A retrospective study on factors associated with COVID-19 vaccine refusal among individuals aged 15 years and above in the general population of Bamenda I sub-division, Cameroon
Yamssi Cédric, Noumedem Anangmo Christelle Nadia, Abongwa Delight Chewah, Wenjuan Liu, Ye Liu, Tako Djimefo Alex Kevin, Vincent Khan Payne, Haibo Hu

TL;DR
This study in Cameroon found that many people refused the COVID-19 vaccine due to concerns about side effects and low knowledge, highlighting the need for better education.
Contribution
The study identifies socio-demographic and knowledge-related factors linked to vaccine refusal in a specific Cameroonian population.
Findings
Most participants (87.9%) were unvaccinated, with significant associations between vaccine refusal and age, gender, and education.
A majority of participants (80.8%) were concerned about vaccine side effects, and many believed vaccines were promoted for financial reasons.
Only 12.1% of participants were vaccinated, indicating a need for targeted educational interventions to improve vaccination rates.
Abstract
By the end of 2020, several vaccines aimed at combating COVID-19 were authorized for widespread immunization. The aim of this study was to assess the factors that were associated with COVID-19 Vaccine refusal in Bamenda I. This was a retrospective study carried out in the subdivision of Bamenda I, from March to June 2024, through interviews and questionnaires in which participants were asked to recall important events during the COVID-19 pandemic. A questionnaire-based survey was conducted to ensure diverse representation in the community study. The questionnaire comprised four sections: socio-demographic characteristics, knowledge about COVID-19 and vaccines, attitudes toward COVID-19, and beliefs about the vaccine. Data were collected during community gatherings, such as focus group discussions and training sessions, and also through Google Forms via the Kobo tool for participants…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
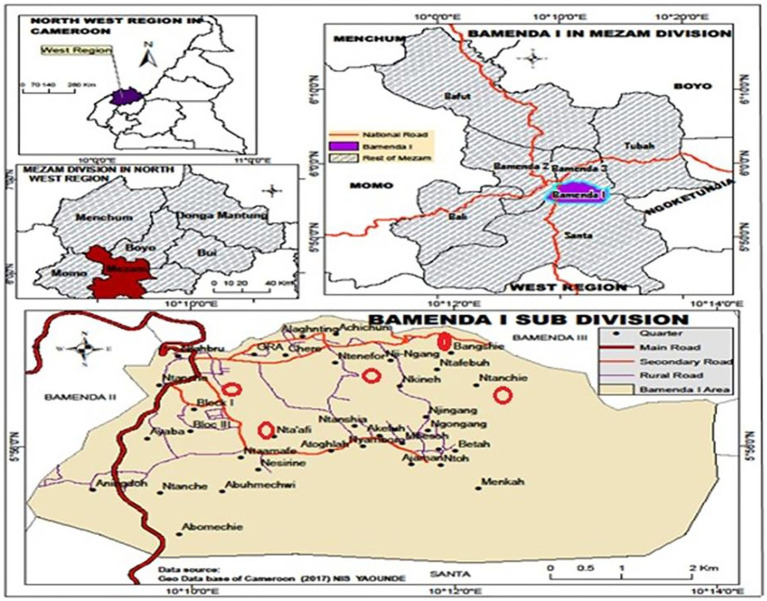 Figure 1
Figure 1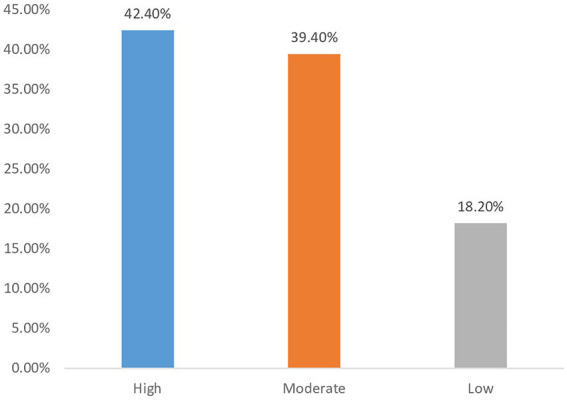 Figure 2
Figure 2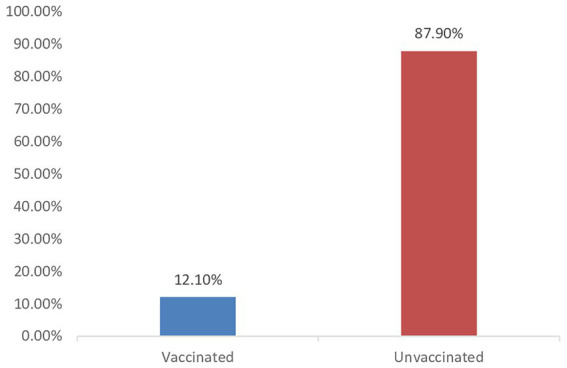 Figure 3
Figure 3| Variable | Modality | Frequency | Percentage |
|---|---|---|---|
| Age | 15–20 | 88 | 44.4 |
| 21–30 | 66 | 33.3 | |
| 31–40 | 34 | 17.2 | |
| 40 and above | 10 | 5.1 | |
| Gender | Male | 94 | 47.5 |
| Female | 104 | 52.5 | |
| Education | Primary | 4 | 2.0 |
| Secondary | 52 | 26.3 | |
| University | 116 | 58.6 | |
| Not educated | 26 | 13.1 | |
| Profession | Entrepreneur | 40 | 20.2 |
| Health personnel | 18 | 9.1 | |
| Student | 98 | 49.5 | |
| Others | 42 | 21.2 |
| Variable | Modality | Frequency | Percentage |
|---|---|---|---|
| Virus responsible for COVID-19 infection? | Ebola | 4 | 2.0 |
| Corona | 188 | 94.9 | |
| Hepatitis A | 6 | 3.0 | |
| Herpes simplex | 0 | 0.0 | |
| Awareness of COVID-19 vaccination center nearby? | Yes | 40 | 20.2 |
| No | 58 | 29.3 | |
| I do not know | 100 | 50.5 | |
| Main reason for COVID-19 vaccine Refusal | Vaccine may be dangerous | 68 | 34.3 |
| Parents refused | 22 | 11.1 | |
| Religion forbids me | 12 | 6.1 | |
| I do not have a reason | 96 | 48.5 | |
| Safety concerns about COVID-19 vaccine? | Yes | 156 | 78.8 |
| No | 42 | 21.2 | |
| Believed in effectiveness of vaccine? | Yes | 88 | 44.4 |
| No | 110 | 55.6 | |
| COVID-19 is a serious public health threat? | Yes | 148 | 74.7 |
| No | 50 | 25.3 | |
| Preventive measures against COVID-19? | Covid 19 vaccine | 34 | 17.2 |
| Hand washing | 26 | 13.1 | |
| Nose masks | 34 | 17.2 | |
| Herbal remedies | 28 | 14.1 | |
| All of above | 76 | 38.4 | |
| COVID-19 vaccine development was rushed? | Yes | 100 | 50.5 |
| No | 98 | 49.5 | |
| Encountered misinformation about the COVID-19 vaccine? | Yes | 106 | 53.5 |
| No | 92 | 46.5 |
| Variable | Modality | Frequency | Percentage |
|---|---|---|---|
| Any underlying health conditions? | Yes | 34 | 17.2 |
| No | 164 | 82.8 | |
| COVID-19 vaccine is a personal choice or a public health responsibility | Personal choice | 129 | 65.2 |
