Complex port removal: balloon-assisted retrieval of retained intravascular catheters – a technical note
Nicholas L. Thomas, Coplen D. Johnson, Christopher Stevens, Joseph Eskew, Chiranjiv Virk, Chaitanya Ahuja, Paul E. Perkowski, Heba Fouad

TL;DR
A balloon-assisted technique effectively removes difficult-to-extract long-term port-a-cath catheters with complications like fibrosis and calcification.
Contribution
Demonstrates balloon-assisted retrieval as a primary method for removing complex retained port-a-caths.
Findings
Balloon-assisted retrieval successfully removed 12 retained port-a-cath catheters with fibrotic and calcified adhesions.
The technique caused minimal blood loss and no complications in all cases.
It is effective for catheters with stenosis and should be considered a primary retrieval option.
Abstract
Balloon dilatation has remained relatively underutilized despite its emerging potential for hemodialysis catheter removal. This case series revisits balloon-assisted retrieval to showcase its effectiveness in retrieving long-term port-a-caths complicated by fibrotic encapsulation, calcification, and stenosis. Endoluminal balloon-assisted retrieval was utilized in 12 cases with retained port-a-cath catheters after gentle traction failed to remove the indwelling 8 French catheter due to complex intravascular fibrotic adhesions and calcifications. Under fluoroscopic guidance, a non-compliant angio-balloon was advanced over a guidewire through the externally accessible central venous catheter. Once the balloon reached the distal segment of the tubing, it was sequentially inflated in a retrograde manner within the catheter's lumen to disrupt the surrounding adhesions. Balloon-assisted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
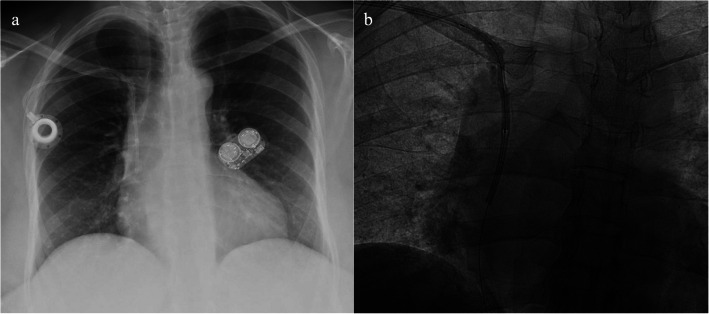 Figure 1
Figure 1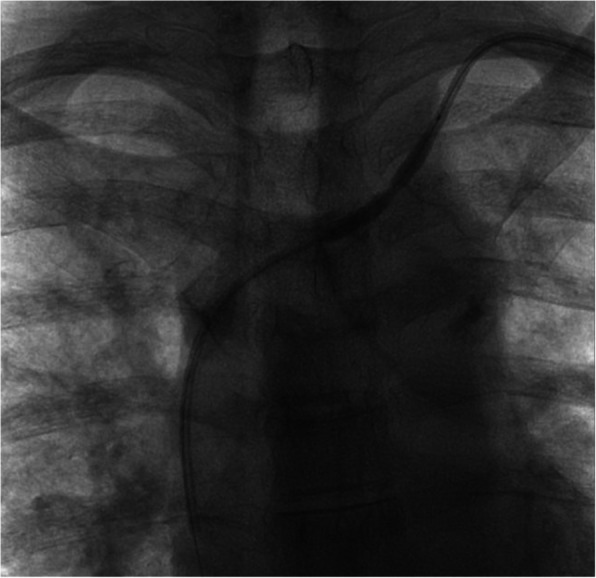 Figure 2
Figure 2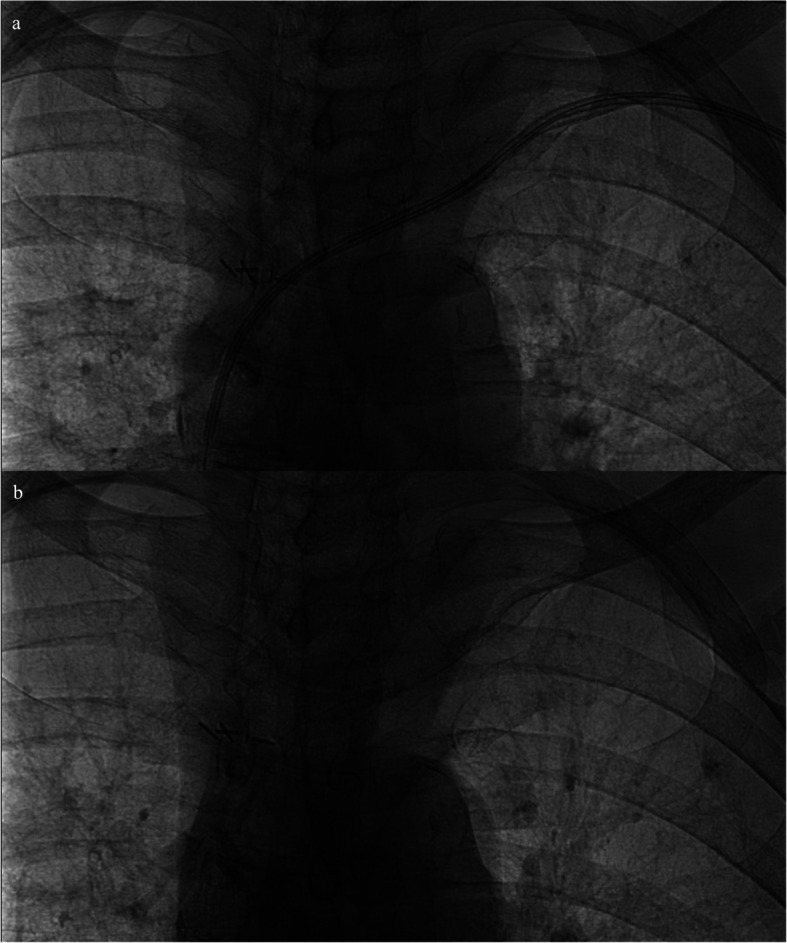 Figure 3
Figure 3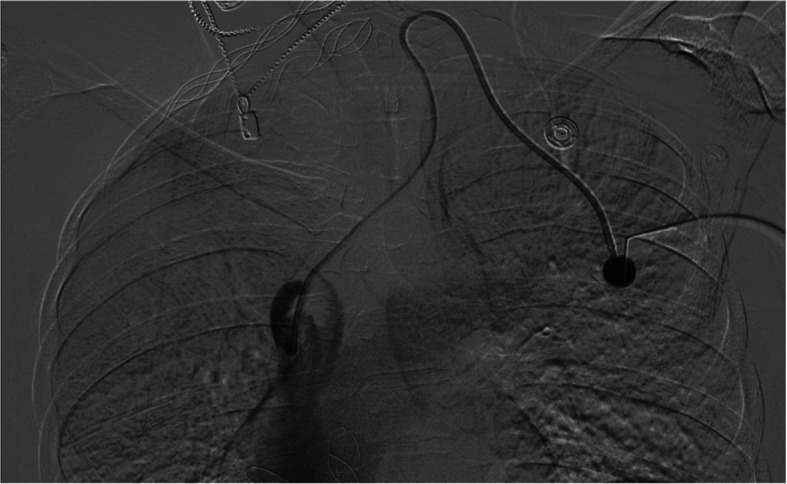 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Vascular Procedures and Complications · Acute Kidney Injury Research
Introduction
Central venous catheterization (CVC), such as the port-a-cath, is a common method of vascular access for chronically ill patients requiring long-term therapy. However, prolonged catheterization increases the risks of infection, catheter/vessel thrombosis, and stenosis due to fibrin sheath formation [1]. Therefore, prompt removal of long-term catheterization is necessary once it is no longer needed.
