Gene variants of glucocorticoid activation pathways and the outcomes of patients with Takayasu arteritis – a retrospective cohort study
Faustino Peron Filho, Andressa de Souza Moreira, Eduarda Bonelli Zarur, Gerson Dierley Keppeke, Alexandre Wagner Silva de Souza

TL;DR
This study found that a specific gene variant in the NR3C1 gene is linked to increased risks of glucocorticoid-related side effects and ischemic events in patients with Takayasu arteritis.
Contribution
The study identifies the NR3C1 gene variant 9β as a novel risk factor for glucocorticoid-related adverse events and ischemic events in Takayasu arteritis patients.
Findings
The NR3C1 9β polymorphism is associated with higher glucocorticoid-related adverse events and weight gain.
Worsening glucose tolerance is a strong independent risk factor for acute ischemic events.
The NR3C1 9β variant is an independent risk factor for ischemic arterial events.
Abstract
This study aims to evaluate the influence of polymorphisms of the HSD11B1, FKBP5 and NR3C1 genes on the outcomes of patients with Takayasu arteritis (TAK). A retrospective cohort study including 81 TAK patients was carried out. Polymorphisms of the genes HSD11B1 (rs11119328), FKBP5 (rs1360780) and NR3C1 (N363S, Bcll, TthIIII1, ER22/23EK and 9ß) were genotyped by the Sanger technique. Associations between the gene variants and the haplotypes (HT) of the NR3C1 gene with variables related to the outcome of TAK and glucocorticoid (GC)-related adverse events (AEs) were analyzed. The polymorphism 9β of the NR3C1 gene, which leads to decreased GC sensitivity, was associated with a higher frequency of GC-related AEs [3.0 (2.0-3.8) vs. 2.0 (1.0-3.0); p = 0.002] and weight gain (37.5% vs. 8.9%; p = 0.012). Worsening glucose tolerance (i.e., a key GC-related AE) was an independent risk factor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
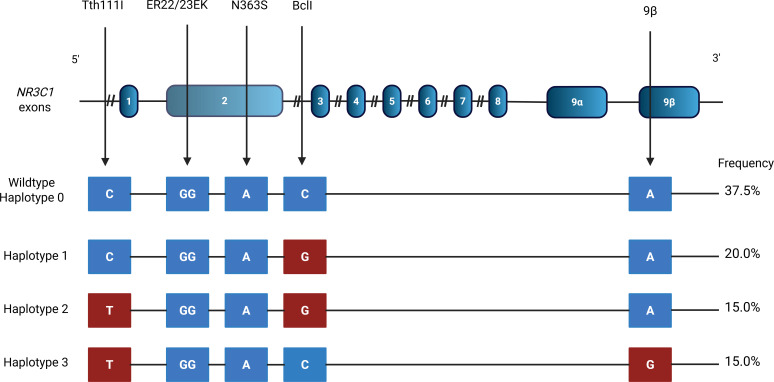 Figure 1
Figure 1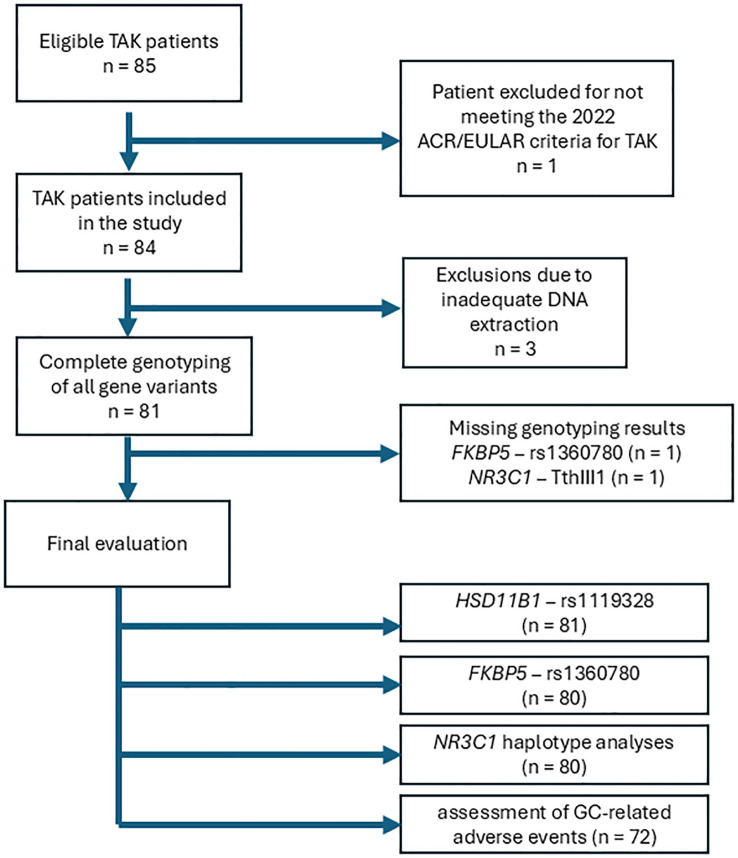 Figure 2
Figure 2| Variables | Results (n = 81) |
|---|---|
| Age at diagnosis, years | 29.6 ± 11.4 |
| Race | |
| Whites, n (%) | 46 (56.8) |
| Mestizos, n (%) | 22 (27.2) |
| Blacks, n (%) | 10 (12.3) |
| Asians, n (%) | 3 (3.7) |
| Median disease duration, months | 85.0 (54.0-103.0) |
| Acute phase reactants at diagnosis | |
| ESR, mm/hour | 29.5 (14.0-50.3) |
| CRP, mg/L | 4.9 (1.0-10.7) |
| Angiographic types | |
| Type V, n (%) | 58 (71.6) |
| Type I, n (%) | 11 (13.6) |
| Type IV, n (%) | 6 (7.4) |
| Type IIb, n (%) | 4 (4.9) |
| Type IIa, n (%) | 1 (1.2) |
| Type III, n (%) | 1 (1.2) |
| Ischemic events, n (%) | 23 (28.4) |
| Number of ischemic events | 32 |
| MI, n (%) | 7 (30.4) |
| Angina pectoris, n (%) | 9 (39.1) |
| TIA, n (%) | 4 (17.4) |
| Stroke, n (%) | 6 (26.1) |
| Abdominal angina, n (%) | 5 (21.7) |
| Subclavian steal syndrome, n (%) | 13 (16.0) |
| Renovascular hypertension, n (%) | 19 (23.5) |
| Involvement of pulmonary arteries, n (%) | 14 (17.3) |
| Progression of arterial lesions, n (%) | 42 (51.9) |
| Variables | Carriers (n = 27) | Non carriers (n = 54) |
| Carriers (n = 44) | Non carriers (n =35) |
|
|---|---|---|---|---|---|---|
|
|
| |||||
|
|
| |||||
| Subclavian steal syndrome, n (%) | 6 (22.2) | 7 (13.0) | 0.341 | 7 (15.9) | 5 (14.3) | 0.842 |
| Renovascular hypertension, n (%) | 7 (25.9) | 12 (22.2) | 0.711 | 12 (27.3) | 7 (20.0) | 0.452 |
| Pulmonary artery involvement, n (%) | 5 (18.5) | 9 (16.7) | 1.000 | 9 (20.5) | 5 (14.3) | 0.476 |
| Angiographic type V, n (%) | 20 (74.1) | 38 (70.4) | 0.727 | 32 (72.7) | 25 (71.4) | 0.898 |
| Ischemic events, n (%) | 6 (22.2) | 17 (31.5) | 0.384 | 11 (25.0) | 11 (31.4) | 0.527 |
| Sustained remission, n (%) | 16 (59.3) | 33 (61.1) | 0.872 | 25 (56.8) | 22 (62.9) | 0.587 |
| Progression of arterial lesions, n (%) | 15 (55.6) | 27 (50.0) | 0.637 | 21 (47.7) | 21 (60.0) | 0.278 |
| Need for bDMARD therapy, n (%) | 18 (66.7) | 27 (50.0) | 0.155 | 24 (54.5) | 21 (60.0) | 0.627 |
