Prevalence and Risk Factors of Iron Deficiency and Iron Deficiency Anemia in Preschool Children of China: A Prospective Observational Study
Changjuan Gu, Zengcheng Wang, Huijun Zhao, Xiaotian Xie

TL;DR
This study finds that nearly a quarter of preschool children in China have iron deficiency, with feeding habits and gender being key risk factors.
Contribution
The study identifies specific independent risk factors for iron deficiency and anemia in preschool children in China.
Findings
The prevalence of iron deficiency was 25.4%, and iron deficiency anemia was 7.5% among preschool children.
Male gender, exclusive breastfeeding beyond six months, and picky eating are independent risk factors for ID and IDA.
Feeding-related factors and delayed introduction of solid foods significantly contribute to iron deficiency.
Abstract
To explore the prevalence and risk factors of iron deficiency (ID) and iron deficiency anemia (IDA) in preschool children. A total of 3503 preschool children (3–4 years) who have normal physical checkups for kindergarten admission have been studied. The prevalence of children's ID and IDA has been detected, and the main influencing factors of children's ID and IDA were analyzed by factor comparison and logistic regression. The prevalence of ID and IDA was 25.4% and 7.5%, respectively, in the total of 3503 children. Male gender, exclusive breastfeeding, delay of solid food supplement, picky eating, recent respiratory infection and diarrhea, and parents without a bachelor's degree or above or other places' household registration are associated with children's ID and IDA. Among these, male gender, exclusive breastfeeding, not adding food in time (such as > 6 months after birth), and picky…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
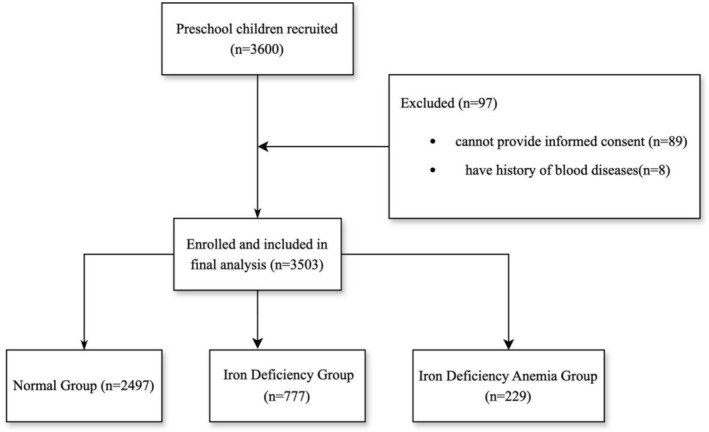 FIGURE 1
FIGURE 1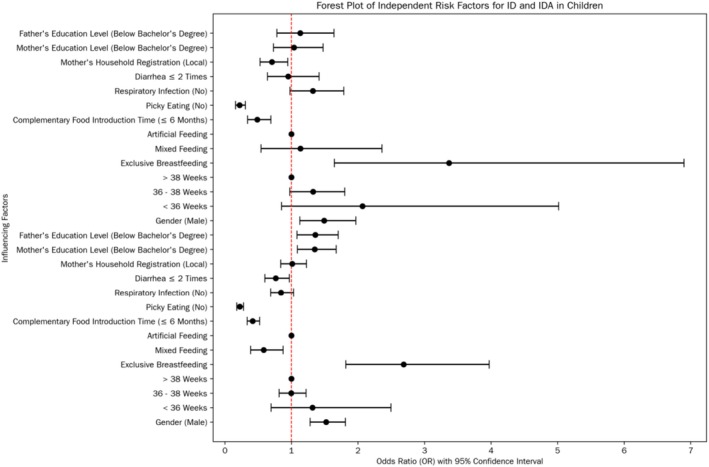 FIGURE 2
FIGURE 2| Variables | Total number (3503) | Normal group (%) | ID group (%) | X2 |
| IDA group (%) | X2 |
| |
|---|---|---|---|---|---|---|---|---|---|
| Gender | Male | 1734 | 1159 (66.8) | 445 (25.7) | 27.946 | 0.000 | 130 (7.5) | 9.02 | 0.003 |
| Female | 1769 | 1338 (75.6) | 332 (18.8) | 99 (5.6) | |||||
| Number of fetuses | Multiple fetuses | 43 | 26 (60.5) | 13 (30.2) | 2.01 | 0.156 | 4 (9.3) | 0.421 | 0.517 |
| Single fetus | 3460 | 2471 (71.4) | 764 (22.1) | 225 (6.5) | |||||
| Gestation age | Full‐term | 3346 | 2389 (71.4) | 741 (22.1) | 0.134 | 0.715 | 216 (6.5) | 0.903 | 0.342 |
| Premature | 157 | 108 (68.8) | 36 (22.9) | 13 (8.3) | |||||
| Birth weight | < 2.5 kg | 85 | 56 (65.9) | 21 (24.7) | 1.602 | 0.449 | 8 (9.4) | 1.647 | 0.439 |
| 2.5–4 kg | 3117 | 2221 (71.3) | 697 (22.4) | 199 (6.4) | |||||
| > 4.0 kg | 301 | 220 (73.1) | 59 (19.6) | 22 (7.3) | |||||
