The effectiveness of acupuncture in the treatment of Tourette syndrome in Chinese children: a systematic review and meta-analysis
Qian-Qian Zhou, Zi-Chen Li, Zhuo-Ya Hu, Juan Tang, Peng Tang, Qi-Rui Wu, Zhong-Qi Deng, Wen-Bin Ma, Lei Lan

TL;DR
A review suggests acupuncture may help improve tics in Chinese children with Tourette syndrome compared to medication or other treatments.
Contribution
This study provides a systematic review and meta-analysis of acupuncture's effectiveness in treating pediatric Tourette syndrome in China.
Findings
Acupuncture may improve motor tics more than dopamine agonist medications in children with Tourette syndrome.
Acupuncture combined with other therapies may improve vocal tics more than other treatments alone.
The evidence supporting acupuncture's effectiveness is of low quality.
Abstract
As a prominent complementary and alternative therapy, acupuncture is widely used to treat Tourette syndrome in children. This review aims to evaluate its clinical efficacy and provide evidence-based support for acupuncture in pediatric Tourette syndrome. We systematically searched six databases: China National Knowledge Infrastructure, Wanfang Database, VIP Information Chinese Journal Service Platform, PubMed, Cochrane Central Register of Controlled Trials, and Embase, from their inception to 10 April 2025. Randomized controlled trials comparing acupuncture alone versus medication, or acupuncture plus other treatments versus other treatments alone, for children tic disorder were included. Thirty-two studies were included, with 2,201 participants. Acupuncture may be more effective in improving motor tics symptoms than dopamine agonist [WMD −3.04, 95% CI (−3.77, −2.31), RD 0.38 (0.29,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
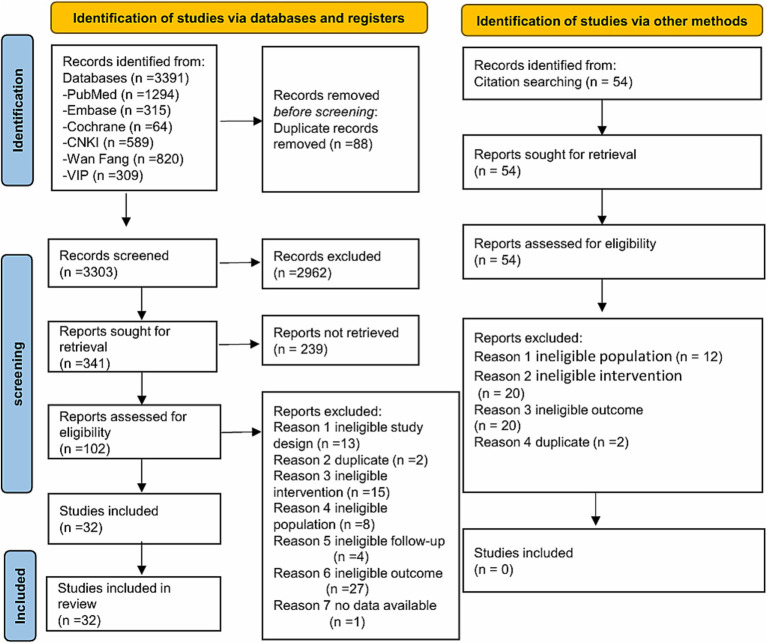 Figure 1
Figure 1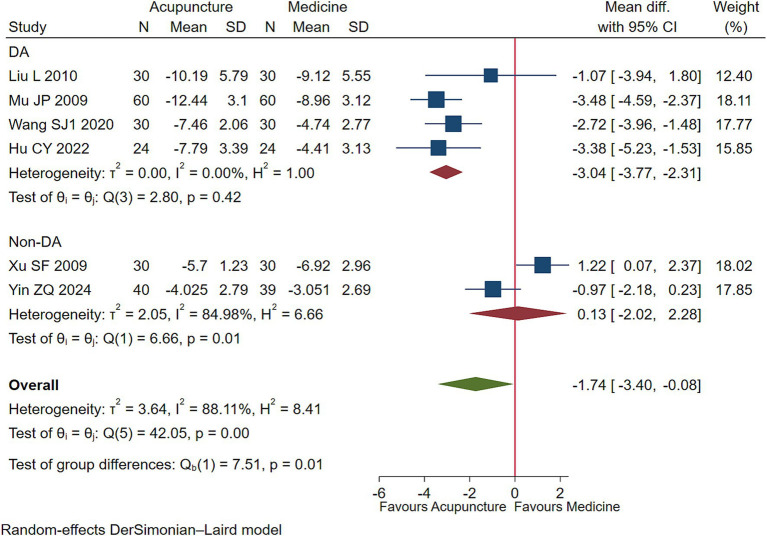 Figure 2
Figure 2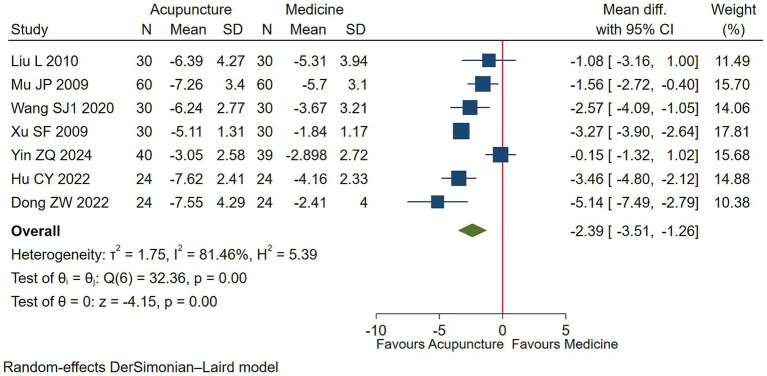 Figure 3
Figure 3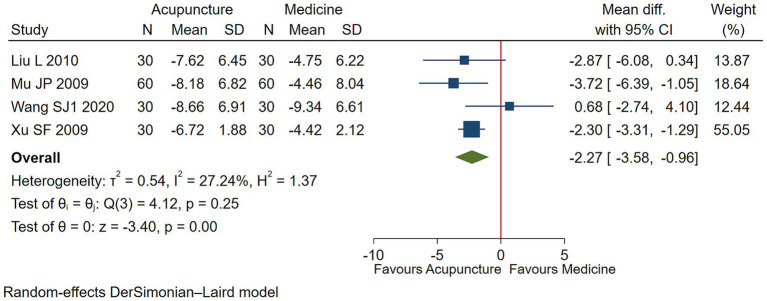 Figure 4
Figure 4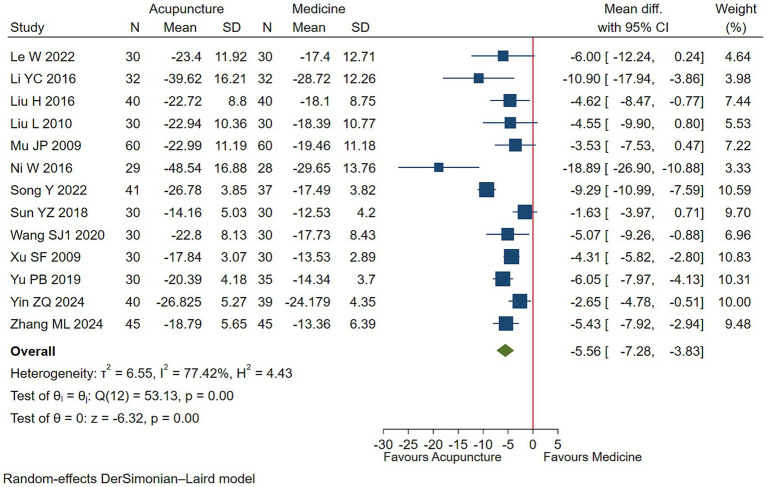 Figure 5