| TADS | 5.0 (2.5-8.0) | 4.5 (3.0-6.7) | 0.965 | 5.0 (2.3-6.0) | 4.5 (3.0-8.8) | 0.264 |
| VDI | 3.0 (1.2-4.0) | 2.0 (2.0-3.0) | 0.640 | 2.0 (2.0-3.0) | 3.0 (2.0-5.0) | 0.066 |
| Vascular interventions, n (%) | 9 (33.3) | 18 (33.3) | 1.000 | 15 (34.1) | 12 (34.3) | 0.986 |
|
|
| |||||
| Presence of GC-related AEs, n (%) | 16 (66.7) | 32 (66.7) | 1.000 | 28 (66.7) | 20 (69.0) | 0.839 |
| Number of GC-related AEs, n (%) | 1.5 (1.0-3.0) | 2.0 (0.3-3.0) | 0.912 | 2.0 (1.0-3.0) | 3.0 (1.0-3.0) | 0.378 |
| Severe infections, n (%) | 3 (12.5) | 3 (6.3) | 0.393 | 3 (7.1) | 3 (10.3) | 0.683 |
| GTI | 40.0 (19.0-91.5) | 46.0 (19.0-71.0) | 0.598 | 38.5 (19.0-74.3) | 50.0 (19.0-92.0) | 0.700 |
| CCI | 1.0 (1.0-2.5) | 2.0 (1.0-3.0) | 0.380 | 1.0 (1.0-3.0) | 2.0 (1.0-3.0) | 0.689 |
| Cumulative prednisone dose, mg | 14,553.75 ± 1,413.66 | 13,126.49 ± 995.78 | 0.414 | 13,334.54 ± 1,072.72 | 14,124.53 ± 1,291.86 | 0.640 |
| Variables | Carriers (n = 28) | Non carriers (n = 44) |
| Carriers (n = 16) | Non carriers (n = 56) |
|
|---|---|---|---|---|---|---|
|
|
| |||||
|
|
| |||||
| Subclavian steal syndrome, n (%) | 6 (20.0) | 7 (13.72) | 0.536 | 5 (31.3) | 8 (12.3) | 0.120 |
| Renovascular hypertension, n (%) | 10 (33.3) | 9 (17.6) | 0.108 | 3 (18.8) | 16 (24.6) | 0.751 |
| Pulmonary artery involvement, n (%) | 3 (10.0) | 11 (21.6) | 0.184 | 4 (25.0) | 10 (15.4) | 0.460 |
| Angiographic type V, n (%) | 23 (76.7) | 35 (68.6) | 0.438 | 10 (62.5) | 48 (73.8) | 0.371 |
| Ischemic events, n (%) | 9 (30.0) | 14 (27.5) | 0.806 | 8 (50.0) | 15 (23.1) | 0.060 |
| Sustained remission, n (%) | 17 (56.7) | 32 (62.7) | 0.589 | 7 (43.8) | 42(64.6) | 0.126 |
| Progression of arterial lesions, n (%) | 15 (50.0) | 27 (52.9) | 0.798 | 8 (50.0) | 34 (52.3) | 0.869 |
| Need for bDMARD therapy, n (%) | 16 (53.3) | 29 (56.9) | 0.758 | 9 (56.3) | 36 (55.4) | 0.950 |
| TADS | 4.0 (3.0-6.7) | 5.0 (3.5-7.5) | 0.263 | 6.0 (4.3-9.0) | 4.0 (3.0-6.0) | 0.117 |
| VDI | 2.0 (1.0-3.2) | 3.0 (2.0-4.0) | 0.416 | 3.0 (2.0-4.5) | 2.0 (2.0-4.0) | 0.381 |
| Vascular interventions, n (%) | 10 (33.3) | 17 (33.3) | 1.000 | 5 (31.3) | 22 (33.8) | 0.844 |
|
|
| |||||
| Presence of GC-related AEs, n (%) | 18 (64.3) | 30 (68.2) | 0.732 | 13 (81.3) | 35 (62.5) | 0.161 |
| Number of GC-related AEs, n (%) | 2.0 (1.0-3.0) | 1.0 (1.0-3.0) | 0.272 | 3.0 (2.0-3.8) | 2.0 (1.0-3.0) | 0.002* |
| Severe infections, n (%) | 3 (10.7) | 3 (6.8) | 0.672 | 2 (12.5) | 4 (7.1) | 0.609 |
| GTI | 29.5 | 49.0 | 0.420 | 61.0 | 30.0 | 0.289 |
| CCI | 1.5 (1.0-3.8) | 1.0 (1.0-3.0) | 0.773 | 2.0 | 1.0 | 0.386 |
| Cumulative prednisone dose, mg | 13,887.03 ± 1,304.93 | 13,421.02 ± 1,040.81 | 0.781 | 14,594.46 ± 1,273.43 | 12,933.08 ± 1,045.68 | 0.902 |
| Variables | HT1 (n=16) | HT2 (n=12) | HT3 (n=12) |
|
|---|---|---|---|---|
| TAK features and outcomes | ||||
| Subclavian steal syndrome, n (%) | 3 (18.8) | 2 (16.7) | 3 (25.0) | 0.867 |
| Renovascular hypertension, n (%) | 6 (37.5) | 4 (33.3) | 3 (25.0) | 0.781 |
| Pulmonary artery involvement, n (%) | 2 (12.5) | 1 (8.3) | 4 (33.3) | 0.217 |
| Angiographic type V, n (%) | 14 (87.5) | 9 (75.0) | 9 (75.0) | 0.626 |
| Ischemic events, n (%) | 5 (31.3) | 2 (16.7) | 4 (33.3) | 0.599 |
| Sustained remission, n (%) | 8 (50.0) | 9 (75.0) | 6 (50.0) | 0.342 |
| Progression of arterial lesions, n (%) | 8 (50.0) | 6 (50.0) | 6 (50.0) | 1.000 |
| Need for bDMARD therapy, n (%) | 8 (50.0) | 6 (50.0) | 6 (50.0) | 1.000 |
| TADS | 3.5 (2.8-6.0) | 4.0 (3.0-6.8) | 5.0 (2.5-9.0) | 0.586 |
| GC-related variables | ||||
| GC-related adverse events, n (%) | 9 (60.0) | 7 (63.6) | 9 (75.0) | 0.705 |
| Number of adverse events | 1.5 (1.0-2.8) | 1.5 (1.0-2.3) | 3.0 (2.0-3.0) | 0.032* |
| Severe infections, n (%) | 3 (20.0) | 0 (0.0) | 2 (16.7) | 0.300 |
| GTI Score | 82.5 (16.8-99.5) | 24.0 (10.0-48.0) | 50.0 (20.5-89.0) | 0.119 |
| CCI Score | 1.0 (1.0-2.0) | 2.0 (1.0-4.0) | 1.5 (1.0-2.8) | 0.711 |