| Feeding method | Exclusive breastfeeding | 2029 | 1293 (63.7) | 580 (28.6) | 131.615 | 0.000 | 156 (7.7) | 22.538 | 0.000 |
| Artificial feeding | 211 | 161 (76.3) | 41 (19.4) | 9 (4.3) | |||||
| Mixed feeding | 1263 | 1043 (82.6) | 156 (12.4) | 64 (5.1) | |||||
| Complementary foods | ≤ 6 months | 2981 | 2202 (73.9) | 597 (20.0) | 61.568 | 0.000 | 182 (6.1) | 14.503 | 0.000 |
| > 6 months | 522 | 295 (56.5) | 180 (34.5) | 47 (9.0) | |||||
| Picky eating | Yes | 634 | 323 (50.9) | 238 (37.5) | 130.681 | 0.000 | 73 (11.5) | 60.616 | 0.000 |
| No | 2869 | 2174 (75.8) | 539 (18.8) | 156 (5.4) | |||||
| Respiratory infection* | Yes | 2583 | 1825 (70.7) | 601 (23.3) | 5.606 | 0.018 | 157 (6.1) | 2.168 | 0.141 |
| No | 920 | 672 (73.0) | 176 (19.1) | 72 (7.8) | |||||
| Respiratory infection frequency | ≤ 2 times | 2203 | 1588 (72.1) | 468 (21.2) | 2.872 | 0.090 | 147 (6.7) | 0.032 | 0.858 |
| > 2 times | 1300 | 909 (69.9) | 309 (23.8) | 82 (6.3) | |||||
| Diarrhea* | Yes | 2433 | 1716 (70.5) | 556 (22.9) | 2.242 | 0.134 | 161 (6.6) | 0.245 | 0.620 |
| No | 1070 | 781 (73.0) | 221 (20.7) | 68 (6.4) | |||||
| Diarrhea frequency | ≤ 2 times | 3013 | 2174 (72.2) | 643 (21.3) | 9.167 | 0.002 | 196 (6.5) | 0.402 | 0.526 |
| > 2 times | 490 | 323 (65.9) | 134 (27.3) | 33 (6.7) | |||||
| Caregiver person | Parents | 1969 | 1403 (71.3) | 440 (22.3) | 0.251 | 0.882 | 126 (6.4) | 0.489 | 0.783 |
| Co‐caregivers | 1534 | 1094 (71.3) | 337 (22.0) | 103 (6.7) | |||||
| Mother age | ≤ 32 years old | 1741 | 1221 (70.1) | 395 (22.7) | 0.89 | 0.345 | 125 (7.2) | 2.714 | 0.099 |
| > 32 years old | 1762 | 1276 (72.4) | 382 (21.7) | 104 (5.9) | |||||
| Mother education | Below Bachelor's Degree | 1148 | 755 (65.8) | 314 (27.4) | 27.903 | 0.000 | 79 (6.9) | 1.794 | 0.180 |
| Bachelor's Degree or Above | 2355 | 1742 (74.0) | 463 (19.7) | 150 (6.4) | |||||
| Mother household registration | Local | 2333 | 1699 (72.8) | 501 (21.5) | 3.413 | 0.065 | 133 (5.7) | 9.447 | 0.002 |
| Nonlocal | 1170 | 798 (68.2) | 276 (23.6) | 96 (8.2) | |||||
| Father age | ≤ 32 years old | 1273 | 887 (69.7) | 293 (23.0) | 1.229 | 0.268 | 93 (7.3) | 2.359 | 0.125 |
| > 32 years old | 2230 | 1610 (72.2) | 484 (21.7) | 136 (6.1) | |||||
| Father education | Below bachelor's degree | 879 | 556 (63.3) | 259 (29.5) | 38.818 | 0.000 | 64 (7.3) | 3.853 | 0.050 |
| Bachelor's degree or above | 2624 | 1941 (74.0) | 518 (19.7) | 165 (6.3) | |||||
| Father registration | Local | 2237 | 1617 (72.3) | 481 (21.5) | 2.096 | 0.148 | 139 (6.2) | 1.508 | 0.219 |
| Non‐local | 1266 | 880 (69.5) | 296 (23.4) | 90 (7.1) | |||||
| Influencing factors | B | SE | OR | 95% CI |
|
|---|---|---|---|---|---|
| Influencing factors of ID group | |||||
| Gender (male) | 0.420 | 0.089 | 1.522 | 1.279–1.811 | 0.000 |