Figure 5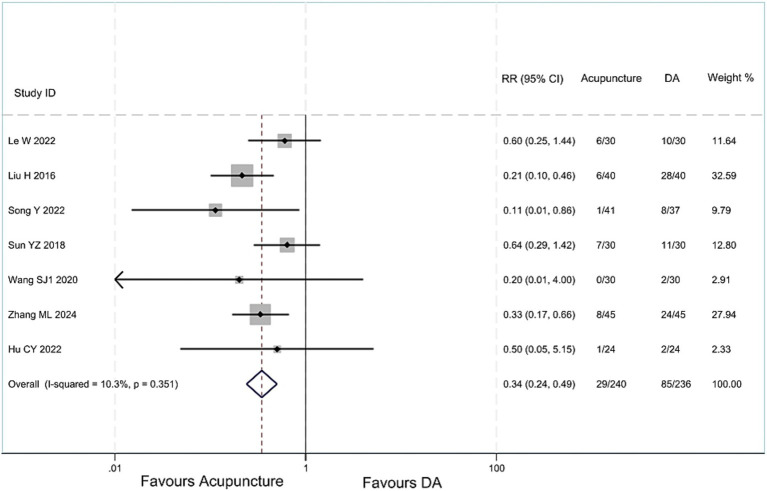 Figure 6
Figure 6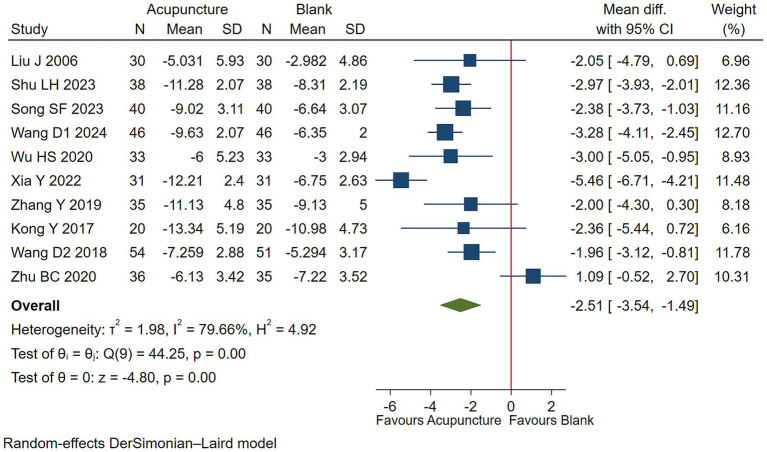 Figure 7
Figure 7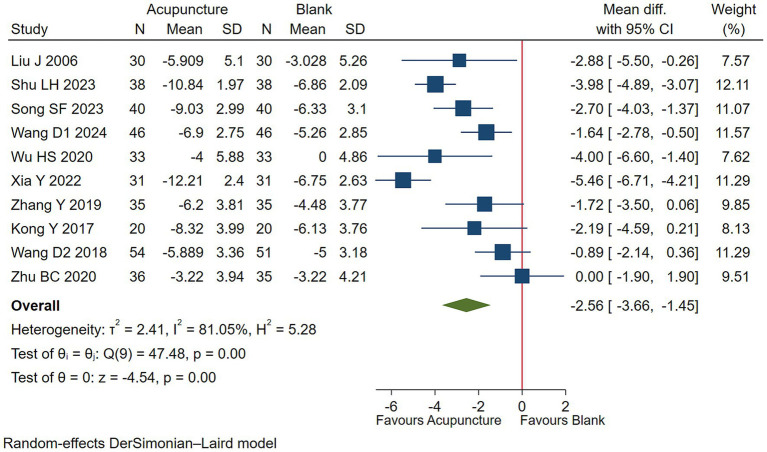 Figure 8
Figure 8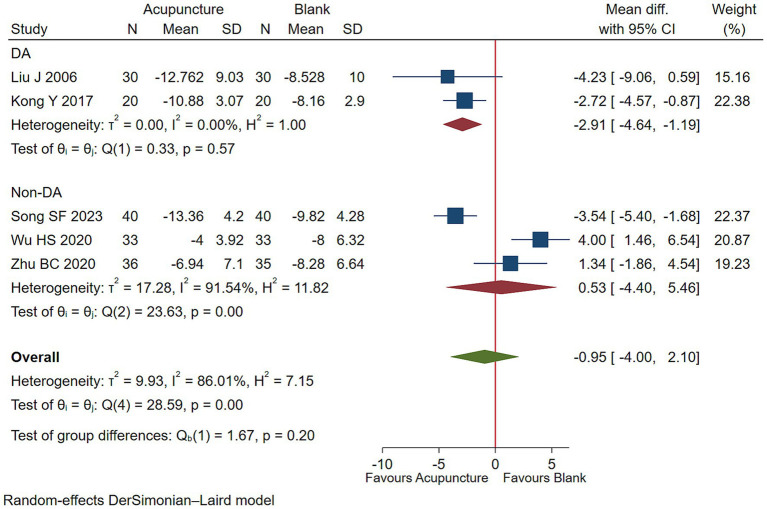 Figure 9
Figure 9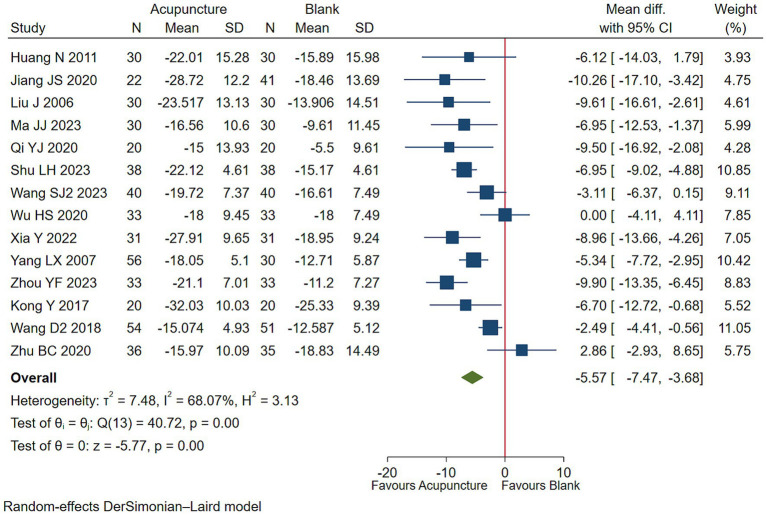 Figure 10
Figure 10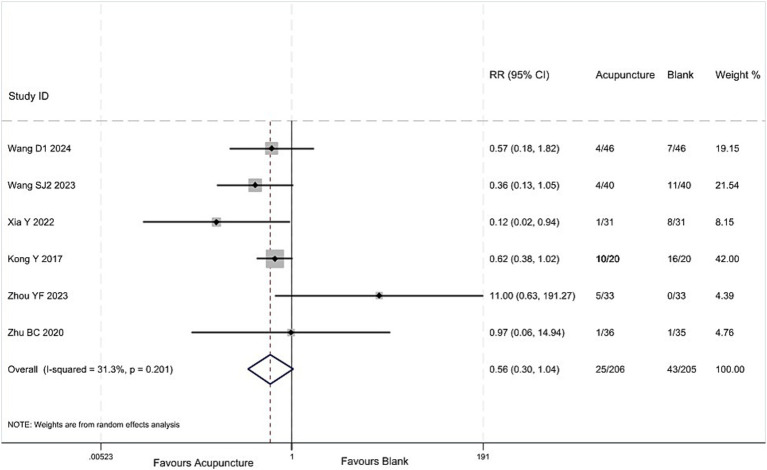 Figure 11
Figure 11| Study ID | Country | Funding | Treatment (No.) | Control (No.) | Sample size | Female (%) | Age (years) | Treatment duration | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Le W | China | Government | Acupuncture | Tiapride | 60 | 46.67% | 10.4 ± 3.03 | 4 M | ④⑤ |
| Li YC | China | NR | Acupuncture | Inosine tablets & Vitamin B6 | 64 | 32.81% | 8.25 ± 2.9 | 1 M | ④ |
| Liu H | China | NR | Acupuncture | Haloperidol | 80 | 22.5% | 9 ± 2.53 | 2 M | ④⑤ |
| Liu L | China | Government | Acupuncture | Haloperidol | 60 | 31.67% | 8.6 ± 3.2 | 2 M | ①②③④ |
| Mu JP | China | NR | Acupuncture & CBT | Haloperidol & CBT | 120 | 44.17% | 9.9 ± 3.11 | 6 W | ①②③④ |
| Ni W | China | NR | Acupuncture | Inosine tablets & Vitamin B6 | 57 | 40.35% | 8.66 ± 3.21 | 4 W | ④ |
| Song Y | China | NR | Acupuncture | Tiapride | 78 | 30.77% | 8.2 ± 0.77 | 3 M | ④⑤ |
| Sun YZ | China | Government | Acupuncture | Haloperidol | 60 | 21.67% | 14.9 ± 6.05 | 8 W | ④⑤ |
| Wang SJ1 | China | NR | Acupuncture | Tiapride | 60 | 18.33% | 8.9 ± 2.26 | 4 W | ①②③④⑤ |
| Xu SF | China | NO | Acupuncture | Risperidone | 60 | 11.67% | 9.5 ± 2.9 | 3 M | ①②③④ |
| Yin ZQ | China | NR | Acupuncture | Changma Xifeng Tablets | 79 | 30.38% | 7.71 ± 1.82 | 8 W | ①②④⑤ |
| Zhang ML | China | Government | Acupuncture | Tiapride | 90 | 27.78% | 7.5 ± 1.28 | 8 W | ④⑤ |
| Hu CY | China | NR | Acupuncture | Haloperidol | 48 | 47.92% | 8 ± 2.15 | 8 W | ①②⑤ |
| Dong ZW | China | Government | Acupuncture & CBT | Haloperidol & CBT | 48 | 47.92% | 8 ± 2.15 | 8 W | ①②③④ |
| Jiang JS | China | NR | Acupuncture & Chinese medicine | Chinese medicine | 63 | 9.52% | 7.7 ± 2.16 | 50D | ④ |
