The Empty Bladder is Preferred in Some Cases of Radiation Therapy for Rectal Cancer
Inna Ospovat, Albert Schlocker, Natan Shtraus, Ravit Geva, Shani Hazan, Tatyana Shevchuk, Alexander Barenboim, Ido Wolf, Orit Gutfeld, Viacheslav Soyfer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
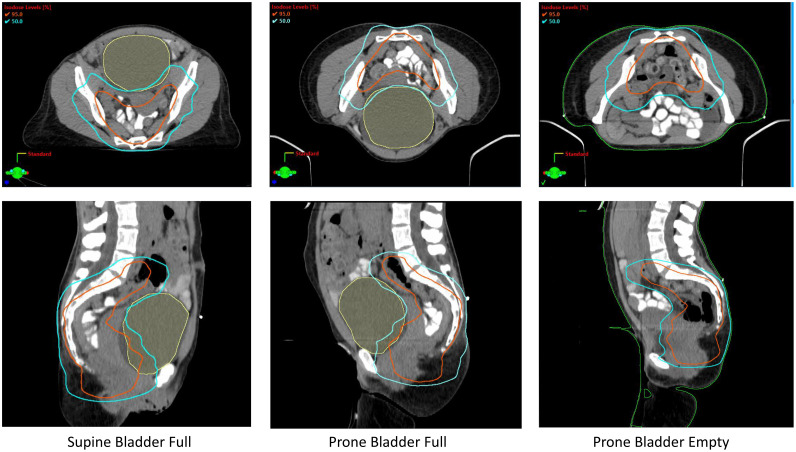 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Stoma care and complications · Anorectal Disease Treatments and Outcomes
Introduction
Radiation therapy is an integral component in the treatment of rectal cancer. Appropriate positioning of patients for the best dosimetric coverage of the treatment volumes that minimizes the irradiation of normal structures, especially avoiding the small bowel, is a primary task for physicians in the simulation and treatment planning of rectal cancer radiation therapy. Many studies on the preference for either prone or supine positioning exist in the literature. Generally, the supine position is preferable in terms of treatment reproducibility, while the prone position is better for small bowel radiation avoidance.1, 2, 3 A full bladder is usually prescribed in order to displace the attached small bowel away from the radiation treatment fields.4, 5, 6
The rectouterine space in women, called the Pouch of Douglas, is the lowest part of the abdominal cavity. In men, this low space is the rectovesical space.7 Normally, this cavity contains a small amount of peritoneal fluid. The small bowel can transiently enter this lower part of the abdominal cavity in certain situations, notably when the patient is in an upright or supine position. An increase in abdominal pressure may also cause the small bowel to translocate to the rectouterine or rectovesical space. Moreover, pelvic inflammatory disease, previous surgery, or an enlarged myomatous uterus can lead to a constant intestinal presence in these cavities. The current standard of care for radiation therapy for rectal cancer, if indicated, is administered prior to surgery, either by 3-dimensional conformal or volumetric modulated arc therapy technique.8 The treatment fields typically include the rectum and surrounding lymphatics, and according to contouring atlases, the posterior wall of the bladder or uterus is included.9
Case Description
In this clinical report, a 63-year-old otherwise healthy woman diagnosed with adenocarcinoma of the mid-rectum T3N1 was simulated for preoperative radiation therapy. Traditional measures to eliminate entrapped small bowel loops between the rectum and bowel were not effective. The standard simulation included an oral contrast in both supine and prone positioning, including the use of a belly board and a full bladder. It appeared that in both supine and prone orientations, there was a significant volume of small bowel loops entrapped behind the bladder.
A third simulation scan, with the patient prone and an empty bladder, allowed the release of small bowel anteriorly and enabled treatment planning with minimal small bowel exposure (Fig. 1).Figure 1. Volumetric modulated arc therapy treatment plans (transverse and sagittal views) discussed in the article for both supine and prone orientations, with a full and empty bladder, illustrate that for this patient, the lowest dose to the small bowel was achieved with the patient prone and an empty bladder.Figure 1
Conclusion
In summary, computed tomography simulation of rectal patients in the prone position concurrent with an empty bladder could be considered in cases when the small bowel is located in the low pelvis behind the bladder or uterus, or behind the bladder in men.
Disclosures
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Esmati E.Barzegartahamtan M.Maddah A.Alikhassi A.Vaezzadeh V.Mohammadpour R.The effect of patient positioning (prone or supine) on the dose received by small bowel in pelvic radiotherapy in rectal cancer patients Cancer Radiother 2520214194233381277810.1016/j.canrad.2020.04.013 · doi ↗ · pubmed ↗
- 2Yang Y.Cai S.Zhao T.Peng Q.Qian J.Tian Y.Effect of prone and supine treatment positions for postoperative treatment of rectal cancer on target dose coverage and small bowel sparing using intensity-modulated radiation therapy Transl Cancer Res 920204914993511739310.21037/tcr.2019.11.33PMC 8799155 · doi ↗ · pubmed ↗
- 3White R.Foroudi F.Sia J.Marr M.A.Lim Joon D.Reduced dose to small bowel with the prone position and a belly board versus the supine position in neoadjuvant 3D conformal radiotherapy for rectal adenocarcinoma J Med Radiat Sci 6420171201242774138110.1002/jmrs.187PMC 5454325 · doi ↗ · pubmed ↗
- 4Zimmermann M.Richter A.Weick S.Acute toxicities of patients with locally advanced rectal cancer treated with intensified chemoradiotherapy within the CAO/ARO/AIO-12 trial: Comparing conventional versus VMAT planning at a single center Sci Rep 1220222126310.1038/s 41598-022-25647-8PMC 973198636481692 · doi ↗ · pubmed ↗
- 5Kim T.H.Chie E.K.Kim D.Y.Comparison of the belly board device method and the distended bladder method for reducing irradiated small bowel volumes in preoperative radiotherapy of rectal cancer patients Int J Radiat Oncol Biol Phys 6220057697751593655810.1016/j.ijrobp.2004.11.015 · doi ↗ · pubmed ↗
- 6Hong T.S.Moughan J.Garofalo M.C.NRG Oncology Radiation Therapy Oncology Group 0822: A phase 2 study of preoperative chemoradiation therapy using intensity modulated radiation therapy in combination with capecitabine and oxaliplatin for patients with locally advanced rectal cancer Int J Radiat Oncol Biol Phys 93201529362616333410.1016/j.ijrobp.2015.05.005PMC 4540628 · doi ↗ · pubmed ↗
- 7Brant W.E.Helms C.A.Fundamentals of Diagnostic Radiology 2007 Lippincott Williams & Wilkins
- 8Sauer R.Becker H.Hohenberger W.Preoperative versus postoperative chemoradiotherapy for rectal cancer N Engl J Med 3512004173117401549662210.1056/NEJ Moa 040694 · doi ↗ · pubmed ↗