A NECessary Workup: Exploring the Rare Histology of an Esophageal Tumor
Ronald Koschny, Georg Martin Haag, Alexander Brobeil

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
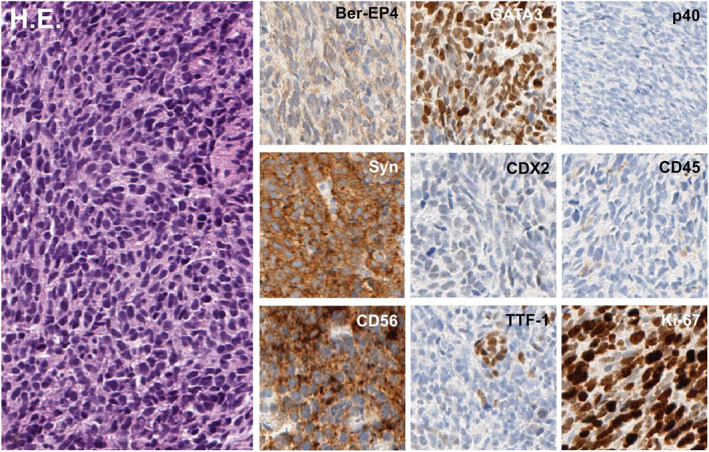 Figure 1
Figure 1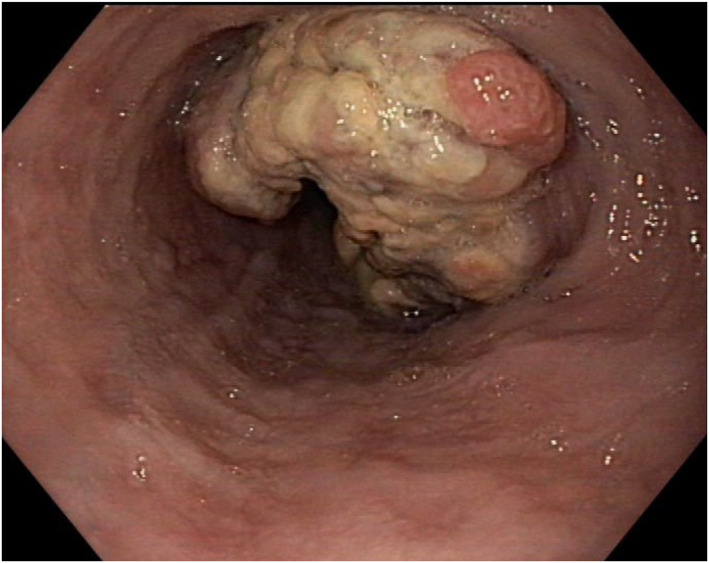 Figure 2
Figure 2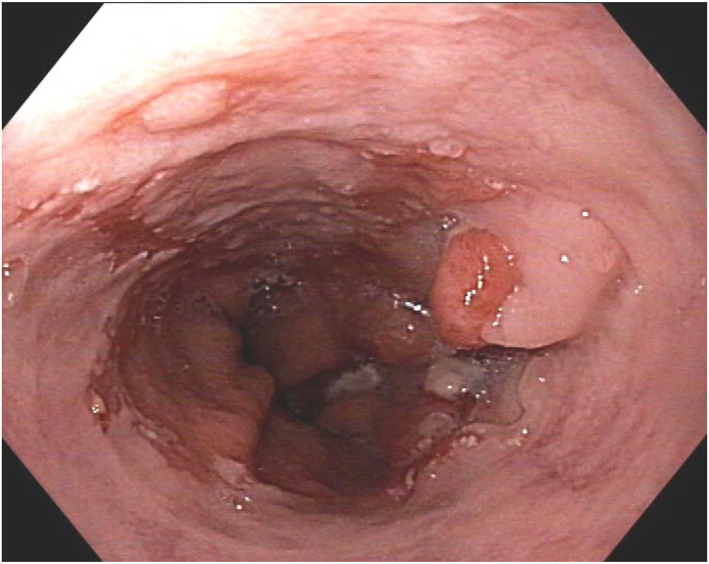 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Gastrointestinal Tumor Research and Treatment · Lung Cancer Research Studies
A 64 years old patient with melena was transferred for re‐biopsy of a suspected adenocarcinoma of the esophagogastric junction (Siewert type II) within Barrett's esophagus (C0M2) with “indeterminate dysplasia” due to insufficient external tissue sampling. The patient's comorbidities (male sex, age, obesity, smoking) supported the suspicion of Barrett's carcinoma. Figure 1 shows the endoscopic appearance of a stenosing tumor stretching from 35 to 45 cm from the incisors (Z‐line at 43 cm). Computed tomography described a T3 tumor with an increased number of morphologically non‐suspicious locoregional lymph nodes.