| Huang N | China | NR | Acupuncture & Chinese medicine | Chinese medicine | 60 | 25% | 8.2 ± 2.76 | 3 M | ④ |
| Liu J | China | NR | Acupuncture & | Haloperidol | 60 | 21.67% | 12.14 ± 3.23 | 1 M | ①②③④ |
| Ma JJ | China | NR | Acupuncture& | Haloperidol | 60 | 28.33% | 6.3 ± 1.29 | 4 W | ④ |
| Qi YJ | China | NR | Acupuncture & CBT | CBT | 40 | 17.5% | 9.5 ± 2.42 | 3 M | ④ |
| Shu LH | China | NR | Acupuncture & | Haloperidol & CBT | 76 | 28.95% | 8.8 ± 1.5 | 3 M | ①②④ |
| Song SF | China | Government | Acupuncture & | auricular points | 80 | 31.25 | 9 ± 1.29 | 3 M | ①②③ |
| Wang D1 | China | Government | Acupuncture & | Haloperidol | 92 | 16.3% | 6.8 ± 2.47 | 4 W | ①②⑤ |
| Wang SJ2 | China | Government | Acupuncture & Tiapride | Tiapride | 80 | 27.5% | 7.35 ± 1.88 | 4 W | ④⑤ |
| Wu HS | China | NR | Acupuncture & Chinese medicine | Chinese medicine | 66 | 30.30% | 9 ± 2.76 | 6 W | ①②③④ |
| Xia Y | China | NR | Acupuncture & Tiapride | Tiapride | 62 | 40.32% | 8 ± 2.25 | 2 M | ①②④⑤ |
| Yang LX | China | NR | Acupuncture & | Haloperidol & CBT | 86 | 13.95% | 11.7 ± 3.07 | 48D | ④ |
| Zhang Y | China | NR | Acupuncture & | Haloperidol | 70 | 28.57% | 9.1 ± 1.78 | 8 W | ①② |
| Zhou YF | China | Government | Acupuncture & | Clonidine | 66 | 21.21% | 8.5 ± 2.44 | 8 W | ④⑤ |
| Kong Y | China | NR | Acupuncture & | Haloperidol | 40 | 32.5% | 9 ± 2.83 | 8 W | ①②③④⑤ |
| Wang D2 | China | NR | Acupuncture & Tiapride | Tiapride | 105 | 19.08% | 8.9 ± 3.27 | 1 M | ①②④ |
| Zhu BC | China | Government | Acupuncture & Chinese medicine | Chinese medicine | 71 | 21.13% | 9.5 ± 3.2 | 12 W | ①②③④⑤ |
| Yu PB | China | NR | Acupuncture | Tiapride | 60 | 45% | 8 ± 1.77 | 1 M | ④ |
| Comparison | No. of trials | Follow-up days | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Treatment association (95% CI) | Overall quality of evidence | |
|---|---|---|---|---|---|---|---|---|---|---|
| Acupuncture vs. Medicine | Motor Tic Score, 0–25, lower is better | |||||||||
| 4 (288) | 28 to 60 | Seriousa | Not serious | Not serious | Seriousb | NA | WMD −3.04 (−3.77, −2.31) | Lowd | ||
| RD 0.38 (0.29, 0.46) | ||||||||||