While gentle catheter traction remains the standard removal technique, long-term catheterization with adhesions and/or calcifications can complicate this process, often necessitating an advanced procedure [1]. In instances where catheter removal is complicated, open surgical removal was previously warranted, as forceful catheter removal could result in fragmentation, embolization, and potentially life-threatening vessel and atrial tearing [2]. However, in 2011, endoluminal balloon dilatation was introduced as a method to free fibrosed hemodialysis catheters from their endovascular adhesions [3]. This innovative technique enabled the safe and effective retrieval of retained catheters with complex adhesions and calcifications [3, 4].
Inspired by this approach, we implemented endoluminal balloon-assisted retrieval as the primary technique for extracting externally accessible retained port catheters. This manuscript adds to the expanding documentation supporting this technique and emphasizes its potential as a primary method for removing retained port-a-caths, particularly in cases involving complex fibrin sheath formations and calcifications.
Materials & methods
From January 2019 to October 2024, twelve patients with long-term port-a-caths underwent endoluminal balloon-assisted retrieval (Table 1). All were diagnosed with retained catheters during port-a-cath removal after gentle traction failed to retrieve the CVC tubing from the vascular tree. All retained catheters were externally accessible, which reduced costs, risks, procedural steps, and time to completion, as we did not require additional percutaneous access. Three cases were identified at an outside hospital after the port was removed via blunt dissection and were subsequently referred to our hospital. Table 1. Patient case and central venous catheter details upon presentationCasePatient AgePatient SexReason for CatheterizationType of CatheterSide of PortAge of CatheterPort Present^a^Case 156FLupus and SclerodermaPort-a-CathRight15 yearsNoCase 273FRight-Sided Breast CancerPort-a-CathLeft8 yearsNoCase 361FLupus and Rheumatoid ArthritisPort-a-CathLeft12 yearsNoCase 461FMetastatic NSCLC AdenocarcinomaPort-a-CathRight11 yearsYesCase 555FSickle Cell DiseasePort-a-CathLeft16 yearsYesCase 644MSickle Cell DiseasePort-a-CathLeft14 yearsYesCase 743FSickle Cell DiseasePort-a-CathRight10 yearsYesCase 871FBilateral Breast CancerPort-a-CathLeft14 yearsYesCase 940MNon-Hodgkin’s LymphomaPort-a-CathLeft9 yearsYesCase 1021FGaucher’s Disease Type 3Port-a-CathRight18 yearsYesCase 1166MGastric LymphomaPort-a-CathRight29 yearsYesCase 1249FCalcium Gluconate InfusionsPort-a-CathLeft15 yearsYes^a^Some ports were removed at an outside hospital and pericatheter adhesions were identified at that time
Upon arrival at the angio-suite and under sterile conditions, we performed a preliminary fluoroscopic evaluation to visualize the retained catheter and surrounding adhesions in the vascular tree (Fig. 1a). We would then attempt removal of the catheter via manual pulling to confirm the necessity for balloon-assisted retrieval. After identifying the retained catheter, we advanced a guidewire into the lumen of the external portion of the catheter tubing. We then advanced a non-compliant balloon over the wire, entering the lumen until we reached the distal end of the catheter tubing, past the identified adhesions, as confirmed by fluoroscopy (Fig. 1b).Fig. 1a: preoperative PA chest x-ray demonstrating right-sided chest port with a subclavian tunneled catheter and pericatheter calcifications along its course through the superior vena cava; b: intraoperative fluoroscopy demonstrating angioplasty with a 3 mm balloon as it disrupts the calcified adhesions to allow for removal of the catheter in its entirety without fragmentation
