adaptation may have introduced measurement error, which we cannot completely rule out. Again, our sample excludes mothers who do not attend postnatal clinics (for example, those giving birth at home or dropping out of care). This may bias results if such women have different PPDS rates.
Interpretation
The prevalence of PPDS in our study is higher than the African average (22.1%) and previous estimates in Ghana (20.3%),^ 1,2 ^ suggesting potential contextual factors that increase vulnerability. Regional differences in Ghana showed lower PPDS in the Northern region (16.8%)^ 26 ^ and higher PPDS in the Ashanti region (31.4%),^ 27 ^ influenced by variations in healthcare systems, cultural norms and support structures.^ 28 ^ For example, extended family support in rural areas like the Northern region may offer protection against PPDS,^ 29 ^ whereas urbanisation in the Ashanti region, despite its development, contributes to reduced family support, increased work–family pressures and social isolation.^ 30 ^ In Ghana’s urbanised context, nuclear family living and changing gender roles may reduce traditional family support for new mothers. Additionally, in migration studies, Volta migrants depend heavily on family ties, whereas Northern migrants rely more on friends,^ 31 ^ reflecting distinct social networks. These socio-structural differences (including Volta’s proximity to Accra versus Northern Ghana’s remoteness) may affect support for mothers and thus help explain the regional prevalence patterns of PPDS that were observed. These findings underscore the importance of tailoring PPDS interventions to specific regional contexts.
Our findings suggest that PPDS among mothers in Ghana is influenced by a combination of sociodemographic, psychological, maternal and perinatal factors, with qualitative analyses highlighting pathways through which these factors exert their influence. Consistent with previous studies, key factors associated with PPDS include being unmarried, lack of partner support, history of depression or psychiatric disorders, unplanned pregnancy,^ 5 ^ low self-esteem^ 6 ^ and low birth weight.^ 7 ^ Being unmarried and experiencing unplanned pregnancies heightened feelings of societal isolation and inadequacy, reflecting cultural norms that stigmatise unmarried mothers.^ 32 ^
Our results align with Ghana’s patriarchal family norms, which emphasise that women should marry and bear children.^ 33 ^ In this context, an adolescent or unmarried pregnancy is widely viewed as shameful. Indeed, local qualitative studies report that unmarried pregnant adolescents are often verbally abused or ostracised by family and neighbours.^ 32,34 ^ The absence of partner support left mothers feeling isolated, emotionally strained and financially burdened, reinforcing the protective role of partner involvement in reducing emotional distress and improving maternal mental health.^ 35 ^
Qualitatively, we also observed that low self-esteem and caregiving challenges, particularly among mothers of low-birth-weight babies, contributed to heightened anxiety, self-blame and feelings of failure. This is consistent with a previous study highlighting the psychological distress caused by added caregiving demands^ 7 ^ and body image concerns. Societal expectations of motherhood further contributed to negative self-image and inadequacy.^ 36 ^ Many mothers exhibited resilience in the presence of PPDS. Some mothers found strength through body acceptance^ 11 ^ and displayed resilience as a result of emotional connection with their babies and support from family and healthcare workers.^ 37 ^ Other possible factors that promote resilience may include individual coping strategies, social support networks and cultural or spiritual beliefs. In our interviews, mothers who reported higher resilience often mentioned faith, encouragement from family or finding purpose in motherhood. Altogether, these findings underscore the dual nature of postpartum experiences, balancing adversity with opportunities for emotional growth. They also emphasise the need for culturally sensitive interventions, combining structural support, such as antenatal and postnatal classes, with psychological care to enhance resilience and reduce the burden of PPDS.^ 38 ^
Our findings have implications for Ghana’s health sector, informing public health policy, clinical practice and future research. At the policy level, it is essential to integrate maternal mental health services into existing maternal and child health programmes. This aligns with Ghana’s mental health policy, which advocates mental health integration into primary care. To leverage identified resilience factors, we recommend couple-based antenatal education (to involve partners in pregnancy care) and mother-to-mother support networks. Specifically, implementing partner-inclusive counselling and creating peer-mentor schemes could harness family and community support.^ 39 ^ Evidence shows that peer-support groups improve maternal mental health outcomes.^ 40 ^ Embedding such programmes within existing maternal health services could enhance the social support infrastructure for at-risk mothers.^ 38 ^ Clinically, maternal health service providers should implement routine screening for postpartum depression at postnatal visits and offer psychosocial support or referrals for mothers at high risk, such as those with prior psychiatric history or low social support. Future research should include longitudinal studies to validate these risk factors over time and the design of targeted interventions (such as partner-inclusive counselling or resilience-building programmes) to determine effective strategies for reducing the burden of postpartum depression in diverse Ghanaian settings.