| Acupuncture | Medicine | |||||||||
| Vocal Tic Score, 0–25, lower is better | ||||||||||
| 7 (475) | 28 to 90 | Seriousa | Serious | Not serious | Seriousb | NA | WMD −2.39 (−3.51, −1.26) | Low | ||
| RD 0.21 (0.10, 0.35) | ||||||||||
| Acupuncture | Medicine | |||||||||
| Impairment Score, 0–50, lower is better | ||||||||||
| 4 (300) | 28 to 90 | Seriousa | Not serious | Not serious | Seriousb | NA | WMD −2.27 (−3.58, −0.96) | Low | ||
| RD 0.05 (0.02, 0.09) | ||||||||||
| Acupuncture | Medicine | |||||||||
| Global Severity Score, 0–100, lower is better | ||||||||||
| 13 (993) | 28 to 120 | Seriousa | Serious | Not serious | Seriousc | NA | WMD −5.56 (−7.28, −3.83) | Low | ||
| RD 0.14 (0.09, 0.20) | ||||||||||
| Acupuncture | Medicine | |||||||||
| Adverse reactions | ||||||||||
| 7 (476) | 28 to 120 | Serious | Not serious | Not serious | Seriousb | NA | RR 0.34, 95%CI (0.24, 0.49) | Lowe | ||
| Comparison | No. of trials (No. of patients) | Follow-up days | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Treatment association (95% CI) | Overall quality of evidence | |
|---|---|---|---|---|---|---|---|---|---|---|
| Acupuncture vs. Blank | Motor Tic Score,0–25, lower is better | |||||||||
| 10 (722) | 28 to 90 | Seriousa | Serious | Not serious | Not serious | NA | WMD −2.51 (−3.54, −1.49) | Low | ||
| RD 0.31 (0.19, 0.41) | ||||||||||
| Acupuncture | Blank | |||||||||
| Vocal Tic Score, 0–25, lower is better | ||||||||||
| 10 (722) | 28 to 90 | Seriousa | Serious | Not serious | Not serious | NA | WMD −2.56 (−3.66, −1.45) | Low | ||
| RD 0.28 (0.15, 0.40) | ||||||||||
| Acupuncture | Blank | |||||||||
| Impairment Score, 0–50, lower is better | ||||||||||
| 2 (100) | 30 to 90 | Seriousa | Not serious | Not serious | Seriousb | NA | WMD −2.91 (−4.64, −1.19) | Lowd | ||
| RD 0.13 (0.05, 0.23) | ||||||||||
| Acupuncture | Blank | |||||||||
| Global Severity Score, 0–100, lower is better | ||||||||||
| 14 (935) | 28 to 90 | Seriousa | Not serious | Not serious | Seriousc | NA | WMD −5.57 (−7.47, −3.68) | Low | ||