Once we visualized the balloon at the distal end of the retained catheter, we performed serial dilatation and deflation from the distal end back to the external end of the tubing (Fig. 2). Because of their increased endoluminal surface area, longer-length balloons required fewer dilatations to expand the entire length of the tubing, while shorter-length balloons required more dilatations. After disrupting the fibrotic encapsulations and calcifications, we could safely extract the catheter in its entirety with gentle traction (Fig. 3). Our institution has shifted preference towards longer balloons for this reason; however, it still depends on the availability of balloons in the procedural suite.Fig. 2. Intraoperative fluoroscopy demonstrating angioplasty of a left-sided central venous catheter with adhesions to the vessel wall of the left brachiocephalic and internal jugular vein; a waist is noted in the midportion of the balloon, demonstrating a segment of stenosis secondary to pericatheter adhesionsFig. 3a Intraoperative fluoroscopy during angioplasty of a left-sided port-a-cath demonstrating the radio-opaque markers used to visualize the edges of the balloon; b postoperative fluoroscopy demonstrating the residual calcifications along the walls of the left innominate vein after the removal of the catheter in its entirety
When comparing the technical aspects of the cases, we utilized ten different non-compliant balloons and two types of guidewires (Table 2). The lengths of the balloons and sizes of the guidewires were determined by what was readily available in the procedure suite or by physician preference. The balloon diameter was determined by the estimated size needed to disrupt surrounding adhesions and calcifications. The largest balloon in this series was 6.0 mm, which was used after a 5.0 mm failed to release the catheter from the surrounding adhesions. The initial difficulty in this case may have been due to the port being used as a long-term access site for calcium gluconate infusions, leading to extensive calcifications. Operators at our institution typically use rated pressure (between 12 and 16 mmHg). If the catheter is not freed at the rated burst pressure with one or two dilations, especially at the site of venous insertion, we then increase the size of the balloon. All retained CVCs included in this report were 8 French catheters and were successfully removed in around 10 min from the start of the procedure. Table 2. Procedural and technical aspects of balloon-assisted retrieval casesCaseAge of CatheterReason for Catheter RemovalGuidewire Used for Removal^a^Balloon Used for Removal^b^Procedural ComplicationDay of DischargeCase 115 yearsNo longer functioning, recurrent bacteremia0.014-inch guidewire3.0 mm x 10 cm Sterling SLNoneSame DayCase 28 yearsCompletion of treatment0.014-inch guidewire2.5 mm x 10 cm Sterling SLNoneSame DayCase 312 yearsRecurrent bacteremia0.014-inch guidewire4 mm x 22 cm CoyoteNonePost-Op Day 3Case 411 yearsCompletion of treatment0.018-inch guidewire4.0 mm x 4 cm SterlingNoneSame DayCase 516 yearsNo longer functioning0.014-inch guidewire3.0 mm x 4 cm Coyote ESNoneSame DayCase 614 yearsNo longer functioning0.014-inch guidewire4.0 mm x 4 cm SterlingNoneSame DayCase 710 yearsNo longer functioning, recurrent bacteremia0.014-inch guidewire4.0 mm x 22 cm CoyoteNonePost-Op Day 1Case 814 yearsCompletion of treatment0.014-inch guidewire2 mm x 15 cm CoyoteNoneSame DayCase 99 yearsCompletion of treatment0.014-inch guidewire3 mm x 15 cm CoyoteNoneSame DayCase 1018 yearsRequested oral treatment0.014-inch guidewire2.5 mm x 15 cm CoyoteNoneSame DayCase 1129 yearsCompletion of treatment0.014-inch guidewire4.0 mm x 15 cm CoyoteNoneSame DayCase 1215 yearsRecurrent bacteremia0.014-inch guidewire6.0 mm x 22 cm SterlingNonePost-Op Day 7^a^The size of the guidewire was determined based on physician preference, and what was readily available in the procedural suite^b^The size of the balloon was determined based on physician preference, preoperative imaging, and trial and error if initial balloon failed to free the catheter tubing from extensive adhesions and calcifications
Results
The youngest patient in this series was 21 years old, while the oldest was 77, with an average age of 53.3 years. The shortest duration of indwelling catheter time in this series was 8 years, while the longest was 29 years, providing an average catheter indwelling time of 14.3 years. Nine patients were female (75.0%), and seven cases involved left-sided port-a-caths (58.3%).