Histopathology of multiple re‐biopsies showed infiltrates of malignant cells positive for CD56 and synaptophysin confirming a neuroendocrine carcinoma (NEC) of the esophagus with a proliferation index (Ki67) of 90% (Figure 2). Expression of TTF1 and GATA3 raised the suspicion of a pulmonary primary. Serum chromogranin was not elevated.
After neoadjuvant treatment with two cycles of carboplatin/etoposide, the neuroendocrine carcinoma showed significant tumor shrinkage (Figure 3). The patient underwent abdomino‐thoracic esophagectomy (ypT1b ypN0 (0/11) L0 V0 G3 R0).
Undergoing continuous monitoring by CT and endoscopy, no tumor relapse occurred during a 5‐year follow‐up. Initial CT scan and long‐term follow‐up excluded a pulmonary primary of the tumor.
Primary NEC of the esophagus accounts for only 3% of esophageal neoplasms [1]. Thus, NEC is a very rare differential diagnosis of tumors of the esophagogastric junction, especially when arising within Barrett's esophagus [2, 3]. Although their etiology is unknown, a common stem cell has been suggested due to the presence of endocrine cell hyperplasia in Barrett mucosa [4]. Alternatively, NEC might arise from hyperplasia of enterochromaffin‐like cells induced by long term proton pump inhibitor use in these patients [5].
Conclusive tumor histology cannot always be obtained from inflamed and necrotic tissue. However, even in putatively clinically conclusive situations, histological classification is an indispensable prerequisite for the correct tumor diagnosis and selection of the optimal neoadjuvant treatment. This case emphasizes the importance of repeated biopsies to avoid improper treatment.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. Babu Kanakasetty , L. Dasappa , K. C. Lakshmaiah , et al., “Clinicopathological Profile of Pure Neuroendocrine Neoplasms of the Esophagus: A South Indian Center Experience,” Journal of Oncology 2016 (2016): 2402417, 10.1155/2016/2402417.27340404 PMC 4906204 · doi ↗ · pubmed ↗
- 2E. Giannetta , V. Guarnotta , F. Rota , et al., “A Rare Rarity: Neuroendocrine Tumor of the Esophagus,” Critical Reviews in Oncology 137 (2019): 92–107, 10.1016/j.critrevonc.2019.02.012.31014519 · doi ↗ · pubmed ↗
- 3P. Patel , E. A. Zaher , and H. Sqour , “High‐Grade Pure Esophageal Neuroendocrine Carcinoma Arising From Barrett's Mucosa: A Rare Phenomenon,” Cureus 15, no. 6 (2023): e 40644, 10.7759/cureus.40644.37476144 PMC 10355687 · doi ↗ · pubmed ↗
- 4M. P. Hoang , C. M. Hobbs , L. H. Sobin , and J. Albores‐Saavedra , “Carcinoid Tumor of the Esophagus: A Clinicopathologic Study of Four Cases,” American Journal of Surgical Pathology 26, no. 4 (2002): 517–522, 10.1097/00000478-200204000-00016.11914632 · doi ↗ · pubmed ↗
- 5N. R. Cary , D. J. Barron , J. P. Mc Goldrick , and F. C. Wells , “Combined Oesophageal Adenocarcinoma and Carcinoid in Barrett's Oesophagitis: Potential Role of Enterochromaffin‐Like Cells in Oesophageal Malignancy,” Thorax 48, no. 4 (1993): 404–405, 10.1136/thx.48.4.404.8511743 PMC 464444 · doi ↗ · pubmed ↗