| RD 0.11 (0.06, 0.17) | ||||||||||
| Acupuncture | Blank | |||||||||
| Adverse reactions | ||||||||||
| 6 (411) | 28 to84 | Seriousa | Not serious | Not serious | Seriousb | NA | RR 0.56, 95%CI (0.30,1.04) | Low | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObsessive-Compulsive Spectrum Disorders
Introduction
1
Tourette’s syndrome (TS) is a prevalent chronic neuropsychiatric disorder representing a distinct chronic subtype of tic disorders: onset occurs before age 18, with a duration exceeding 1 year; it involves both motor and vocal tics, which may occur asynchronously. This distinguishes it from chronic tic disorders presenting solely with one tic type and transient tic disorders lasting less than 1 year. Patients typically present with semivoluntary muscle twitching in the head, face, shoulders, neck, and limbs, alongside abnormal vocalizations. These symptoms are frequently accompanied by psychological comorbidities such as attention deficit hyperactivity disorder and obsessive-compulsive disorder (1). The causes and mechanisms of the disease remain unclear, and treatment primarily involves symptomatic drug therapy (2). Long-term medication use often leads to adverse neurological reactions, such as blurred vision, drowsiness, fatigue, nausea, and vomiting, making it difficult for children to comply with long-term medication regimens, resulting in suboptimal treatment outcomes (3). Acupuncture is a non-pharmacological therapy for neurological disorders. Research indicates that acupuncture has demonstrated substantial efficacy in treating such conditions, including central nervous system disorders such as stroke and migraine, and peripheral nervous system disorders such as Bell’s palsy and trigeminal neuralgia. With its minimal adverse reactions, acupuncture is gaining increasing acceptance among practitioners and patients alike (4, 5). This study aims to evaluate the clinical efficacy of acupuncture in treating children with TS and provide evidence-based medical for acupuncture treatment of childhood Tourette syndrome.