| Cumulative dose of prednisone, mg | 13,527.24 ± 1,972.50 | 15,556.91 ± 2,314.90 | 15,325.06 ± 2,201.36 | 0.754 |
| Variables | OR | 95% CI |
|
|---|---|---|---|
|
| |||
| rs1119328 | 0.685 | 0.204-2.307 | 0.542 |
| Sustained remission | 0.656 | 0.180-2.398 | 0.524 |
| bDMARDs | 2.085 | 0.652-6.671 | 0.215 |
| Vascular interventions | 1.102 | 0.292-4.163 | 0.886 |
| Worsening glucose tolerance | 8.928 | 2.132-37.391 | 0.003* |
| GC-induced hyperlipidemia | 0.595 | 0.174-2.032 | 0.407 |
| Worsening hypertension | 0.543 | 0.165-1.785 | 0.314 |
| Progression of arterial lesions | 0.518 | 0.155-1.733 | 0.286 |
|
| |||
| rs1360780 | 0.785 | 0.250-2.465 | 0.679 |
| Sustained remission | 0.565 | 0.149-2.140 | 0.401 |
| bDMARDs | 2.184 | 0.666-7.164 | 0.198 |
| Vascular interventions | 1.251 | 0.318-4.931 | 0.749 |
| Worsening glucose tolerance | 9.503 | 2.220-40.676 | 0.002* |
| GC-induced hyperlipidemia | 0.643 | 0.181-2.287 | 0.495 |
| Worsening hypertension | 0.583 | 0.177-1.924 | 0.376 |
| Progression of arterial lesions | 0.504 | 0.146-1.745 | 0.280 |
|
| |||
| BclI | 1.014 | 0.325-3.164 | 0.981 |
| Sustained remission | 0.639 | 0.174-2.342 | 0.499 |
| bDMARDs | 1.974 | 0.627-6.216 | 0.245 |
| Vascular interventions | 1.132 | 0.296-4.327 | 0.856 |
| Worsening glucose tolerance | 9.287 | 2.223-38.793 | 0.002* |
| GC-induced hyperlipidemia | 0.585 | 0.167-2.054 | 0.403 |
| Worsening hypertension | 0.545 | 0.167-1.775 | 0.313 |
| Progression of arterial lesions | 0.500 | 0.149-1.675 | 0.261 |
| NR3C1 9β | |||
| 9β | 4.371 | 1.042-18.341 | 0.044* |
| Sustained remission | 0.863 | 0.225-3.314 | 0.830 |
| bDMARDs | 2.102 | 0.636-6.952 | 0.223 |
| Vascular interventions | 1.335 | 0.343-5.201 | 0.677 |
| Worsening glucose tolerance | 10.227 | 2.295-45.581 | 0.002* |
| GC-induced hyperlipidemia | 0.354 | 0.085-1.474 | 0.354 |
| Worsening hypertension | 0.618 | 0.179-2.139 | 0.448 |
| Progression of arterial lesions | 0.622 | 0.177-2.191 | 0.448 |
| Variables | OR | 95% CI |
|
|---|---|---|---|
|
| |||
| rs1119328 | 0.899 | 0.281-2.878 | 0.858 |
| IV methylprednisolone pulse therapy | 2.894 | 0.697-12.021 | 0.144 |
| bDMARDs | 0.274 | 0.070-1.068 | 0.062 |
| Sustained remission | 3.395 | 1.006-11.458 | 0.049* |
| Vascular interventions | 1.038 | 0.305-3.527 | 0.953 |
| Acute ischemic events | 1.342 | 0.410-4.394 | 0.626 |
| Angiographic type V | 0.629 | 0.188-2.101 | 0.451 |
|
| |||
| rs1360780 | 1.637 | 0.534-5.021 | 0.389 |
| IV methylprednisolone pulse therapy | 2.934 | 0.718-11.993 | 0.134 |
| bDMARDs | 0.304 | 0.079-1.172 | 0.084 |
| Sustained remission | 3.256 | 0.938-11.306 | 0.063 |
| Vascular interventions | 1.037 | 0.291-3.690 | 0.956 |
| Acute ischemic events | 1.320 | 0.379-4.594 | 0.663 |
| Angiographic type V | 0.568 | 0.167 -1.928 | 0.364 |
|
| |||
| BclI | 1.688 | 0.541-5.265 | 0.367 |
| IV methylprednisolone pulse therapy | 3.130 | 0.762-12.857 | 0.113 |
| bDMARDs | 0.257 | 0.068-0.975 | 0.046* |
| Sustained remission | 3.611 | 1.057-12.332 | 0.040* |
| Vascular interventions | 1.012 | 0.294-3.475 | 0.985 |
| Acute ischemic events | 1.319 | 0.400-4.346 | 0.649 |
| Angiographic type V | 0.590 | 0.174-1.999 | 0.397 |
| NR3C1 9β | |||
| 9β | 1.213 | 0.319-4.606 | 0.777 |
| IV methylprednisolone pulse therapy | 2.906 | 0.707-11.939 | 0.139 |
| bDMARDs | 0.270 | 0.071-1.024 | 0.054 |
| Sustained remission | 3.486 | 1.007-12.067 | 0.049* |
| Vascular interventions | 1.034 | 0.303-3.528 | 0.957 |
| Acute ischemic events | 1.282 | 0.374-4.393 | 0.693 |
| Angiographic type V | 0.645 | 0.190-2.192 | 0.483 |
- —Fundação de Amparo à Pesquisa do Estado de São Paulo 10.13039/501100001807
- —Sociedade Brasileira de Reumatologia 10.13039/100030774
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Systemic Lupus Erythematosus Research · Vasculitis and related conditions
Highlights