| Public health responsibility | 69 | 34.8 | |
| Worried about potential side effects of the COVID-19 vaccine? | 1 | 160 | 80.8 |
| 2 | 38 | 19.2 | |
| Believed that natural immunity is better than vaccine-induced immunity? | Yes | 130 | 65.7 |
| No | 68 | 34.3 | |
| Concerned about the long-term effects of the COVID-19 vaccine? | Yes | 136 | 68.7 |
| No | 62 | 31.3 | |
| COVID-19 vaccine is unnecessary now that the pandemic has slowed down? | Yes | 106 | 53.5 |
| No | 92 | 46.5 | |
| Heard about any potential religious or ethical concerns related to the COVID-19 vaccine? | Yes | 84 | 42.4 |
| No | 114 | 57.6 | |
| Did vaccine hesitancy contribute to the spread of COVID-19? | Yes | 80 | 80.4 |
| No | 118 | 59.6 |
| Variable | Modality | Frequency | Percentage |
|---|---|---|---|
| Discuss risks/benefits of the vaccine with healthcare worker if pregnant, planning to conceive | Strongly agree | 54 | 27.3 |
| Agree | 68 | 34.3 | |
| Neutral | 50 | 25.3 | |
| Disagree | 22 | 11.1 | |
| Strongly disagree | 4 | 2.0 | |
| Receive next COVID-19 dose while breastfeeding | Strongly agree | 20 | 10.1 |
| Agree | 32 | 16.2 | |
| Neutral | 90 | 45.5 | |
| Disagree | 34 | 17.2 | |
| Strongly disagree | 22 | 11.1 | |
| Advice family and friends to be vaccinated. | Strongly agree | 18 | 9.1 |
| Agree | 42 | 21.2 | |
| Neutral | 80 | 40.4 | |
| Disagree | 34 | 17.2 | |
| Strongly disagree | 24 | 12.1 | |
| Receive vaccine if required for travel purposes? | Yes | 106 | 53.5 |
| No | 92 | 46.5 |
| Variable | Modality | Frequency | Percentage |
|---|---|---|---|
| COVID-19 vaccine should not be given to older adults | Strongly agree | 14 | 7.1 |
| Agree | 38 | 19.2 | |
| Neutral | 76 | 38.4 | |
| Disagree | 50 | 25.3 | |
| Strongly disagree | 20 | 10.1 | |
| Stop following other preventive measures after first dose? | Strongly agree | 18 | 9.1 |
| Agree | 48 | 24.2 | |
| Neutral | 50 | 25.3 | |
| Disagree | 46 | 23.2 | |
| Strongly disagree | 36 | 18.2 | |
| Measures taken to address vaccine refusal and hesitancy? | Mandatory | 58 | 29.3 |
| Not necessary to force people | 122 | 61.6 | |
| Isolate unvaccinated people | 18 | 9.1 | |
| COVID-19 vaccination promoted for financial reasons? | Strongly agree | 40 | 20.2 |
| Agree | 34 | 17.2 | |
| Neutral | 72 | 36.4 | |
| Disagree | 40 | 20.2 | |
| Strongly disagree | 12 | 6.1 | |
| COVID-19 vaccines are harmful to women planning to conceive? | Strongly agree | 34 | 17.2 |
| Agree | 62 | 31.3 | |
| Neutral | 86 | 43.4 | |
| Disagree | 12 | 6.1 | |
| Strongly disagree | 4 | 2.0 |
| Variable | Modality | Receive the COVID-19 vaccine | Chi-square | ||
|---|---|---|---|---|---|
| Vaccinated (%) | Unvaccinated (%) | ||||
| Age | 15–20 | 6(3.03) | 82(41.41) |
|
|
| 21–30 | 8(4.04) | 58(29.29) | |||
| 31–40 | 6(3.03) | 28(14.14) | |||
| 40 and above | 4(2.02) | 6(3.03) | |||
| Gender | Male | 16(8.08) | 78(39.39) |
|
|
| Female | 8(4.04) | 96(48.48) | |||
| Education | Primary | 2(1.01) | 2(1.01) |
|
|
| Secondary | 10(5.05) | 42(21.21) | |||
| University | 6(3.03) | 110(55.55) | |||
| Not educated | 6(3.03) | 20(10.10) | |||
| Profession | Entrepreneur | 6(3.03) | 34(17.17) | 3.661 | 0.300 |
| Health personnel | 4(2.02) | 14(7.07) | |||
| Student | 8(4.04) | 90(45.45) | |||
| Others | 6(3.03) | 36(18.18) | |||
| Variable | Modality | Received the COVID-19 vaccine | Chi-square | ||
|---|---|---|---|---|---|
| Vaccinated (%) | Unvaccinated (%) | ||||
| Virus responsible for COVID-19? | Ebola | 0(0) | 4(2.02) | 1.453 | 0.484 |
| Corona | 24(12.12) | 164(82.82) | |||
| Hepatitis A | 0(0) | 6(3.03) | |||
| Herpes simplex | 0(0) | 0(0) | |||
| Awareness of COVID-19 vaccination center nearby? | Yes | 8(4.04) | 32(16.16) | 2.925 | 0.232 |
| No | 6(3.03) | 52(26.26) | |||
| I do not know | 10(5.05) | 90(45.45) | |||
| Main reason for vaccine refusal? | Vaccine may be dangerous | 14(7.07) | 54(27.27) |
|
|
| Parents refused | 2(1.01) | 20(10.10) | |||
| Religion forbids me | 4(2.02) | 8(4.04) | |||
| I do not have a reason | 4(2.02) | 92(46.46) | |||