Methods
2
Literature search
2.1
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (6) to report our systematic review and registered it in PROSPERO (registration number: CRD42023444312). The search strategy is as follows: (1) Database Search: China National Knowledge Infrastructure, Wanfang Data Online Knowledge Service Platform, VIP Information Chinese Journal Service Platform, PubMed, Cochrane Central Register of Controlled Trials, and Embase Database. (2) Manual Search: (1) China Clinical Trials Registry (search terms: Tourette syndrome AND acupuncture); (2) Included literature from published systematic reviews and their reference lists. The search was conducted up to 10 April 2025, with no language restrictions. (Database search terms and search results are listed in Supplementary Table 1).
Literature screen and data extraction
2.2
After removing duplicate documents using Endnote 21 software, four researchers (QQZ, ZCL, ZYH, JT) independently read the titles, abstracts, and full texts of all documents to determine the final documents to be included. In case of disagreement, the issue was resolved through discussion or by the third party (PT, LL). Data extraction was conducted independently by four researchers (QQZ, ZCL, ZYH, JT) in a blinded fashion. The extracted data included: literature characteristics (title, authors, publication year, age, disease duration, sample size, intervention and control measures), methodological information (randomization method, allocation concealment, use of blinding, loss to follow-up), and outcome measures (tics, vocal tics, functional impairment, adverse reactions). After extraction, we applied the following inclusion and exclusion criteria.
Inclusion criteria: (1) patients diagnosed with TS according to the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (7), with a disease duration of over 1 year and no tic-free periods exceeding 2 months, aged <18 years,(2) acupuncture vs. western medicine, acupuncture vs. blank control, with a follow-up ≥4 weeks, (3) randomized controlled trial (RCT), (4) primary outcomes involved tic symptoms, coprolalia symptoms, and functional impairment, and secondary outcomes were adverse reactions.
Exclusion criteria: (1) Semi-randomized controlled trials; (2) Tics attributable to other neurological disorders.
Risk of bias assessment
2.3
The risk of bias in the included RCTs was assessed independently by two reviewers (QQZ, ZCL) using the Cochrane Risk of Bias 1.0 tool (8, 9). The following domains were rated: (1) random sequence generation; (2) allocation concealment; (3) blinding of participants and personnel; (4) blinding of outcome assessment; (5) incomplete outcome data; (6) selective reporting; and (7) other sources of bias.
Data analysis
2.4
Continuous variables were analyzed using the weighted mean difference (WMD) and corresponding confidence interval (95% CI); binary variables were analyzed using the relative risk (RR) and 95% CI. All meta-analyses were performed using a random-effects model in Stata 17 software. Heterogeneity was assessed using the I^2^ value and Q test, with an I^2^ value ≥ 50% indicating high heterogeneity. Subgroup analysis was conducted to identify sources of heterogeneity. To better interpret the clinical significance of effect sizes, we defined an effect size of ≥30% reduction from baseline as the minimal clinically important difference (MCID), and calculated the risk difference (RD) between groups to quantify between-group differences.
Certainty of evidence
2.5
We used the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) method to assess the certainty of evidence for each outcome (10). Evidence from RCTs started at high quality but can be downgraded to high, moderate, low, or very low quality based on factors such as risk of bias, consistency, directness, precision, and publication bias.
Results
3
Literature screening
3.1
Database search yielded 3,391 records. Manual search yielded 54 records from 11 published systematic reviews (11–21). Thirty-two studies were ultimately included (Figure 1).
Literature screening process and results of acupuncture for children with TS.
Characteristics of included studies
3.2
Thirty-two studies (22–52) were included, involving 2,201 patients, with 28.17% being female. All included studies were conducted in China, and 10 studies (22, 25, 29, 34, 36, 42–44, 48, 51) received funding support. Among the 25 studies reporting participants’ specific ages, the average age of participants was 8.84 years, with the shortest intervention duration being 28 days and the longest being 120 days. This included 15 acupuncture vs. medication control studies (22–31, 33–36, 52), 11 acupuncture combined with medication vs. medication alone control studies (38, 39, 41, 43, 44, 46–50, 52, 53), 4 studies comparing acupuncture combined with Chinese herbal medicine vs. Chinese herbal medicine alone (32, 37, 45, 51), 1 study comparing acupuncture combined with ear acupuncture vs. ear acupuncture alone (42), and 1 study comparing acupuncture combined with cognitive behavioral therapy vs. cognitive behavioral therapy alone (40). Fourteen studies (22, 24, 28–30, 33–35, 43, 44, 46, 48, 49, 51) reported adverse reactions. The detailed information of the included studies can be seen in Table 1.
Risk of bias
3.3
All of the 32 included studies showed that 26 (81%) had adequate randomization sequence generation, 3 (9%) had adequate allocation concealment (22, 35, 36), and 3 (9%) had blinding of data collectors, data processors, and data analysts (22, 35, 36). Six studies reported patient attrition (27, 32, 37, 48, 51, 53), but the attrition rates did not exceed 20% in any case (Supplementary Table 3).
Acupuncture vs. medicine
3.4
Motor tic symptoms
3.4.1
Low-quality evidence (4 studies, 288 participants) suggested that acupuncture may lessen motor tics symptoms in children with TS than DA [WMD −3.04, 95% CI (−3.77, −2.31), RD 0.38 (0.29, 0.46) (Figure 2; Table 2)] (25, 26, 30, 35).
Acupuncture vs. medicine evaluation of efficacy of motor tics.