Worsening glucose tolerance and the carriage of 9β of the NR3C1 gene were risk factors for acute ischemic events in TAK.Carriage of 9β of the NR3C1 gene was associated with a higher median of GC-related adverse events.Other polymorphisms of NR3C1, FKBP5 and HSD11B1 genes were not associated with outcomes in TAK.
Introduction
Takayasu arteritis (TAK) is a chronic granulomatous systemic vasculitis, with no defined etiology, that affects large vessels, involving the aorta and its main branches, as well as pulmonary arteries (1). The inflammatory process begins in the adventitia and progresses to all layers of the artery, resulting in concentric thickening of the arterial wall that may lead to structural changes such as stenosis, occlusion, dilatation or aneurysm (2).
The treatment of TAK is mainly based on glucocorticoid (GC) use in association with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) or biological DMARDs (bDMARDs) (3–6). The long-term use of GC in TAK patients leads to an array of adverse events (AEs) that differ widely between patients and different strategies should be applied to minimize the burden of GC toxicity (7, 8).
Pharmacogenomics is an area of genetics that assesses the influence of individual genetic profiles on the effectiveness and AEs of therapeutic agents. It may be applied to the management of several diseases and is useful the individualization of treatment according to genetic variability in drug receptors or in enzymes involved in drug metabolism (9).
Tissue sensitivity to GC may be affected by different variables linked to pharmacogenomics. Firstly, the regulation of GC bioavailability may be influenced by the conversion of cortisone into cortisol, the active form of GC, by 11β hydroxysteroid dehydrogenase type 1 (11βHD1), an enzyme found mainly in the liver and the adipose tissue (10). Then, GC is bound to its receptors and its signaling pathways are activated as it exerts immunosuppressive, anti-inflammatory, and antiallergic effects on different immune cells through genomic and non-genomic mechanisms (11).
The polymorphism rs11119328 of the HSD11B1 gene is an intronic variant (C>A/C>T) commonly found in the general population with a minor allele A frequency ranging between 0.186 and 0.236. This polymorphism reduces the expression of the 11βHD1 enzyme and results in lower bioavailability of the activated cortisol (12). In patients with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, the carriage of rs11119328 was associated with an increased relapse rate (13).
The FKBP5 gene is located in the short arm of chromosome 6 (6p21) and composed of 10 exons. To date, several intronic FKBP5 polymorphisms have been described, especially rs1360780 (T>A/T>C) which is located in intron 2 (14). The T allele carriage leads to decreased tissue sensitivity to GC, and it is associated with psychiatric conditions including depression, borderline personality disorder, post-traumatic stress and suicidality (15). Indeed, decreased GC sensitivity is associated with psychiatric events (16).
Activated cortisone exerts its genomic effect by binding to GC receptors in the soluble and inactivated form in the cytoplasm of nucleated cells. The NR3C1 gene encodes the glucocorticoid receptor (GR) and is located in the long arm of chromosome 5 (5q31.3) with 9 exons and 4.1kb (12, 13). The NR3C1 gene is very polymorphic; some of its polymorphisms have a functional impact on the effects of cortisol and the pharmacodynamics of exogenous GC. Tissue sensitivity to GC is increased upon the carriage of rs56149945 (N363S) and rs41423247 (BclI) polymorphisms of the NR3C1 gene, while the polymorphisms rs6189 (ER22/23EK), rs6190 (ER22/23EK) and rs6198 (GR-9β) lead to decreased GC sensitivity (17). Furthermore, rs10052957 (TthIII1), another polymorphism in the promoter region of the NR3C1 gene, is characterized by the single base change of cytosine for a thymine (C>T) (18). TthIII1 alone does not impact GC sensitivity, but the concomitant carriage with ER22/23EK decreases GC sensitivity (19).