All procedures were completed successfully, achieving a 100% success rate, minimal blood loss (< 10 mL, without need for pressure bandaging), and no procedural complications. Nine patients were discharged from the hospital on the same day as their procedure; however, three required additional treatment for ongoing bacteremia before discharge.
Recurrent bacteremia was reported as an indication for removal in four cases (33.3%), while a non-functional port-a-cath was indicated in four cases (33.3%). Completion of treatment without further need for indwelling CVC was cited as a reason for removal in five cases (41.7%). Additionally, one patient opted to receive oral medications after being treated via pediatric port-a-cath for 18 years.
Discussion
Prompt CVC removal via manual pulling is the optimal strategy to prevent complications when access is no longer needed. However, in cases of pericatheter fibrotic encapsulation, stenosis, or calcification, we recommend balloon-assisted retrieval as the primary method, especially for retained port-a-caths (Fig. 4), where current standard endovascular techniques have been known to fail [2, 5]. Additionally, it’s important to note that all retained CVCs were externally accessible in this series, allowing us to enter the catheter tubing directly without requiring additional percutaneous access or surgical incisions.Fig. 4. Digital subtraction angiography via a left-sided port-a-cath demonstrating a filling defect and contrast jet at the catheter tip typical of a fibrin sheath formation and the appearance of intravascular calcifications along the distal catheter tip
This study's limitations include its retrospective design, small sample size, absence of a control group, variability in balloon and guidewire selection, lack of long-term follow-up, and potential undetected complications (such as vessel injury and thrombosis). Furthermore, it is important to acknowledge that the findings are based on procedures performed by multiple physicians at a single institution, which may not reflect variations in practice, patient populations, or operator experience at other centers.
We opted for balloon-assisted retrieval due to the initial challenges faced during port-a-cath removal and our interest in its reported ease of use, effectiveness, and safety in hemodialysis catheter retrieval [3–5]. Throughout the procedures, we noted that the balloon's ability to disrupt adhesions and safely remove the retained catheter was remarkable, especially in cases where the catheter was firmly adhered or where conventional methods posed a greater risk of vessel injury [2, 5–7]. All cases were successfully completed using balloon-assisted retrieval without complications, consistent with existing data on hemodialysis catheter retrieval, indicating a higher success rate and a lower complication rate than other retrieval methods [5].
Although several well-documented foreign body retrieval options exist, including various endovascular devices and surgical interventions [5], we believe balloon-assisted retrieval provides a more controlled and less traumatic alternative. Furthermore, minimizing cost, risk, and procedure time aligns with our practice's goals of patient-centered care, as current standards for foreign body retrieval often require additional percutaneous access [6, 7], multiple catheters [5–7], additional procedural steps [6, 7], increased risk to patients [5], less delicate instruments [5–7], and longer time to completion. As the use of indwelling CVCs continues to rise, complications such as fibrotic encapsulation, calcification, and stenosis are likely to increase as well. Recognizing pericatheter adhesions and employing appropriate endovascular retrieval will be crucial for effectively managing our aging population.
Conclusion
Endoluminal balloon-assisted retrieval, an emerging technique for hemodialysis catheter removal, is a safe and effective method for retrieving long-term port-a-caths complicated by fibrotic encapsulation, calcification, and stenosis. Further prospective studies are needed to optimize and refine this technique; however, this minimally invasive approach helps mitigate risks associated with forceful traction and surgical removal while maintaining vascular integrity. Given its high success rate and low complication profile, balloon-assisted retrieval should be regarded as the primary method in cases where standard techniques fall short.