Recurrent Septic Shock in Immunosuppressed Patients
Shinnosuke Fukushima, Koji Fujita, Hideharu Hagiya

TL;DR
This paper discusses a case where cytomegalovirus enteritis caused recurring septic shock in an immunosuppressed patient.
Contribution
The paper highlights the need to consider cytomegalovirus enteritis in the differential diagnosis of recurrent septic shock in immunocompromised patients.
Findings
Cytomegalovirus gastroenteritis can present with subtle symptoms in immunosuppressed individuals.
Histopathological examination via endoscopy is crucial for diagnosis.
The condition can lead to septic shock, necessitating early recognition.
Abstract
Cytomegalovirus gastroenteritis presents with diarrhea and abdominal pain in immunosuppressed patients, and histopathological examination is essential by endoscopy. This case illustrates that cytomegalovirus enteritis may develop insidiously and possibly invoke shock in immunocompromised patients, warranting its inclusion in the differential diagnosis of recurrent septic shock.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
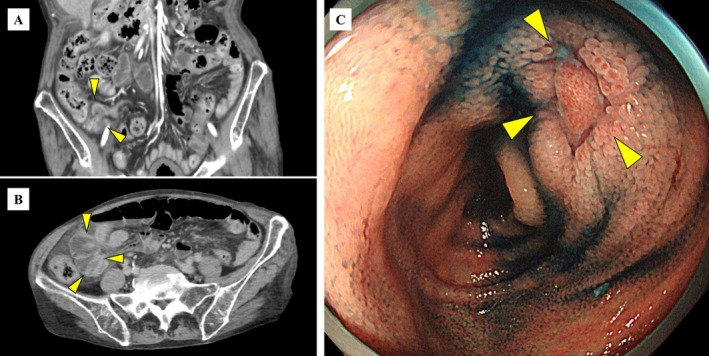 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Bacterial Infections and Vaccines · Infectious Encephalopathies and Encephalitis
A 70‐year‐old woman with rheumatoid arthritis presented with fever and was admitted to our hospital. Her medication included prednisolone 4 mg daily and iguratimod, with a notable history of two hospitalizations within the preceding 2 months for septic shock without bacteremia. On admission, the patient exhibited hypotension (78/34 mmHg) and hyperpyrexia (42.0°C), and cefepime was empirically initiated for septic shock. Blood cultures obtained on admission yielded Escherichia coli the following day. Contrast‐enhanced computed tomography was performed to evaluate the gastrointestinal tract as a potential source, demonstrating enteritis predominantly involving the terminal ileum (Figure 1A,B). At the time of previous septic shock 1 month ago, colonoscopy revealed ulcerative lesions from the terminal ileum to the ileocecal valve (Figure 1C). The previous colonoscopy findings, showing a terminal ileum ulcer in an immunosuppressed patient, prompted consideration of cytomegalovirus (CMV) infection. Immunostaining was performed on the previous biopsy specimen, and CMV‐positive cells were detected, indicating that CMV enteritis was considered the etiology of recurrent septic shock. CMV antigenemia was negative at the time of admission. Ganciclovir therapy was initiated, and the patient was discharged without further episodes of infection.
CMV gastroenteritis presents with gastrointestinal bleeding, diarrhea, and abdominal pain in immunosuppressed patients [1, 2]. Because the accuracy of serodiagnosis is poor for CMV gastrointestinal tract disease, histopathological examination is essential by endoscopy [1, 2]. Intestinal ulcers are observed in 82.5% of immunosuppressed patients with CMV gastroenteritis [2], which has the potential for the development of bacteremia by bacterial translocation. In immunocompetent critically ill patients of the intensive care unit, septic shock had been reported to precede CMV colitis in 92.8% of patients [3]. Our patient presented with recurrent septic shock without gastrointestinal bleeding or diarrhea, which differs from the more common manifestations of CMV enteritis reported previously [1, 2]. Elderly and immunocompromised patients are more frequently colonized by multidrug‐resistant bacteria, making these pathogens an important consideration in the differential diagnosis of recurrent sepsis; however, CMV should also be considered, as in this case. While management guidelines for CMV infection are well established in solid organ transplant recipients, confirmed recommendations for non‐HIV immunocompromised patients receiving immunosuppressive therapy for rheumatologic diseases remain lacking. This case illustrates that CMV enteritis may develop insidiously and possibly invoke shock in immunocompromised patients, warranting its inclusion in the differential diagnosis of recurrent septic shock.
Author Contributions
Shinnosuke Fukushima: conceptualization, writing – original draft. Koji Fujita: writing – review and editing. Hideharu Hagiya: writing – review and editing.
Ethics Statement
This case report was reviewed and considered exempt from full Institutional Review Board approval according to our institution's guidelines.
Consent
Written informed consent was obtained from the patient for the publication.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1P. J. Yeh , R. C. Wu , C. L. Chen , et al., “Cytomegalovirus Diseases of the Gastrointestinal Tract in Immunocompetent Patients: A Narrative Review,” Viruses 16, no. 3 (2024): 346.38543712 10.3390/v 16030346 PMC 10975113 · doi ↗ · pubmed ↗
- 2T. Chaemsupaphan , J. Limsrivilai , C. Thongdee , et al., “Patient Characteristics, Clinical Manifestations, Prognosis, and Factors Associated With Gastrointestinal Cytomegalovirus Infection in Immunocompetent Patients,” BMC Gastroenterology 20, no. 1 (2020): 22.32000707 10.1186/s 12876-020-1174-y PMC 6990526 · doi ↗ · pubmed ↗
- 3R. F. Siciliano , J. B. Castelli , B. A. Randi , R. D. Vieira , and T. M. Strabelli , “Cytomegalovirus Colitis in Immunocompetent Critically Ill Patients,” International Journal of Infectious Diseases 20 (2014): 71–73.24406737 10.1016/j.ijid.2013.11.008 · doi ↗ · pubmed ↗