This study aims to evaluate different polymorphisms of the NR3C1, FKBP5 and HSD11B1 genes and their impact on the clinical outcomes of TAK and GC-related AEs.
Patients and methods
Study design and patients
We carried out a retrospective cohort study with prospective genetic analysis, including 81 TAK patients who were selected from the Vasculitis Outpatient Clinic of the Rheumatology Division at the Universidade Federal de São Paulo/Escola Paulista de Medicina (Unifesp/EPM) between March 2022 and August 2023. The inclusion criteria were age ≥ 18 years, fulfilment of the 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology criteria for TAK (20), treatment with GC at any stage after diagnosis of the disease and written informed consent. Patients with chronic infectious diseases or systemic inflammatory/autoimmune diseases associated with TAK were excluded. The study protocol was approved by the Institutional Ethics Committee of Unifesp/EPM (CAAE: 45377121.5.0000.5505) and all study procedures were carried out according to the Declaration of Helsinki and its updates.
Data collection
Patients’ information was collected from the medical records during their follow-up between the years 2014 and 2023. Details about clinical characteristics and outcome measures evaluated in the study are depicted in Supplementary Table S1. Relevant comorbidities for mortality risk were scored using the Charlson Comorbidity Index (21). Adverse events attributed to GC use were defined according to the Glucocorticoid Toxicity Index (GTI), as shown in Supplementary Table S2. The GC-related AEs included GC-induced hyperlipidemia, worsening systemic hypertension, worsening glucose tolerance, deterioration of bone mineral density (BMD), weight gain, cataract, skin lesions and severe infection. Worsening glucose tolerance included patients with previous diagnosis of diabetes, and those who developed hemoglobin A1c above 5.7% after GC therapy (22). Permanent damage related to TAK was assessed using two tools: the Vasculitis Damage Index (VDI) and the Takayasu Arteritis Damage Score (TADS) (23, 24). Stable disease in TAK was defined as the absence of disease relapse or of the development of new arterial lesions in previously unaffected vascular territories during follow-up (25).
Genotyping and determination of haplotypes
After DNA extraction from the peripheral blood, genotyping was carried out in the Genetics Laboratory at UNIFESP-EPM. Polymorphism genotyping was performed using the Sanger sequencing method. The following polymorphisms were evaluated TthIII1 (rs10052957), ER22/23EK (rs6189/6190), N363S (rs56149945) BclI (rs41423247) and 9β (rs6198) in the NR3C1 gene; rs11119328 in the HSD11B1 gene; and rs1360780 in the FKBP5 gene. The haplotypes (HT) of the polymorphisms in the NR3C1 gene were determined by the PHASE software as previously reported (13, 26). HT0 was defined as the absence of any of the above-mentioned polymorphisms, HT1 as the presence of the minor allele of BclI, HT2 as the presence of the minor allele of TthIII1 and BclI, and HT3 as the presence of the minor allele of TthIII1 and 9ß. Other NR3C1 HT with a frequency below 5% were not analyzed. Figure 1 depicts the location of the SNP of the NR3C1 gene and all HT evaluated.
Description of the haplotypes of the NR3C1 gene and their respective frequencies. Nucleotide exchanges are indicated in red.
Statistical analysis
Descriptive statistics included mean and standard deviation or median and interquartile range (IQR), for quantitative variables and frequency with proportion, for categorical variables. Continuous variables were compared for two groups using Student’s t-test for normally distributed variables or Mann-Whitney’s U test for variables with non-Gaussian distribution. Comparisons among three groups for continuous variables were performed using the Kruskal-Wallis test or by the one-way analysis of variance (ANOVA). The analysis of covariance (ANCOVA) was used to compare the cumulative prednisone dose adjusted for the duration of therapy between the carriers and non-carriers of each polymorphism and haplotypes. Categorical variables were evaluated using the chi-square test or Fisher’s exact test. Multivariate logistic regression models were built to evaluate predictors of acute arterial ischemic events and stable disease (i.e., no new arterial lesions during follow-up), and results were expressed as odds ratios (OR) with 95% confidence intervals (95% CI). The accepted significance level was 5% (p-value < 0.05). The IBM SPSS software for Windows version 21.0 (Armonk, NY) was used to perform statistical analysis of the data. GraphPad Prism for Windows version 9.0 (Boston, MA) was used to build graphs. The Hardy-Weinberg equilibrium assessment was performed using R Software version 4.3.2.
Results
Characteristics of TAK patients
Eighty-one TAK patients were included in the study. Figure 2 describes patients’ inclusion in the study, as well as polymorphisms and haplotypes assessed in the study. The patients were mostly female (90.1%) and had a mean age of 29.6 ± 11.4 years, and a median of 85.0 months (54.0-103.0) of follow-up. Acute arterial ischemic events were observed in 28.4% of the patients and coronary artery disease was more common than stroke or transient ischemic attacks. Table 1 describes the disease characteristics and ischemic events of TAK patients. Most patients were Whites or Mestizos (i.e., 84% of study participants). Angiographic type V was the most frequent type (71.6%), according to the classification of Hata and Numano (27), followed by types I (13.6%), IV (7.4%) and IIb (4.9%) (Table 1).
Flowchart of inclusion of patients in the study and analysis of the different polymorphisms and haplotypes.
Approximately half of the patients had progressive arterial lesions (i.e., the development of arterial lesions in previously unaffected territories) during the follow-up period (51.9%). TAK patients presented renovascular hypertension (23.5%), pulmonary artery involvement (17.3%) and subclavian steal syndrome (16.0%) (Table 1). At the end of the follow-up, the median and IQR were [2.0 (1.0-3.0)] for the Charlson Comorbidity Index, [2.0 (2.0-4.0)] for VDI and [5.0 (3.0-7.0)] for TADS.