| Gestational week | |||||
| < 36 weeks | 0.275 | 0.326 | 1.317 | 0.695–2.496 | 0.399 |
| 36–38 weeks | −0.003 | 0.103 | 0.997 | 0.815–1.220 | 0.979 |
| > 38 weeks | — | — | 1 | — | — |
| Feeding method | |||||
| Exclusive breastfeeding | 0.988 | 0.199 | 2.686 | 1.817–3.971 | 0.000 |
| Mixed feeding | −0.541 | 0.209 | 0.582 | 0.387–0.876 | 0.009 |
| Artificial feeding | — | — | 1 | — | — |
| Complementary food introduction time (≤ 6 months) | −0.874 | 0.114 | 0.417 | 0.334–0.522 | 0.000 |
| Picky eating (no) | −1.496 | 0.113 | 0.224 | 0.179–0.280 | 0.000 |
| Respiratory infection | −0.170 | 0.103 | 0.843 | 0.689–1.033 | 0.099 |
| Diarrhea | −0.271 | 0.122 | 0.763 | 0.601–0.969 | 0.026 |
| Mother's household registration (local) | 0.013 | 0.097 | 1.013 | 0.839–1.225 | 0.890 |
| Mother's education level (below bachelor's degree) | 0.301 | 0.109 | 1.351 | 1.090–1.674 | 0.006 |
| Father's education level (below bachelor's degree) | 0.307 | 0.115 | 1.359 | 1.085–1.704 | 0.008 |
| Influencing factors of IDA group | |||||
| Gender (male) | 0.398 | 0.142 | 1.49 | 1.127–1.969 | 0.005 |
| Gestational week | |||||
| < 36 weeks | 0.726 | 0.453 | 2.067 | 0.851–5.018 | 0.109 |
| 36–38 weeks | 0.282 | 0.156 | 1.326 | 0.976–1.801 | 0.071 |
| > 38 weeks | — | — | 1 | — | — |
| Feeding method | |||||
| Exclusive breastfeeding | 1.215 | 0.366 | 3.369 | 1.645–6.901 | 0.001 |
| Mixed feeding | 0.127 | 0.374 | 1.135 | 0.545–2.362 | 0.735 |
| Artificial feeding | — | — | 1 | — | — |
| Complementary food introduction time (≤ 6 months) | −0.720 | 0.180 | 0.487 | 0.342–0.692 | 0.000 |
| Picky eating (no) | −1.506 | 0.168 | 0.222 | 0.160–0.308 | 0.000 |
| Respiratory infection (no) | 0.280 | 0.154 | 1.323 | 0.979–1.788 | 0.069 |
| Diarrhea ≤ 2 times | −0.050 | 0.203 | 0.952 | 0.639–1.417 | 0.807 |
| Mother's household registration (local) | −0.347 | 0.149 | 0.707 | 0.528–0.946 | 0.020 |
| Mother's education level (below bachelor's degree) | 0.038 | 0.179 | 1.039 | 0.732–1.475 | 0.832 |
| Father's education level (below bachelor's degree) | 0.123 | 0.189 | 1.131 | 0.781–1.639 | 0.514 |
- —Science and Technology Program of Suzhou10.13039/501100018556
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Child Nutrition and Water Access · Folate and B Vitamins Research
Introduction
1
Iron deficiency anemia (IDA) and iron deficiency (ID) are among the most prevalent nutritional deficiency disorders in children worldwide (Leung et al. 2024). IDA, in particular, is characterized by a reduction in hemoglobin levels due to insufficient iron availability, while ID represents an earlier stage where iron stores are depleted, yet anemia may not be fully manifested (Camaschella 2019). These conditions are not only common but also pose significant threats to children's health.