| Concerned about the safety of the vaccine? | Yes | 12(6.06) | 144(72.72) |
|
|
| No | 12(6.06) | 30(15.15) | |||
| Believed in the effectiveness of the vaccine? | Yes | 20(10.10) | 68(34.34) |
|
|
| No | 4(2.02) | 106(53.53) | |||
| COVID-19 is a serious public health threat? | Yes | 10(5.05) | 138(69.69) |
|
|
| No | 14(7.07) | 36(18.18) | |||
| Some preventive measures against COVID-19? | Covid 19 vaccine | 8(4.04) | 26(13.13) |
|
|
| Hand washing | 4(2.02) | 22(11.11) | |||
| Nose masks | 8(4.04) | 26(13.13) | |||
| Herbal remedies | 0(0) | 28(14.14) | |||
| All of above | 4(2.02) | 72(36.36) | |||
| Was COVID-19 vaccine development was rushed? | Yes | 10(5.05) | 90(45.45) | 2.044 | 0.563 |
| No | 14(7.07) | 84(42.42) | |||
| Encountered COVID-19 vaccine misinformation? | Yes | 14(7.07) | 92(46.46) | 0.253 | 0.615 |
| No | 10(5.05) | 82(41.41) | |||
| Variable | Modality | Received the COVID-19 vaccine | Chi-square | ||
|---|---|---|---|---|---|
| Vaccinated (%) | Unvaccinated (%) | ||||
| COVID-19 vaccine is harmful to women planning to conceive? | Strongly agree | 2(1.01) | 32(16.16) |
|
|
| Agree | 8(4.04) | 54(27.27) | |||
| Neutral | 8(4.04) | 78(39.39) | |||
| Disagree | 2(1.01) | 10(5.05) | |||
| Strongly disagree | 4(2.02) | 0(0) | |||
| Discuss risks/benefits of COVID-19 vaccine with healthcare worker? | Strongly agree | 6(3.03) | 48(24.24) | 1.507 | 0.825 |
| Agree | 8(4.04) | 60(30.30) | |||
| Neutral | 8(4.04) | 42(21.21) | |||
| Disagree | 2(1.01) | 20(10.10) | |||
| Strongly disagree | 0(0) | 4(2.02) | |||
| Receive next dose of vaccine while breastfeeding? | Strongly agree | 8(4.04) | 12(6.06) |
|
|
| Agree | 0(0) | 32(19.16) | |||
| Neutral | 12(6.06) | 78(39.39) | |||
| Disagree | 0(0) | 34(17.17) | |||
| Strongly disagree | 4(2.02) | 18(9.09) | |||
| Advise family and friends to be vaccinated? | Strongly agree | 0(0) | 18(9.09) | 8.155 | 0.086 |
| Agree | 6(3.03) | 36(18.18) | |||
| Neutral | 14(7.07) | 66(33.33) | |||
| Disagree | 4(2.02) | 30(15.15) | |||
| Strongly disagree | 0(0) | 24(12.12) | |||
| Receive vaccine if required for traveling purposes? | Yes | 16 (8.08) | 88(44.4) | 2.329 | 0.312 |
| No | 8(4.04) | 86(43.43) | |||
| Variable | Modality | Received the COVID-19 vaccine | Chi-square | ||
|---|---|---|---|---|---|
| Vaccinated (%) | Unvaccinated (%) | ||||
| COVID-19 vaccine should not be given to older adults | Strongly agree | 4(2.02) | 10(5.05) |
|
|
| Agree | 6(3.03) | 32(16.13) | |||
| Neutral | 8(4.04) | 68(34.34) | |||
| Disagree | 0(0) | 50(25.25) | |||
| Strongly disagree | 6(3.03) | 14(7.07) | |||
| Stop following preventive measures after receiving first dose | Strongly agree | 10(5.05) | 8(4.04) |
|
|
| Agree | 8(4.04) | 40(20.20) | |||
| Neutral | 4(2.02) | 46(23.23) | |||
| Disagree | 0(0) | 46(23.23) | |||
| Strongly disagree | 2(1.01) | 34(17.17) | |||
| Measures taken to address vaccine refusal and hesitancy | Mandatory | 6(3.03) | 52(26.26) | 0.3 | 0.860 |
| Not necessary to force people | 16(8.08) | 106(53.53) | |||
| Isolate unvaccinated people | 2(1.01) | 16(8.08) | |||
| COVID-19 promoted for financial reasons | Strongly agree | 6(3.03) | 34(17.17) | 0.7 | 0.940 |
| Agree | 4(2.02) | 30(15.15) | |||
| Neutral | 8(4.04) | 64(32.32) | |||
| Disagree | 4(2.02) | 36(18.18) | |||
| Strongly disagree | 2(1.01) | 10(5.05) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVaccine Coverage and Hesitancy · SARS-CoV-2 and COVID-19 Research · COVID-19 epidemiological studies
Introduction
1
The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is the agent behind coronavirus disease 2019 (COVID-19), which surfaced in late 2019 and has caused over 5 million deaths and more than 270 million confirmed cases (1). The virus was first identified in December 2019 in Wuhan, Hubei province, China, following a cluster of pneumonia cases of unknown origin (2). It quickly spread globally, leading the World Health Organization (WHO) to declare it a Public Health Emergency of International Concern on January 30, 2020, and later a pandemic on March 11, 2020.