Regarding TAK therapy with csDMARDs, methotrexate, leflunomide and azathioprine were used at any time during the follow-up in 73 (90.1%), 54 (66.6%) and 27 (33.3%) patients, respectively. On the other hand, bDMARDs, mostly TNF inhibitors, were prescribed for 55.6% of the patients.
GC-related AEs
At the end of the follow-up, the median cumulative prednisone dose was 10,741.00 mg (5,840.63-22,547.88) and the median GTI score was 46.0 (19.0-76.0). At least one GC-related AE was observed in 82.7% of patients, and the median number of GC-related AEs was 2.0 (1.0-3.0). The frequencies of GC-related AEs were as follows: GC-induced hyperlipidemia (50.6%), worsening systemic hypertension (27.2%), worsening glucose tolerance (19.8%), deterioration of BMD (19.8%), weight gain (13.6%), severe infection (8.6%), skin lesions (6.2%), and cataract (3.7%). Among patients with worsening glucose tolerance, 81.3% had had a previous diagnosis of diabetes and needed to increase their diabetic medication, whereas 18.7% developed HbA1c levels above 5.7% upon GC therapy. Osteonecrosis of the femoral head and GC-induced psychosis were rare complications of GC therapy as they were each observed in only one TAK patient.
Genotyping of TAK patients for the HSD11B1, FKBP5 and NR3C1 polymorphisms
The minor allele frequencies of the HSD11B1 and FKBP5 gene polymorphisms (i.e., rs11119328 and rs1360780) were 33.3% and 55.6%, respectively, while the minor alleles of NR3C1 polymorphisms were found in 37.0% for BclI, 19.7% for 9β, 3.7% for ER22/23EK and 1.2% for N363S. The minor alleles were predominantly in heterozygosis. The minor allele of the TthIII1 polymorphism was present in 41.3% of TAK patients. Supplementary Table S3 depicts the number of TAK patients who are homozygous and heterozygous for each polymorphism of HSD11B1, FKBP5 and NR3C1 genes. The rs11119328, rs1360780, BclI and 9β alleles were all in Hardy-Weinberg equilibrium. The frequencies of HT1, HT2 and HT3 of the NR3C1 gene were 20%, 15% and 15% respectively. HT4 and HT5 were only found in 2 and 1 TAK patients, respectively.
The frequency of minor alleles of the HSD11B, FKBP5 and NR3C1 genes was compared among the ethnic groups (i.e., Whites, Mestizos and Blacks) with TAK. No significant differences were found in the carriage of the minor alleles of HSD11B, FKBP5 and NR3C1 genes among ethnic groups of TAK patients (Supplementary Table S4). These analyses did not include Asians since only three individuals had an Asian background in this study. Each of the rs1119382, rs1360780 and BclI polymorphisms was found in only one Asian patient. The 9β and TthIII1 polymorphisms of the NR3C1 gene were not found in Asians.
Associations between the carriage of HSD11B1, FKBP5 and NR3C1 polymorphisms and the outcomes of TAK
No significant associations were found between the carriage of the polymorphisms rs11119328 of HSD11B1, rs1360780 of FKBP5, and BclI and 9β of NR3C1 and disease features or outcomes of TAK such as angiographic type V, subclavian steal syndrome, renovascular hypertension, pulmonary artery involvement, sustained remission, need for therapy with bDMARD, progressive arterial lesions, TADS score, VDI, and need for vascular interventions (Tables 2, 3). Additionally, comparisons between carriers and non-carriers of HSD11B1, FKBP5, and BclI polymorphisms yielded no significant results in regard to GC-related AEs, severe infections, GTI score, CCI and cumulative prednisone dose (Tables 2, 3). However, carriers of the 9β polymorphism had a higher median number of GC-related AEs compared to non-carriers (Table 3).
For specific GC-related AEs as defined by the GTI, such as worsening lipid profile, exacerbation of hypertension, worsening glucose tolerance, deterioration of BMD, weight gain, cataracts, and skin lesions, only 9β carriers had a higher frequency of weight gain than non-carriers (37.5% vs. 8.9%; p = 0.012) (Supplementary Table S5). No other significant differences were found concerning the carriage of other polymorphisms (i.e., rs11119328 of HSD11B1, rs1360780 of FKBP5 and BclI of NR3C1) and specific GC-related AEs (Supplementary Tables S5, S6).
Due to the low frequencies of ER22/23EK and N363S polymorphisms among TAK patients, no further analyses were performed for TAK features, outcomes and GC-related AEs.
NR3C1 gene haplotypes in TAK patients
Table 4 compares the outcomes of TAK and GC-related AEs among TAK patients carrying HT1, HT2, and HT3 of the NR3C1 gene. Despite significant differences in the median number of GC-related AEs among HTs (p = 0.032), we only found a tendency for a higher median number of GC-related AEs in carriers of HT3 compared to the carriers of HT1 and HT2 (p = 0.025 and p = 0.020; respectively) (Bonferroni’s correction – p = 0.016) in the post-hoc analyses. For specific GC-related AEs (Supplementary Table S7), only a tendency for a higher frequency of weight gain was observed in HT3 compared to HT1 carriers (33.3% vs. 0.0%; p = 0.028) in the post-hoc analysis. No differences were found between HT2 and HT3 carriers regarding weight gain (9.1% vs. 33.3%; p > 0.05). No other significant differences were observed among HT1, HT2 and HT3 carriers (Table 4, Supplementary Table S7).
Predictors of ischemic arterial events in patients with TAK
We built multivariate logistic regression models to analyze predictors of acute ischemic events and stable disease (i.e., no disease relapses or progression of arterial lesions) in TAK. In the regression models, we evaluated one of the following polymorphisms: rs11119328 of HSD11B1, rs1360780 of FKBP5 and BclI of NR3C1 gene with other relevant independent variables.