Recent research (Pivina et al. 2019) has also highlighted the critical impact of ID during the early stages of life, especially in infants. The brain is in a rapid development phase during infancy, and iron is essential for normal brain development. ID during this period may lead to irreversible damage to brain development, potentially affecting cognitive function, learning ability, and behavior in the long term.
Over the past few decades, there has been an increase in the understanding of anemia and the implementation of intervention measures for this condition. In China, due to its vast territory and diverse regional characteristics, even the Chinese government has made reducing children's IDA a key goal; nevertheless, the incidence of children's IDA in various regions remains at a relatively high level (Cheung et al. 2023; Zheng et al. 2020). In particular, in economic development zones with large‐scale population inflows, a high proportion of child‐bearing‐age populations, and significant differences in the educational levels of parents, relevant epidemiological studies are urgently needed. Moreover, before the effective implementation of national intervention measures and programs, it is essential to assess the prevalence and severity of ID and IDA and their potential risk factors.
Therefore, this study is to explore the prevalence and risk factors of ID and IDA in preschool children and provide a scientific basis for effective prevention and targeted treatment, aiming at improving the overall health level of children.
Materials and Methods
2
Study Design
2.1
The data for this study were collected from preschool–age children undergoing kindergarten admission physical examinations in May 2023. This research project was a collaborative effort between the education and health departments of Suzhou Industrial Park and the Municipal Science and Technology Bureau. It was led by the Department of Pediatrics of Tongji Hospital of Tongji University and Suzhou Kowloon Hospital of Shanghai Jiaotong University, with the assistance of relevant kindergartens and nurseries. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Diagnostic Criteria
2.2
Diagnostic Criteria for IDA
2.2.1
The diagnostic criteria for IDA were based on the following:
- Hemoglobin (HB) reduction and meet the anemia diagnostic criteria for children.
- Microcytic hypochromic characteristics: Mean corpuscular volume (MCV) < 80 fL, mean corpuscular hemoglobin (MCH) < 27 pg, and mean corpuscular hemoglobin concentration (MCHC) < 310 g/L.
- Related factors that could lead to ID.
- In the iron metabolism test, at least two of the following four items were present: Serum ferritin (SF) < 15 μg/L, serum iron (SI) < 10.7 μmol/L, total iron‐binding capacity (TIBC) > 62.7 μmol/L, and transferrin saturation (TS) < 15%.
- Effective response to iron therapy: After 4 weeks of iron therapy, Hb increased by more than 20 g/L.
- Bone marrow examination: The extracellular iron was significantly reduced, and the sideroblasts < 15%.
- Differential diagnosis: Excluding other diseases that could present with microcytic hypochromic anemia.
Those who met the first and second items above and excluded other diseases with microcytic hypochromic anemia could be tentatively diagnosed with IDA.
Diagnostic Criteria for ID
2.2.2
The diagnostic criteria for ID were as follows:
- Factors that could lead to ID
- SF was below the normal range
- Microcytic hypochromic characteristics
- Hb had not yet reached the degree of anemia.
Patients
2.3
Inclusion Criteria
2.3.1
- Preschool children aged between 3 and 4 years old.