The WHO’s Strategic Preparedness and Response Plan 2021 sought to address the COVID-19 pandemic by strengthening national health systems’ abilities to detect, prevent, and treat the virus (3). Governments and health systems worldwide responded with measures such as lockdowns, social distancing, mask mandates, and mass vaccination campaigns (4). Several vaccines, including mRNA-based and viral vector vaccines, were developed and authorized for emergency use within a year an unprecedented achievement in medical science. The COVAX facility aims to guarantee worldwide access to safe and effective COVID-19 vaccines. As of November 2021, 7.8 billion vaccine doses had been administered worldwide, with Africa receiving 227 million doses (5). COVID-19 has had profound social, economic, and psychological impacts worldwide. It has also spurred major advancements in public health infrastructure, vaccine technology, and global health cooperation (6). As of recent years, the disease has transitioned from a pandemic to an endemic stage in many regions, with ongoing surveillance and vaccination efforts aimed at controlling its spread and impact (7).
COVID-19 vaccine refusal, which differs from vaccine hesitancy, is the deliberate and steadfast unwillingness to vaccinate despite the availability of safe vaccines (8). While hesitancy is defined by delay or indecision, refusal is defined by adamant refusal (9). In most of the African contexts, for instance in Cameroon, refusal of vaccine has been attributed to several factors ranging from doubt in government and public health organizations, concern over side effects, religious or cultural motivations, and dissemination of misinformation and conspiracy theories, most notably through social media (10). Additionally, the perception that COVID-19 poses a localized limited threat has led to lower urgency perception, further contributing to refusal (11). These are more likely based on more general structural and historical concerns, including previous negative encounters with health care systems.
However, despite improvements in vaccine availability, significant hesitancy toward COVID-19 vaccination has hindered efforts to achieve higher immunization rates (12). COVID-19 reached the African continent relatively later than in Asia, Europe, or the Americas. The first confirmed case in Africa was reported in Egypt on February 14, 2020, followed by a rapid spread across the continent (13). Africa’s initial response was marked by swift governmental actions, including border closures, curfews, and public health campaigns, which helped delay the widespread transmission in the early months (14). Despite fears that the continent’s fragile health systems could be overwhelmed, Africa experienced lower reported infection and mortality rates compared to other continents in the initial phases of the pandemic (15). Several factors contributed to this, including a younger population, experience with epidemic responses (e.g., Ebola), and community-based health structures. However, limited testing capacity, underreporting, and disparities in access to health care and vaccines posed significant challenges. Africa exhibited a diverse vaccination uptake, ranging from 6.9 to 97.9% across the continent (16). The prevalence and mortality rates of COVID-19 vary widely among populations due to several factors, including adherence to containment measures, the reliability of diagnostics and reporting systems, demographics, climate, environmental influences, genetic factors, and immunological variations (17). By the end of 2020, several vaccines aimed at combating COVID-19 were expected to be authorized for widespread immunization.
The first confirmed case in Cameroon was a French national who arrived in Yaoundé on March 6, 2020. Since then, various preventive measures have been implemented nationwide, including reducing public transit use, caring for and quarantining those infected or suspected of infection, banning gatherings larger than 50 people, regulating consumer flow in markets and supermarkets, conducting virtual meetings, avoiding physical contact like handshakes, and covering mouths while sneezing (18). Cameroon’s nationwide vaccination program started on April 12, 2021, utilizing Sinopharm and AstraZeneca vaccines, aiming to vaccinate at least 15 million people (19). The COVID-19 vaccination was to reduce disease-related disability and mortality by controlling the transmission and severity of the SARS-CoV-2 virus.
Additionally, protecting vulnerable populations who cannot be vaccinated is crucial through achieving herd immunity. Herd immunity has successfully eradicated smallpox and other deadly infectious diseases (20). By February 2022, 6.5% of the population in Cameroon, as well as 11.9% in Nigeria had administered at least one dose of COVID-19 vaccine (21). Despite these efforts, Cameroon faced challenges such as limited testing capacity, insufficient health infrastructure, and vaccine hesitancy. Health workers played a vital role in community outreach and awareness campaigns (22). The national COVID-19 vaccination campaign began in April 2021, using vaccines such as Sinopharm, AstraZeneca, Johnson & Johnson, and later Pfizer-BioNTech. However, vaccine uptake was slow due to misinformation, skepticism, and logistical constraints (23). By the end of 2022, Cameroon, like many African countries, had transitioned to a more targeted approach focusing on vulnerable populations and integrating COVID-19 management into routine healthcare services (24). The pandemic also highlighted the importance of strengthening health systems, digital health surveillance, and public health preparedness in Cameroon.
Studying COVID-19 vaccine refusal in Bamenda I, Cameroon, is important due to the underlying socio-political, cultural, and public health environment. Bamenda I is situated within a conflict area in the Northwest Region, where government suspicion, poor healthcare access, and misinformation spread are increased (25, 26). These conditions can result in low vaccine uptake, but data on refusal trends are scarce. Understanding the specific drivers of refusal in this setting is needed to develop context-appropriate public health responses, promote vaccine use, and prevent possible future outbreaks not only of COVID-19 but also of other preventable infectious diseases (27). Results from this local research would contribute to general principles guiding risk communication and trust building in health systems for similarly affected communities. The aim of this study was to assess the factors associated with COVID-19 vaccine refusal among individuals aged 15 years and above in Bamenda I Sub-Division, Cameroon.