Vocal tic symptoms
3.4.2
Low-quality evidence (7 studies, 475 participants) suggested that acupuncture may slightly improve vocal tics symptoms in children with TS compared to conventional medication [WMD −2.39, 95% CI (−3.51, −1.26), RD 0.21 (0.10, 0.35) (Figure 3, Table 2)] (25, 26, 30, 31, 33, 35, 36).
Acupuncture vs. medicine evaluation of efficacy of vocal tics.
Functional impairment
3.4.3
Low-quality evidence (4 studies, 300 participants) suggested that acupuncture may has a negligible effect on functional impairment in children with TS [WMD −2.27, 95% CI (−3.58, −0.96), RD 0.05 (0.02, 0.09) (Figure 4; Table 2)] (25, 26, 30, 31).
Acupuncture vs. medicine evaluation of efficacy of functional improvement.
Overall symptom severity
3.4.4
Low-quality evidence (13 studies, 995 participants) suggested that acupuncture may slightly control overall symptom severity in children with TS [WMD −5.56, 95% CI (−7.28, −3.83), RD 0.14 (0.09, 0.20) (Figure 5; Table 2)] (22–31, 33, 34, 52).
Acupuncture vs. medicine evaluation of efficacy of overall symptom efficacy evaluation.
Adverse reactions
3.4.5
Low-quality evidence (7 studies, 476 participants) suggested that acupuncture treatment for children with TS has less adverse reactions than DA, [RR 0.34, 95%CI (0.24, 0.49) (Figure 6; Table 2)] (22, 24, 28–30, 34, 35). One article (33) compared the acupuncture group with the drug group, and found no difference in the incidence of adverse reactions between the two groups.
Acupuncture vs. DA group analysis of the incidence of adverse reactions.
Acupuncture vs. blank control on basis of usual care
3.5
Motor tic symptoms
3.5.1
Low-quality evidence (10 studies, 722 participants) suggested that acupuncture may lessen more motor tics symptoms in children with TS than blank treatment on basis of usual care [WMD −2.51, 95% CI (−3.54, −1.49), RD 0.31 (0.19, 0.41) (Figure 7; Table 3)] (38, 41–43, 45–47, 49–51).
Acupuncture vs. blank control on basis of usual care evaluation of efficacy of motor tics.
Vocal tic symptoms
3.5.2
Low-quality evidence (10 studies, 722 participants) suggested that acupuncture may improve vocal tics symptoms in children with TS compared to blank treatment on basis of usual care [WMD −2.56, 95% CI (−3.66, −1.45), RD 0.28 (0.15, 0.40) (Figure 8; Table 3)] (38, 41–43, 45–47, 49–51).
Acupuncture vs. blank control on basis of usual care evaluation of efficacy of vocal tics.
Functional impairment
3.5.3
Low-quality evidence (2 studies, 100 participants) suggested that acupuncture with DA may lessen functioning impairment than DA [WMD −2.91, 95% CI (−4.64, −1.19), RD 0.13 (0.05, 0.23) (Figure 9; Table 3)] (38, 42, 45, 49, 51).
Acupuncture vs. blank control on basis of usual care evaluation of efficacy of functional improvement.
Overall symptom severity
3.5.4
Low-quality evidence (14 studies, 935 participants) suggested that acupuncture may be superior in improving overall symptoms severity in children with TS than blank treatment [WMD −5.57, 95% CI (−7.47, −3.68), RD 0.11 (0.06, 0.17) (Figure 10; Table 3)] (32, 37–41, 44–46, 48–51, 53).
Acupuncture vs. blank control on basis of usual care evaluation of efficacy of overall symptom efficacy evaluation.
Adverse reactions
3.5.5
Low-quality evidence (6 studies, 411 participants) suggested that the incidence of adverse reactions in children with TS treated with acupuncture combined with other therapies is not significantly different from that in children treated with other therapies alone, [RR 0.56, 95%CI (0.30, 1.04), (Figure 11; Table 3)] (43, 44, 46, 48, 49, 51).
Acupuncture vs. blank control on basis of usual care analysis of the incidence of adverse reactions.
Discussion
4
Overall findings
4.1
Compared with pharmacotherapy, acupuncture may alleviate more motor tics symptoms with less adverse effects, but it may bring about slight improvement in vocal tics, functional impairments, and overall symptom severity in Chinese children with TS. Compared with blank treatment, acupuncture may alleviate more motor tics, vocal tics symptoms, functional impairments, and overall symptom severity in Chinese children with TS.
Relation of other studies
4.2
We identified eleven systematic reviews on acupuncture treatment for childhood tic disorders (11–21). After screening their included studies, we excluded those that enrolled patients with chronic or transient tic disorders, or that used ineligible comparators or outcomes (Supplementary Table 2).
The latest systematic review (21) included 26 studies, with a search cut-off date of October 2023. The results indicated that acupuncture is more effective than most existing treatments in alleviating motor and vocal tics in children with TS, while also reducing the incidence of adverse reactions. However, some outcome measures in the included studies only reported treatment efficacy rates, failing to clearly assess improvements in tic symptom-related scores. Additionally, the study did not include outcomes related to functional impairments in children with TS, focusing solely on motor and vocal tics. Finally, the study did not assess the certainty of the evidence, lacking a certain degree of professionalism.