- Permission from parents: The parents and children were willing to cooperate with the examination, complete the questionnaire survey, and sign the informed consent.
Exclusion Criteria
2.3.2
- History of blood diseases, congenital malformations, or family history of genetic diseases.
- The physical examination showed special facial features, jaundice, splenomegaly, or other physical signs related to blood diseases.
- There was a history of diseases or recent surgeries during the detection period.
Detection Items
2.4
Physical Examination
2.4.1
The physical examination for preschool children included routine items for kindergarten admission. This involved a comprehensive assessment of physical development, such as measuring height, weight, and head circumference to evaluate the growth status of children. Behavioral ability was also examined, observing the children's motor skills, language development, and social interaction abilities. Clinical physical examinations of the skin and mucosa were carried out to check for any signs of skin diseases, jaundice, or other abnormal conditions. The head, face, five sense organs, as well as the thoracic and abdominal internal organs, were carefully examined. For example, auscultation of the heart and lungs was performed to detect any abnormal heart sounds or respiratory problems, and palpation of the abdomen was done to check for the presence of an enlarged liver, spleen, or other abdominal masses.
Laboratory Tests
2.4.2
- Blood Routine Test: The dodecyl sulfonate method was used (standard instrument: SYSMEX SN‐A3430). This test detected routine items such as the counts of red blood cells (RBC), white blood cells (WBC), and platelets in the peripheral blood, HB value, and RBC morphological parameters (MCV, MCH, and MCHC).
- SF: The chemiluminescent microparticle immunoassay was adopted (standard instrument: ARCHITECT i2000SR). SF is an important indicator reflecting the body's iron storage status. By measuring SF levels, it is possible to determine whether a child has ID at an early stage.
- SI: The ferrozine method was employed (standard instrument: ARCHITECT c16000 system). Measuring SI can help understand the level of iron in the blood that is available for physiological functions, which is crucial for diagnosing iron‐related disorders.
Questionnaire Survey
2.4.3
A questionnaire survey was designed and completed with the close cooperation of kindergartens and nurseries based on the epidemiological characteristics and possible influencing factors of children's IDA suggested by previous studies.
- Birth History: Information such as gestational age (full‐term or premature), number of fetuses (single fetus or multiple fetuses), birth weight, and average gestational age was collected.
- Feeding History: The feeding methods within 6 months after birth were investigated, including exclusive breastfeeding, mixed feeding with added formula milk or relying solely on formula milk, and artificial feeding. The time of complementary food addition was also recorded. Additionally, with the assistance of kindergartens and nurseries, it was determined whether there were obvious picky eating habits.
- Common Disease History: Information on whether there was a clear history of respiratory tract infections or diarrhea within the recent 6 months, and the number of illnesses was collected.
- Primary Caregiver Information: This included details about the composition of the main primary caregiver in the family (whether grandparents were involved), the ages, educational levels, and household registration locations of the parents.
Based on the test results, the children under examination were divided into a normal group, an ID group, and an IDA group. The data from the questionnaire were then used to statistically compare and analyze the main influencing factors leading to the occurrence of ID and IDA in local children.
Statistical Analysis
2.5
Data analysis was performed using SPSS 20.0 statistical software. For count data, they were expressed as frequency (n) and rate (%). The chi‐square test was used for comparisons between groups. For measurement data, they were expressed as mean ± standard deviation (^−^x ± s), and the t‐test was used for comparisons between groups. Logistic regression analysis was employed to identify independent risk factors. A value of p < 0.05 was considered statistically significant.
Results
3
A total of 3600 children, aged between 3 and 4 years old, from 23 kindergartens (7 public and 16 private) were assessed for eligibility for the study. 97 children were excluded because they could not provide informed consent or had a history of blood diseases. Finally, 3503 children were enrolled in the study (Figure 1). Among them, 1734 were boys and 1769 were girls (Table 1).
The study flow diagram.
According to the diagnostic criteria, 777 cases (25.4%) of ID and 229 cases (7.5%) of IDA were detected, respectively. Statistical comparison showed that the prevalence rates of ID and IDA in boys were significantly higher than those in girls. The specific data are shown in Table 1.