Materials and methods
2
Study design
2.1
This was a retrospective study carried out in the subdivision of Bamenda I, from March to June 2024, through interviews and questionnaires in which participants were asked to recall important events during the COVID-19 pandemic.
Study area
2.2
The Bamenda I community served as the research study’s current setting. In the Mezam department of the North-West Region of Cameroon, the urban town of Bamenda contains the district commune known as Bamenda I, or Bamenda I as seen on Figure 1. The district of Bamendankwe serves as its capital. One of the three districts that make up the Bamenda Urban Community is the district commune of Bamenda I, which was established in 2007. According to the 2005 census, there were 28,359 people, with 18,468 living in Bamenda Town’s urban area. The three major ethnic groups are the Bamendankwe, Bamilékés, and Bafut. The town is home to four health facilities: a military hospital and camp, the Bamendankwe Health Center in Akefu, the Bamenda Polyclinic Station in Alatining, and the World Hospital in Ayaba.
Map of Bamenda I sub-division.
Sample size determination
2.3
The sample size was calculated using Lorenz’s formula (StatCalc of EPI Info software). Using the prevalence of 10% of a study on the factors associated with COVID-19 vaccine refusal: A community-based study in the Menoua division in Cameroon (28), with an 80% power to detect significant associations or differences and a 5% accepted margin of error, the minimal sample size estimate was 139 participants.
The sample size was calculated using the Lorentz’ formula which is expressed as follows:
Where:
Z = 1.96 (for 95% confidence level).
p = 0.10 (10% prevalence).
d = 0.05 (5% margin of error).
Substituting into the formula:
Therefore, the minimum required sample size is approximately 139 participants (after rounding up).
Sampling technique
2.3.1
A convenience sample method was used, as it is the most suitable selection method for this study.
Inclusion and exclusion criteria
2.3.2
Everyone from 15 years and above, including those who refused to be vaccinated against COVID-19 and were willing to participate were included in the study. Meanwhile, those with incoherent data or incompletely filled questionnaires were excluded. Also, questionnaire was structured based on specific objectives.
Data collection procedure
2.4
A pretest was carried out in the Bamenda I sub-division, involving 10 randomly selected residents aged 15 years and above. The questionnaire was given to them, and following the pretest, complex questions were simplified for easier understanding, leading to the validation of the questionnaire. A questionnaire-based survey was employed in this community-based study to ensure representation across all population categories. The questionnaire was divided into four sections: socio-demographic characteristics, knowledge about COVID-19 and vaccines, attitudes toward COVID-19, and beliefs regarding the COVID-19 vaccine. The first section gathered information on age, gender, education level, and profession, with participants responding by marking the letter that matched their answer. Most questions were closed-ended to facilitate comparison. The second section assessed participants’ knowledge about COVID-19, including the virus itself, preventive measures, awareness of local vaccination centers, concerns about vaccine side effects, and any underlying health conditions that might affect vaccination eligibility. The third section explored whether participants would recommend the vaccine to family and friends, if they would get vaccinated for travel purposes, whether they would cease preventive measures after their first dose, and if they would discuss vaccine risks and benefits with healthcare professionals while pregnant or planning to conceive. Responses were rated on a scale from “Strongly agree” to “Strongly disagree.” The fourth section included questions about whether the COVID-19 vaccine should be administered to older adults, concerns regarding its safety for women planning to conceive, and whether financial motives drive vaccine promotion.
Data collection took place during community gatherings events, including church meetings, health education sessions, market-day gatherings, focus group discussions, and training workshops. These settings provided convenient and trusted spaces within which to invite participants into open discussion about COVID-19 vaccine refusal. Additionally, Google Forms were administered via Kobo Collect to participants with access to Android phones. For those facing language or literacy barriers, we filled out the response sheets after obtaining verbal consent. Participants were informed that their personal information would be kept confidential and that results might be published for academic purposes.
Measurement of COVID-19 vaccine refusal
2.5
COVID-19 vaccine refusal was assessed through a structured questionnaire administered to participants aged 15 years and above residing in Bamenda I Sub-Division.
Participants were asked the direct question: “Have you received the COVID-19 vaccine?”
o Those answering “Yes” were classified as vaccinated. o Those answering “No” were further asked: “If no, what is the main reason you have not been vaccinated?”
Respondents who explicitly stated lack of trust in the vaccine, disbelief in COVID-19, fear of side effects, or outright unwillingness to ever receive the vaccine were categorized as refusers.Respondents citing temporary reasons (e.g., illness, waiting for availability, lack of time, or intention to vaccinate later) were classified as delayers/hesitant.
Associated factors: Socio-demographic characteristics (age, sex, marital status, education, occupation), health status (history of chronic illness, previous COVID-19 infection), and attitudinal factors (knowledge about COVID-19, perception of vaccine safety and effectiveness, trust in health authorities, and exposure to misinformation) were also measured and analyzed for their association with vaccine refusal.
Ethical considerations
2.6
Prior to data collection, ethical clearance was obtained from the Faculty of Health Science (FHS) at the University of Bamenda, with a project identification number (2024/0108H/Uba/IRB). Administrative authorization was also obtained from the North West Regional Delegation of the Ministry of Public Health of Cameroon, the District Health Services, and the directors of the hospitals. During data collection, informed consent was obtained from all participants. For literate individuals, the purpose of the study and their rights were explained verbally, and their oral consent was recorded before beginning the questionnaire. For participants with limited literacy, field workers provided detailed verbal explanations in the participant’s preferred language, ensuring they fully understood the study before consenting. In cases involving minors aged 15–17 years, verbal assent was obtained from the participant along with verbal consent from a parent, guardian, or responsible adult present at the time. All participants were assured that their responses would remain anonymous and confidential, and that their personal data would not be shared. The results would be used strictly for academic research and public health improvement purposes.