In the regression models for acute ischemic events, we included sustained remission, bDMARD use, vascular interventions, worsening glucose tolerance, GC-induced hyperlipidemia, worsening systemic hypertension, progression of arterial lesions and each polymorphism as independent variables. In all the regression models, worsening glucose tolerance was an independent risk factor for acute ischemic events in TAK. However, in the regression model with the 9β polymorphism of NR3C1, both worsening glucose tolerance and 9β carriage were predictors of acute ischemic events in TAK (Table 5).
In the models analyzing predictors for stable disease in TAK, we added methylprednisolone use, bDMARDs, sustained remission, vascular interventions, acute ischemic events, angiographic type V and each polymorphism as independent variables. In these regression models, no polymorphisms were predictors of stable disease. In all but one regression model, sustained remission was associated with stable disease in TAK, and in one of the regression models, the use of bDMARDs was inversely associated with stable disease (Table 6).
Discussion
In this study, the carriage of 9β and worsening glucose tolerance were independent risk factors for acute arterial ischemic events in TAK. In addition, 9β carriers were associated with a higher median number of GC-related AEs compared to non-carriers. No significant associations were found between the “other” polymorphisms of NR3C1, FKBP5, and HSD11B1 genes and TAK features or outcomes. None of the polymorphisms of NR3C1, FKBP5, and HSD11B1 genes, besides 9β, were associated with GC-related AEs. No significant associations were found between NR3C1 HTs and TAK features, outcomes and GC-related AEs. None of the polymorphisms of NR3C1, FKBP5, and HSD11B1 were predictors of stable disease (i.e., no angiographic progression).
This is the first study to evaluate the frequencies of the polymorphisms of the NR3C1, FKBP5, and HSD11B1 genes in TAK and their associations with TAK features, outcomes, and GC-related AEs. We assessed whether, from a genetic point of view, GC sensitivity had any impact on TAK outcomes. Patients presenting decreased GC sensitivity required higher daily prednisone doses than usual to control disease activity, resulting in a higher burden of GC-related AEs, whereas patients presenting increased GC sensitivity required lower daily prednisone doses to control disease activity, possibly leading to a lower risk of developing AEs (28).
TAK therapy is based on long-term use of GC, resulting in high cumulative GC doses and the development of GC-related AEs (29). Furthermore, acute ischemic arterial events, mainly involving the cerebral and coronary territories, are common complications of TAK (30). Therefore, the evaluation of polymorphisms in the NR3C1, FKBP5 and HSD11B1 genes and their associations with clinical outcomes of TAK patients is of paramount importance for clinical practice. The carriage of specific polymorphisms indicates susceptibility to increased GC toxicity or a favorable therapeutic response.
The 9β polymorphism is associated with decreased GC sensitivity (31), which in theory may be related to poor control of disease activity upon GC therapy and hypothetically may lead to an increased risk of progression of arterial lesions and development of ischemic events. Therefore, the need for longer and higher GC doses to control disease activity may result in a higher frequency of GC-related AEs. This assumption aligns with the findings of our cohort, as 9β carriers had a higher median number of AEs and more frequent weight gain. Furthermore, 9β carriage was an independent risk factor for developing acute ischemic arterial events in patients with TAK, regardless of the risk factors for coronary artery disease.
In the literature, carriage of the 9β variant has been reported to be associated with systemic inflammatory conditions. The 9β variant has been shown to increase the chance of developing rheumatoid arthritis (32). In ANCA-associated vasculitis, this NR3C1 variant is associated with an increased mortality rate and a higher chance of end-stage renal disease (13). This evidence points to poor control of the inflammatory process associated with the carriage of the 9β polymorphism, despite therapy. In addition, TAK patients present metabolic syndrome more frequently than healthy controls and the excessive number of risk factors for cardiovascular disease may be a confounding factor when analyzing the influence of 9β on acute arterial ischemic events (33, 34). Nonetheless, the carriage of 9β polymorphism and worsening glucose tolerance were independent predictors of this severe complication in our study. It has been reported that HT3 of the NR3C1 gene, which contains the 9β polymorphism, is related to increased cardiovascular risk with increased inflammatory cytokines and carotid intima-media thickening in the general population (35). Conversely, a study of a multiethnic population in the Netherlands did not find any associations between 9β carriage and the age of onset of diabetes or metabolic parameters (36).
The NR3C1 polymorphisms N363S, BclI, and 9β and their relationships with disease activity parameters were evaluated in patients with rheumatoid arthritis. The carriage of the minor allele of BclI or N363S (i.e., both increase GC sensitivity) was associated with lower baseline levels of disease activity (37). Conversely, the carriage of BclI increased the frequency of central nervous system manifestations, especially psychiatric symptoms, in patients with systemic lupus erythematosus (38).
Since the NR3C1 gene is very polymorphic, it is worth mentioning that the carriage of polymorphisms with antagonist functions may result in nullified effects on GC sensitivity. Therefore, haplotypic analysis of the NR3C1 gene may be more relevant compared to the analyses of individual polymorphisms. In our study, we evaluated only three haplotypes of the NR3C1 gene (i.e., HT1, HT2 and HT3) since the frequencies of the other HTs, such as HT4 and HT5, were too low for further analyses. HT3 carriage encompasses the combination of the polymorphisms 9ß and TthIII1 in the NR3C1 gene. The carriage of HT3 in TAK patients led to a trend for more frequent GC-related AEs compared to the carriage of other HTs, and a trend for a higher frequency of weight gain than HT1 carriage. The similarity of findings in the analysis of HT3 and the 9ß polymorphism indicates that the intronic variant Tthlll1 had little effect on the GC-decreased sensitivity exerted by 9ß. Indeed, the carriage of the polymorphism 9β was an independent risk factor for acute ischemic events in TAK patients. In all logistic regression models evaluating predictors of ischemic events in TAK, worsening glucose tolerance, as described by the GTI, was an independent risk factor for acute ischemic arterial events. This is in line with the evidence in the literature that diabetes is a major risk factor for acute ischemic events in the general population (39).