The univariate analysis showed factors such as gestational age, number of fetuses, and birth weight had no significant differences between the normal group and ID/IDA group. The prevalence of ID and IDA in children, who were exclusively breastfed, did not add complementary foods in time, or had obvious picky eating habits, was significantly increased. For children with a history of respiratory tract infections or diarrhea within the recent 6 months, the prevalence of ID was notably elevated. Those whose fathers or mothers did not obtain higher education diplomas and whose mothers had non‐local household registrations demonstrated a high incidence of both ID and IDA. In contrast, neither the participation of grandparents in the upbringing process nor the parental age exhibited any correlation with the prevalence of ID and IDA. The specific data are shown in Table 1.
Based on the results of the univariate analysis, Logistic regression analysis was carried out. The results showed that male gender, exclusive breastfeeding, not adding complementary foods in time (more than 6 months after birth), and having a picky eating habit were all independent risk factors for the incidence of ID and IDA in preschool children.
In addition, there were some differences in independent risk factors between ID and IDA. A recent history of diarrhea, the educational levels of parents were independent risk factors for the incidence of ID, while household registration was an independent risk factor for the incidence of IDA. Premature birth and a recent history of respiratory tract infections were not independent risk factors for ID and IDA. The specific data are shown in Table 2 and Figure 2.
Forest plot of independent risk factors for ID and IDA in children.
Discussion
4
ID and IDA are significant global health issues, particularly affecting children and pregnant women (Camaschella 2019). The prevalence is high in regions with low Socio‐Demographic Indexes, such as sub‐Saharan Africa and South Asia (Camaschella 2019; Liu et al. 2024). The samples of this study were from Suzhou Industrial Park in China, which is a national‐level economic development zone established under an international cooperation model. The results showed that the incidence of IDA and ID in this group of children still reached 25.4% and 7.5%, respectively. This indicates that even in the relatively developed areas in terms of economic and cultural levels, the overall popularization degree of knowledge related to children's iron metabolism is still lagging behind.
ID is a precursor to IDA and is more prevalent than IDA, especially in children (Turawa et al. 2021; Gupta et al. 2016). ID in young children, even without anemia, can lead to significant neurocognitive and developmental challenges, including cognitive impairments, psychomotor delays, and behavioral issues [3.9]. Our research findings indicate that the prevalence rate of ID exceeds that of IDA by almost threefold. Paradoxically, clinicians tend to allocate less attention to ID. In the case of young children, whose brains are at a critical stage of development, the detrimental effects induced by ID frequently prove to be persistent and, consequently, demand heightened attention from all concerned parties.
Among adults, females are more likely to develop IDA due to factors such as menstrual blood loss, pregnancy, and dietary deficiencies (Sedlander et al. 2021; Levi 2019). Nevertheless, when it comes to the pediatric population, the gender‐based variation in the prevalence of IDA remains inconclusive. One study in Sweden and Honduras found that male infants had significantly lower HB levels and other iron status indicators compared to females, with boys having a 10‐fold higher risk of developing IDA by 9 months of age (Domellöf et al. 2002). Conversely, other research indicates a higher prevalence of IDA among females, particularly in adolescents, with rates reported as 26% in the Gaza Strip, Palestine (Jalambo et al. 2018), 21.1% in Jatinangor, Indonesia (Sari et al. 2022), and 40% in India (Scott et al. 2022).
In our study, male gender was identified as a clear risk factor for ID and IDA in 3–4 years old preschool children. It might be due to rapid weight gain, larger blood volume, and potentially higher androgen levels, which may influence iron metabolism and requirements. Some studies suggest that boys may be more susceptible to the cognitive impacts of ID (Farhan et al. 2024). The higher incidence of cognitive impairment in boys may be associated with a higher risk of early ID. Our results reflected the importance of early detection and intervention, and further research is needed to fully understand the gender‐specific impacts and to develop effective prevention strategies.