Statistical analysis
2.7
The data were subsequently transferred to the Statistical Package for Social Sciences (SPSS) software for analysis. Frequency distribution tables were generated for categorical variables, and the Pearson chi-square test was conducted to assess associations between variables. p < 0.05 were considered statistically significant. Knowledge levels regarding COVID-19 vaccines were categorized into three groups based on participant scores from an ordinal scale. Participants scoring 8 or higher were classified as having a high level of knowledge, those scoring exactly 5 were deemed to have a moderate level, and scores of 3 or 4 indicated a low level of knowledge.
Results
3
Socio-demographic characteristics of the study population
3.1
Table 1 shows the socio-demographic data of participants. The study consisted of 198 respondents who were partitioned according to different age groups which ranged from 15 years and above, who were either male or female. It included adolescents who made up 44.4% of the study population, followed by the young adult population who made up 33.3%, followed by the old adult population who accounted for 17.2%, and finally the oldest population made up 5.1% of the total respondents. It also recorded 47.5% male, and 52.5% female respondents. Two percent of respondents had attained just primary education, 26.3% ended at the level of secondary education, 58.6% had completed their university education, and 13.1% were uneducated. 20.2% respondents were entrepreneurs, 9.1% were health personnel, 49.5% were students, and 21.2% were involved in other professions.
Knowledge of respondents on COVID-19
3.2
Table 2 illustrate the respondents’ knowledge about COVID-19. When asked about the virus causing COVID-19, 2.0% identified it as the Ebola virus, 94.9% correctly named the coronavirus, 6% mentioned Hepatitis A. Regarding the availability of vaccination centers during the peak of the pandemic, 20.2% reported yes, 29.3% said no, and 50.5% were unsure. As for reasons for vaccine refusal, 34.3% thought it was dangerous to their health, 11.1% were restricted by their parents, 6.1% cited religious objections, and 48.5% had no specific reasons. When asked about preventive measures, 17.2% mentioned that the COVID-19 vaccine could help, 13.1% believed hand washing was effective, another 17.2% highlighted wearing masks, 14.1% preferred herbal remedies, and the majority, 38.4%, supported using a combination of all these measures for prevention.
Table 3 assess the level of knowledge respondents had that could influence their reasons for vaccine refusal. When asked if respondents had underlying health conditions that could have prevented them from receiving the vaccine, 17.2% said yes while 82.8% said no. When asked their thoughts about natural immunity and vaccine-induced immunity, 65.7% chose natural immunity, while 34.3% chose vaccine-induced immunity. On finding out if they saw no necessity now that the pandemic has slowed down, 53.5% said yes, while 46.5% disagreed.
Figure 2 shows the overall level of knowledge respondents had on COVID-19 which was measured on a scale of high, medium and low level. From this figure, 42.40% of respondents had a high level of knowledge, 39.40% scored moderately, and 18.20% had low level of knowledge.
Overall level of knowledge of participants about COVID-19.
Participants attitudes toward COVID-19 vaccine
3.3
Table 4 illustrates participants’ attitudes toward the vaccine. On investigating the importance of discussing risks and benefits of the vaccine with healthcare givers if pregnant, planning to conceive or breastfeeding; a majority of 34.3% agreed, 27.3% strongly agreed, 25.3% were neutral, 11.1% disagreed and 2.0% strongly disagreed. Regarding advising their family and friends to get vaccinated, 9.1% strongly agreed, 21.2% agreed, 40.4% were neutral, 17.2% disagreed, and 12.1% strongly disagreed. When asked if they could accept the vaccine in future if required for traveling purposes, 53.5% said yes while 46.5% said no.
Participants beliefs about COVID-19 vaccine
3.4
Table 5 shows the participants beliefs about COVID-19 vaccine. When asked if the vaccine should not be given to older adults, 7.1% strongly agreed, 19.2% agreed, 38.4% were neutral, 25.3% disagreed, and 10.1% strongly disagreed. Upon finding out if preventive measures could stop after receiving first dose of the vaccine, 9.1% strongly agreed, 24.2% agreed, 25.3% were neutral, 23.2% disagreed, and 18.2%strongly disagreed. On finding out from participants what measures can be taken to address COVID-19 vaccine refusal in the community, 29.3% said vaccination should be made mandatory, 61.6% said it will not be necessary to force people, while 9.1% said unvaccinated persons should be isolated from the community. Additionally, on finding out whether COVID-19 vaccination was promoted for financial reasons, 20.2% strongly agreed, 17.2% agreed, 36.4% were neutral, 20.2% disagreed and 6.1% strongly disagreed.
Prevalence of COVID-19 vaccine acceptance
3.5
Figure 3 shows the overall percentage of vaccinated and unvaccinated persons in Bamenda I during the peak of the pandemic. It follows from the analysis of this figure that, 12.10% of the study population were vaccinated, while 87.90% were unvaccinated.
Overall percentage of vaccinated and unvaccinated persons.
COVID-19 vaccine refusal with respect to sociodemographic factors
3.6
Table 6 shows the association between sociodemographic factors and COVID-19 vaccine refusal. The analysis revealed that age, gender, and educational background were significantly associated with vaccine refusal (p < 0.05), indicating that these factors may influence individuals’ decisions regarding COVID-19 vaccination. In contrast, profession did not show a statistically significant association with vaccine refusal (p > 0.05), suggesting that occupational status may not be a determining factor in this context.
COVID-19 vaccine refusal with respect to knowledge of participants
3.7
Table 7 illustrates the association between participants’ knowledge and specific reasons for COVID-19 vaccine refusal. The analysis indicates that factors such as concerns about vaccine safety, doubts about its effectiveness, perceptions of alternative preventive measures, and public health considerations were all significantly associated with vaccine refusal (p < 0.05). These findings suggest that both individual knowledge levels and specific perceived risks play a critical role in shaping attitudes toward COVID-19 vaccination.