This study included 18 RCTs not included in the latest review and excluded 12 studies included in the review, with specific reasons as follows: (1) Six studies had questionable inclusion criteria for children with TS, including patients with chronic tic disorder and transient tic disorder (54–59), (2) Two studies had acupuncture intervention durations of less than 28 days (60, 61), (3) Four studies did not report reasonable tic symptom scores (62–65). Our findings lead to a more cautious conclusion than the latest review and emphasize that the role of acupuncture in the treatment of TS in children requires further clinical research to confirm. (Supplementary Table 2).
Strengths and limitations
4.3
The strengths of this study include a comprehensive search for eligible RCTs and a focus on patient-reported outcome measures, with analysis conducted across three domains: motor tics, vocal tics, and functional impairment. We used the GRADE method to assess the certainty of the evidence and referenced the latest research results from the BMJ (66) and Cochrane Collaboration (10) for methodological exploration: first, we calculated the scores where the reduction rate in each YGTSS subscale reached at least 30%, defining this as the MCID. We then calculated the probability of achieving this value in the acupuncture group and the control group, respectively, and used the RD to display the between-group differences, thereby making the findings more accessible and clinically interpretable.
This study has limitations. Only three studies (22, 35, 36) adequately described random-sequence generation, allocation concealment, participant blinding, and implementation details. Additionally, due to the special nature of acupuncture procedures, it was not possible to blind patients or operators, resulting in a high risk of bias. Our review was based on the Chinese population, which limits its generalizability. Evidence from other populations is therefore needed for further analysis.
Implications
4.4
Chinese children with TS who receive acupuncture may experience greater relief of motor tics and fewer adverse effects compared with those on pharmacotherapy. Relative to no-treatment controls, these children also demonstrate larger reductions in vocal tics, functional impairment, and overall symptom severity. Low-certainty evidence underpins these conclusions on basis of Chinese population. Future trials should adopt rigorous methodological safeguards to minimize bias, and additional well-designed RCTs are required to clarify the efficacy of acupuncture for pediatric tic disorders.
Conclusion
5
Compared to pharmacotherapy, acupuncture may relieve more motor tics symptoms with less adverse effects, but it may slightly improve vocal tics, functional impairments, and overall symptom severity in Chinese children with TS. Compared to blank treatment, acupuncture may alleviate more motor tics, vocal tics symptoms, functional impairments, and overall symptom severity in Chinese children with TS. All results are supported by low-quality evidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hirschtritt ME Lee PC Pauls DL Dion Y Grados MA Illmann C . Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry. (2015) 72:325–33. doi: 10.1001/jamapsychiatry.2014.2650, PMID: 25671412 PMC 4446055 · doi ↗ · pubmed ↗
- 2Roth J . The colorful spectrum of Tourette syndrome and its medical, surgical and behavioral therapies. Parkinsonism Relat Disord. (2018) 46:S 75–9. doi: 10.1016/j.parkreldis.2017.08.004, PMID: 28807495 · doi ↗ · pubmed ↗
- 3Lin LP Gao X Li YP Teng SY WSM LXF. Interpretation of the European clinical practice guidelines for the pharmacological treatment of Tourette syndrome, version 2.0. J Psychiatry. (2023) 36:87–91. Available online at: https://kns.cnki.net/kcms 2/article/abstract?v=i 9Xs I Id 0T 11t C Fxyje U 4R Ljyzip 6Vg T Qe-QL Igx PM Ei Fc F 8zpz 1Bk 3N Rctst-Een ZS 1agn JP-fv 8j P 94b Rg FLI_6qb E Dkf-6Jv 1he B Ws VU 5A Zh Hv 0yc ORBI 9Zo Jetpa Fe 7t Ljcta 5BS Nhc XY 54ms 3Vy 19sn CKQNNR Dd Wm NUE Sg N Npoz Hrm DP Eg==&uniplatform=NZKPT&language=CHS
- 4Zhang MJ LHY. Clinical and mechanisms of acupuncture and moxibustion in the treatment of childhood Tourette′s disease. Asia-Pacific Traditional Med. (2020) 16:208–10. doi: 10.11954/ytctyy.202001065 · doi ↗
- 5Yao J Bao QN Wu KX Zhong WQ Zhang YX Chen ZW . The overview and future trend of high-quality clinical randomized controlled trial of acupuncture for neurological disorders. Modern. Traditional Chinese Med. Materia Medica. (2024) 27:973–81. doi: 10.11842/wst.20240409003 · doi ↗
- 6Moher D Liberati A Tetzlaff J Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. (2009) 62:1006–12. doi: 10.1016/j.jclinepi.2009.06.005, PMID: 19631508 · doi ↗ · pubmed ↗
- 7Jones KS Saylam E Ramphul K. Tourette syndrome and other tic disorders. Stat Pearls. Treasure Island (FL): Stat Pearls Publishing Copyright © 2025, Stat Pearls Publishing LLC (2025).29763133 · pubmed ↗
- 8Higgins JP Altman DG Gøtzsche PC Jüni P Moher D Oxman AD . The Cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d 5928. doi: 10.1136/bmj.d 5928, PMID: 22008217 PMC 3196245 · doi ↗ · pubmed ↗