The variants BclI and N363S in the NR3C1 gene are associated with increased sensitivity to GC, whereas 9β and ER22/23EK polymorphisms are associated with a decreased GC sensitivity (40). In this study, the most frequent polymorphisms of the NR3C1 gene among TAK patients were BclI and 9β, which have antagonist effects regarding GC sensitivity. This is in line with previous reports in the literature, where the frequencies of the minor alleles in these polymorphisms in the dbSNP database vary from 16 to 36% and from 1 to 24%, respectively (41, 42). On the other hand, the rare NR3C1 polymorphisms, described in 0-3% of individuals in databases that include data on Brazil, were infrequent among TAK patients, since only 3 individuals were carriers of the ER22/23EK polymorphism and only one patient had the N363S polymorphism (43, 44). The frequency of the minor allele in the intronic variant TthIII1 was 41.3% in TAK patients. This finding is consistent with the wide range of frequencies (1.9-60.7%) reported for different populations (45).
The minor allele of the rs11119328 polymorphism in the HSD11B1 gene is associated with a decreased expression of the 11βHD1 enzyme and lower conversion of inactive cortisone into active cortisol. Theoretically, rs11119328 polymorphism, which has been studied in a few disorders, induces poor disease control in patients with systemic inflammatory diseases, and it has been studied in a few disorders. In ANCA-associated vasculitis, the carriage of rs11119328 minor allele was associated with a higher risk of disease relapse (13). Furthermore, kidney transplant patients presenting chronic rejection had upregulation of the cortisol-activating HSD11B1 gene, indicating an unmet cortisol demand in chronic kidney transplant rejection. Conversely, lower 11βHD1 activity after discontinuing infliximab use in Crohn’s disease, increased the risk of mid/long-term clinical relapse (46, 47). In our study, the carriage of the rs11119328 A allele had no impact on disease features and outcomes of patients with TAK, as well as on GC-related AEs.
FKBP5 is a polymorphic gene that encodes the protein FKBP5, a co-chaperone protein of the GC receptor (48). Most studies evaluating genetic variants of FKBP5 focused mainly on its relations with psychiatric diseases. The FKBP5 polymorphism of interest in our study was rs1360780, and even though it was found at a high frequency (55.7%) in TAK patients, no significant associations were found with TAK features and outcomes, as well as with GC-related AEs (14, 49). In a related study, no association was observed between rs1360780 and clinical outcomes in idiopathic thrombocytopenic purpura (50). However, rs1360780 carriage has already been described as a risk factor for bronchial asthma (51). No studies, besides ours, have described associations between rs1360780 carriage and outcomes in systemic inflammatory diseases.
Our study has its strengths and limitations. The main strengths are the long-term follow-up of TAK patients and the use of the Sanger technique, which increases precision in detecting genetic variants, for genotyping the polymorphisms of interest. The main limitations of the study are its single-center retrospective design, which is subject to recall bias, and the relatively small number of TAK patients included which limit generalizability of the results. The latter may be due to the rarity of the disease in Brazil (52). Additionally, limitations of this study include the absence of a control group and body mass index data of the participants.
In conclusion, 9β was the only polymorphism of the NR3C1 gene to present significant associations in TAK in this cohort, as its carriage led to a higher frequency of GC-related AEs and weight gain. Worsening glucose tolerance and 9β in the NR3C1 gene carriage were independent risk factors for acute ischemic events in TAK in our patient population. None of the other variants of the NR3C1, HSD11B1 and FKBP5 gene were associated with clinical outcomes or GC-related AEs in TAK.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Souza AW Sde Carvalho JF. Diagnostic and classification criteria of Takayasu arteritis. J Autoimmun. (2014) 48–49:79–83. doi: 10.1016/j.jaut.2014.01.012, PMID: 24461381 · doi ↗ · pubmed ↗
- 2Arnaud L Haroche J Mathian A Gorochov G Amoura Z. Pathogenesis of Takayasu’s arteritis: A 2011 update. Autoimmun Rev. (2011) 11:61–7. doi: 10.1016/j.autrev.2011.08.001, PMID: 21855656 · doi ↗ · pubmed ↗
- 3de Souza AWS Sato EI Brance ML Fernández-Ávila DG Scolnik M Magri SJ. Pan american league of associations for rheumatology guidelines for the treatment of takayasu arteritis. J Clin Rheumatol. (2023) 29:316–25. doi: 10.1097/RHU.0000000000002004, PMID: 37553869 · doi ↗ · pubmed ↗
- 4Keser G Aksu K. What is new in management of Takayasu arteritis? Presse Med. (2017) 46:e 229–35. doi: 10.1016/j.lpm.2016.11.033, PMID: 28774475 · doi ↗ · pubmed ↗
- 5Keser G Direskeneli H Aksu K. Management of Takayasu arteritis: a systematic review. Rheumatol (Oxford). (2014) 53:793–801. doi: 10.1093/RHEUMATOLOGY/KET 320, PMID: 24097290 · doi ↗ · pubmed ↗
- 6Pacheco RL Latorraca CDO Cde Souza AWS Pachito DV Riera R. Clinical interventions for Takayasu arteritis: A systematic review. Int J Clin Pract. (2017) 71(11). doi: 10.1111/ijcp.12993, PMID: 28895653 · doi ↗ · pubmed ↗
- 7Spies CM Strehl Cvan der Goes MC Bijlsma JWJ Buttgereit F. Glucocorticoids. Best Pract Res Clin Rheumatol. (2011) 25:891–900. doi: 10.1016/j.berh.2011.11.002, PMID: 22265268 · doi ↗ · pubmed ↗
- 8Palmowski A Buttgereit F. Reducing the toxicity of long-term glucocorticoid treatment in large vessel vasculitis. Curr Rheumatol Rep. (2020) 22(12):85. doi: 10.1007/S 11926-020-00961-0, PMID: 33047263 PMC 7550368 · doi ↗ · pubmed ↗