COVID-19 vaccine refusal with respect to attitudes
3.8
Table 8 presents the association between participants’ attitudes and COVID-19 vaccine refusal. The results indicate that variables such as the importance of discussing the risks and benefits of receiving the COVID-19 vaccine with a healthcare provider and concerns about receiving the next COVID-19 dose while breastfeeding were significantly associated with vaccine refusal (p < 0.05). These findings highlight the role of healthcare communication and reproductive health considerations in shaping vaccine-related decisions.
COVID-19 vaccine refusal with respect to beliefs
3.9
Table 9 shows the association between participant’s beliefs and COVID-19 vaccine variables such as COVID-19 vaccine should not be given to older adults, after receiving the first COVID-19 vaccine dose should other preventive measures. Beliefs such as; COVID-19 vaccine is harmful to women planning to conceive, stop following preventive measures after receiving the vaccines, and COVID-19 vaccine should not be given to older adults were significantly associated with COVID-19 vaccine refusal.
Discussion
4
Merely 12.10% of people in Bamenda I had received the COVID-19 vaccination. The majority of participants consisted of young people, with 33.3% of the respondents being in their 20s and 30s. Although people aged 20–30 generally have stronger immune systems and are less likely to die from COVID-19, they can still become seriously ill, be hospitalized, or suffer long-term effects (long COVID). The vaccine helps reduce: risk of severe symptoms, risk of hospitalization and risk of long COVID (29). This result is in line with earlier research emphasizing the important impact of age on COVID-19-related knowledge, attitudes, and actions (30). The younger population may have different perceptions of the virus’s risk and susceptibility, which may have an impact on their preventive measures (31). Our results also showed a significant association between age and unwillingness to get the COVID-19 vaccination which is consistent with a study conducted on COVID-19 vaccine hesitancy in peri-urban areas in Kanpur, Uttar Pradesh, India (32). The acceptance of COVID-19 vaccines has demonstrated substantial regional disparities, with reported rates ranging from 36% in Africa to 83% in Oceania (33). Globally, vaccine hesitancy rates have varied considerably, estimated between 23.6 and 97% (34, 35). Within Africa, hesitancy prevalence has been reported at 42.2% in Uganda (36), 53.9% in Ethiopia (37), and 48% across 16 countries on the continent (38). Nigeria reports a hesitancy rate of 49.8% (39), while Arab countries exhibit a rate of 37.6% (40). Outside the African region, the prevalence of vaccine hesitancy includes 19.1% in Canada (41), 20% in both Mexico and India (38), 21.4% in other Indian studies (42), 25.5% in Bangladesh (43), and 33% in Italy (44). These findings emphasize that vaccine hesitancy remains a globally heterogeneous phenomenon, influenced by geographical context (45). Certain demographic groups are disproportionately affected by vaccine hesitancy. Higher rates have been observed among women, individuals with lower educational levels, low-income populations, Black adults, those with comorbid conditions, and residents of rural or semi-urban areas (43). Younger individuals often believe they are less likely to get seriously ill or die from COVID-19 (46). This leads to a lower perceived personal benefit from getting vaccinated, reducing motivation. This contrasts with a study conducted in Venezuela that reported no significant association (47), potentially due to differences in the age groups studied. Additionally, 52.5% of participants were female, indicating a slight gender imbalance favoring women.
Women have generally shown higher COVID-19 vaccination rates than men in many countries, and this trend can be explained by a combination of biological, social, behavioral, and cultural factors. Women are more likely than men to seek healthcare proactively, attend regular checkups, and follow public health advice. This includes being more willing to accept vaccinations as a form of preventive care. Research suggests that gender disparities can influence COVID-19 knowledge and behaviors, with women generally showing greater awareness and commitment to preventive measures (48). The relationship between gender and vaccine refusal in our study was significant, differing from Terry et al.’s (49) findings, which indicated no significant association. This discrepancy may be attributed to the heightened health related concerns and susceptibility to vaccine misinformation often observed among women. Misinformation about the COVID-19 vaccine causing infertility may also contribute to these differences. Regarding education, most respondents (26.3%) had completed secondary school, while 58.6% held university degrees and 13.1% were uneducated. A significant association was found between education level and vaccine refusal.
People with higher education levels often have better health literacy, meaning they are more likely to: understand medical information, assess the risks and benefits of vaccines, recognize misinformation (50). This makes them more likely to trust vaccines and understand their importance. Consistent with other studies on vaccine hesitancy (51), people with higher achievement of education were not as likely to exhibit vaccine reluctance compared to those with lower education levels. Educated individuals are more likely to access information from various sources, enabling them to make informed decisions compared to those with limited literacy skills. Education also helps to dispel misconceptions and cultural practices surrounding health. However, this contrasts with findings from a mixed-methods study in Senegal, which found no meaningful correlation between education and Coronavirus vaccine refusal (52). This discrepancy may stem from the fact that about 97% of Senegalese are Muslim, and there may be a cultural context that de-emphasizes education.
In our study, the occupational distribution revealed that 49.5% of respondents were students. The fact that 49.5% were students suggests that students represent a significant portion of the vaccine-hesitant population in the studied group. This finding is significant, as students particularly those in healthcare fields can play a vital role in raising awareness about COVID-19 and promoting preventive measures within their communities (53).
Our results indicated that most participants had high (42.40%) to moderate (39.40%) levels of knowledge about COVID-19, consistent with a study conducted in Menoua Division, Cameroon, which also found high knowledge levels among participants (28). This similarity may be attributed to greater exposure to COVID-19-related information. However, our findings contrast with those from a study in Venezuela, which reported low to moderate levels of knowledge about the virus, potentially due to inadequate communication and access to vaccination campaigns there (47).
Additionally, our study revealed that many respondents were unaware of nearby COVID-19 centers, with 20.2% indicating knowledge of such facilities. This is inconsistent with the Menoua Division study, where 58.6% of respondents were aware of local vaccination centers (28). This discrepancy might be related to the retrospective nature of our study, as the pandemic’s decline may have led people to forget specifics about vaccination availability. Lack of knowledge regarding healthcare resources can hinder timely diagnosis, treatment, and preventive measures, underscoring the need for enhanced communication and outreach efforts to inform the public about available COVID-19 services.