In conclusion, PPDS were common in our sample and were significantly associated with modifiable factors such as prior mental health history and low self-esteem. These findings underscore the importance of prioritising maternal mental health through integration of depression screening and psychosocial care into routine antenatal and postnatal services, with particular support for high-risk groups like unmarried mothers.
Supporting information
Tornyevah et al. supplementary material 1Tornyevah et al. supplementary material
Tornyevah et al. supplementary material 2Tornyevah et al. supplementary material
Tornyevah et al. supplementary material 3Tornyevah et al. supplementary material
Tornyevah et al. supplementary material 4Tornyevah et al. supplementary material
Tornyevah et al. supplementary material 5Tornyevah et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nweke M , Ukwuoma M , Adiuku-Brown AC , Okemuo AJ , Ugwu PI , Nseka E. Burden of postpartum depression in sub-Saharan Africa: an updated systematic review. S Afr J Sci 2024; 120:1–12.
- 2Keku E , Asabea S , Nti SJ , Kwamekyi A. Prevalence of postpartum depression in Ghana: a systematic review study. Sci Electron Arch 2023; 17: 65–70.
- 3Roberts M , Mogan C , Asare JB. An overview of Ghana’s mental health system: results from an assessment using the World Health Organization’s Assessment Instrument for Mental Health Systems (WHO-AIMS). Int J Mental Health Syst 2014; 8: 16.10.1186/1752-4458-8-16PMC 401665224817908 · doi ↗ · pubmed ↗
- 4Appiah-Dolphyne J . Government Expands NHIS to Cover Four Mental Health Disorders from 1 November. Asaase Radio, 2024 (https://asaaseradio.com/government-expands-nhis-to-cover-four-mental-health-disorders-from-1-november/).
- 5Agrawal I , Mehendale AM , Malhotra R. Risk factors of postpartum depression. Cureus 2022; 14: e 30898.36465774 10.7759/cureus.30898 PMC 9711915 · doi ↗ · pubmed ↗
- 6Han JW , Kim DJ. Longitudinal relationship study of depression and self-esteem in postnatal korean women using autoregressive cross-lagged modeling. Int J Environ Res Public Health 2020; 17: 3743.32466278 10.3390/ijerph 17103743 PMC 7277650 · doi ↗ · pubmed ↗
- 7Pellegrino J , Mundagowa PT , Sakyi KS , Owusu PG , Agbinko-Djobalar B , Larson LM , et al. Prevalence and risk factors for postpartum depression and stress among mothers of preterm and low birthweight infants admitted to a neonatal intensive care unit in Accra, Ghana. Int J Gynaecol Obstet 2025; 169: 131–7.39475422 10.1002/ijgo.15998 PMC 11911984 · doi ↗ · pubmed ↗
- 8Bening JE , Darko F , Anterkyi R , Narh VK , Prempeh NYA , Jain N , et al. Predictors of postpartum depression among new mothers in Kumasi, Ghana: a multicenter study using Bayesian analysis. Womens Health (Lond) 2025; 21: 17455057251343953.40478594 10.1177/17455057251343953 PMC 12144355 · doi ↗ · pubmed ↗