According to our study, individuals who were immunized against COVID-19 had a greater understanding of the illness and its prevention methods. Specifically, they exhibited higher knowledge levels about COVID-19 and were more aware of the vaccination clinics nearby. In contrast, the unvaccinated group showed a lower comprehension of vaccination and otherpreventative actions, such using masks and washing your hands. Given that evidence shows that vaccination intentions and behaviors are strongly influenced by faith in the safety and efficacy of vaccinations, this knowledge gap could represent a substantial obstacle to vaccine uptake (28, 53).
Our findings indicated that a significant majority (87.90%) of participants were unvaccinated against COVID-19, with 12.10% having received the vaccine. This aligns with the study by Tetsatsi et al. (28), which reported a similar vaccination rate of 10%. In contrast, vaccination acceptance rates were notably higher in Burkina Faso and Nigeria, at 66.53 and 74.47%, respectively, where common reasons for refusal included perceived lack of necessity, safety concerns, and parental opposition. This hesitancy is concerning, as it may facilitate the virus’s further propagation and exacerbate risks for vulnerable populations. Notably, about 26% of women expressed willingness to receive the vaccine while breastfeeding, likely due to widespread misinformation regarding vaccine safety, such as fears about infertility, as noted by Emily Terry et al. (54). The reasons for vaccine hesitancy-safety concerns, perceived ineffectiveness, and exposure to misinformation-are consistent with previous studies on vaccine attitudes and behaviors (55). Addressing these issues through targeted educational campaigns and fostering trust in scientific and public health authorities will be essential for improving COVID-19 vaccination rates and enhancing future pandemic preparedness (51).
In our study, we found a meaningful correlation age group and refusal of the COVID-19 vaccination, with many participants believing that vaccines should not be administered to older adults. This contrasts with the findings of Tetsatsi et al. (28), who noted that the older population is more vulnerable to the disease and therefore more likely to accept vaccination. This discrepancy may stem from our respondents’ belief that older individuals are naturally immune to infections. Additionally, other beliefs observed in our study included the perception that COVID-19 vaccination serves as a means for financial exploitation and the notion that individuals could discontinue all preventive measures after receiving the first dose of the vaccine. However, these beliefs are less common in other studies, making direct comparisons challenging.
Conclusion
5
This study which was aimed at unveiling the factors associated with COVID-19 vaccine refusal in Bamenda I sub-division of the Northwest Region had indicated that the COVID-19 vaccine refusal was substantially correlated with socio-demographic factors like age, gender, and educational attainment. Our findings revealed that while most participants were familiar with COVID-19, their knowledge of other diseases like Ebola and Hepatitis A was limited. Regarding attitudes toward the COVID-19 vaccination, many women engaged in discussions with health workers about the risks and benefits. Participants held several negative beliefs and myths about the vaccines.
Limitations
5.1
This study has several limitations that should be acknowledged. First, as a retrospective study relying on self-reported data, it is subject to recall bias, as participants were asked to remember their attitudes and behaviors during the height of the COVID-19 pandemic. Additionally, the use of questionnaires and self-administered surveys may have introduced social desirability bias, potentially affecting the accuracy of responses. The sample size, while adequate for preliminary analysis, may limit the generalizability of the findings to the broader population. Furthermore, the retrospective cross-sectional design does not allow for causal inferences between variables.
Future research
5.2
Future research should consider qualitative approaches, such as in-depth interviews and focus group discussions, to explore underlying beliefs, cultural influences, and emotional factors driving vaccine refusal. Longitudinal studies could also help track changes in attitudes over time and evaluate the effectiveness of targeted interventions aimed at improving vaccine acceptance in similar settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Resource, M.A.-J.H.C. Center. Available online at: https://coronavirus.jhu.edu/data/mortality [accessed 2020-05-11], (2020).
- 2Mohan B Nambiar V. COVID-19: an insight into SARS-Co V-2 pandemic originated at Wuhan City in Hubei Province of China. J Infect Dis Epidemiol. (2020) 6:146. doi: 10.23937/2474-3658/1510146, PMID: 34988352 · doi ↗
- 3Wen LS Sadeghi NB. The opioid crisis and the 2020 US election: crossroads for a national epidemic. Lancet. (2020) 396:1316–8. doi: 10.1016/S 0140-6736(20)32113-9, PMID: 33035495 PMC 7538141 · doi ↗ · pubmed ↗
- 4Filip R Gheorghita Puscaselu R Anchidin-Norocel L Dimian M Savage WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. J Personalized Med. (2022) 12:1295. doi: 10.3390/jpm 12081295, PMID: 36013244 PMC 9409667 · doi ↗ · pubmed ↗
- 5Darko DM Seaneke SK Karikari-Boateng E Nkansah E Amponsa-Achiano K Mohamed NT. Safety of m RNA COVID-19 vaccines among persons 15-years and above in Ghana: a cohort event monitoring study. Vaccine. (2024) 42:126460. doi: 10.1016/j.vaccine.2024.126460, PMID: 39447252 · doi ↗ · pubmed ↗
- 6Harris C. Transforming public health paradigms: lessons from COVID-19 to enhance global pandemic preparedness and resilience. Public health. Spectrum. (2024) 1. Available at: https://docentra.com/covid 19
- 7Possas C Marques ET Risi JB Jr Homma A. COVID-19 and future disease X in circular economy transition: redesigning pandemic preparedness to prevent a global disaster. Circ Econ Sustain. (2021) 1:1463–78. doi: 10.1007/s 43615-021-00060-x, PMID: 34888566 PMC 8238518 · doi ↗ · pubmed ↗
- 8Tran JL. Of vaccine and hesitancy. Food & Drug LJ. (2022) 77:176.