Exclusive breastfeeding is generally recommended for the first 6 months of life due to its numerous health benefits. However, our findings and several previous studies indicate that exclusive breastfeeding beyond 6 months can increase the risk of ID and IDA in infants. This is because breast milk alone may not provide sufficient iron to meet the growing needs of infants after this period (Clark et al. 2017).
Our study demonstrates that a history of poor feeding during infancy (failure to add complementary foods after 6 months) is an independent risk factor for the incidence of ID and IDA in preschool children, which further demonstrates the importance of timely addition of complementary foods. While exclusive breastfeeding is beneficial in the early months, it may increase the risk of ID and anemia if continued beyond 6 months without appropriate dietary interventions.
For preschoolers aged between 3 and 4, another prominent feeding concern pertains to picky eating habits and dietary aversions. Picky eating often results in a limited diet, which can lead to low intakes of iron and zinc, particularly due to reduced consumption of meat, fruits, and vegetables (Taylor and Emmett 2018). Our research reaffirms that children with finicky eating behaviors are more predisposed to developing ID and IDA. Ensuring a balanced diet rich in iron and other essential nutrients is crucial for preventing ID and anemia in children.
Diarrhea can lead to nutrient malabsorption, including iron, particularly in young children (Chandyo et al. 2015). Our research findings suggest that persistent diarrhea (> 2 times in recently 6 months) is a risk factor for ID, but not for IDA. It is shown that while diarrhea can increase the risk of ID, the association with IDA is not significant, suggesting other factors might be involved in the development of anemia. The relationship between diarrhea and IDA is complex, might involve multiple nutritional and environmental factors, which need further exploration.
Similar to previous studies (Al‐Suhiemat et al. 2020), our research found that parental education plays a significant role in influencing the risk of ID and IDA in children. Children with more educated parents are less likely to develop ID and anemia due to higher socioeconomic status and better dietary practices, including a greater understanding of the importance of iron‐rich foods and the role of dietary diversity, which contribute to higher HB levels in children.
Thus, conducting educational programs for parents is of the utmost necessity. These programs can effectively enhance their knowledge about IDA, thereby reducing the prevalence of this condition among children.
Premature birth, being a twin, and low birth weight are recognized as risk factors for ID and IDA in many previous studies (Sundararajan and Rabe 2021; Wirth et al. 2022). However, our research findings present distinctive outcomes; these all are not risk factors for ID or IDA in children after 3 years old. Under unfavorable congenital conditions like premature birth, provided that adequate attention of iron‐supplemented diet promptly, it may not have an impact during early childhood.
Our study has several limitations. For example, there is a limited number of cases and a relatively narrow age distribution. However, the sample selection from China can offer valuable references for similar regions with high development levels and large inflow populations.
Conclusion
5
Our study highlights the substantial prevalence of ID (25.4%) and IDA (7.5%) among preschool children in China. Among 3–4 years preschool children, boys are at higher risk of developing ID and IDA. Exclusive breastfeeding beyond 6 months without timely introduction of complementary foods, picky eating habits, and lower parental education levels are independent risk factors. These findings provide actionable insights for targeted interventions.
Author Contributions
Changjuan Gu: conceptualization (equal), data curation (equal), formal analysis (lead), investigation (equal), methodology (equal), resources (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal). Zengcheng Wang: conceptualization (equal), data curation (equal), formal analysis (equal), funding acquisition (lead), investigation (equal), project administration (lead), validation (equal), writing – original draft (equal). Huijun Zhao: conceptualization (equal), data curation (equal), methodology (equal), project administration (supporting), supervision (equal), writing – review and editing (equal). Xiaotian Xie: conceptualization (equal), investigation (supporting), methodology (lead), project administration (supporting), supervision (equal), writing – review and editing (equal).
Ethics Statement
This study was in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Suzhou Kowloon Hospital (XJ‐2016‐007).
Consent
All the parents of children signed the informed consent forms.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al‐Suhiemat, A. A. , R. M. Shudifat , and H. Obeidat . 2020. “Maternal Level of Education and Nutritional Practices Regarding Iron Deficiency Anemia Among Preschoolers in Jordan.” Journal of Pediatric Nursing 55: e 313–e 319.32933806 10.1016/j.pedn.2020.08.019 · doi ↗ · pubmed ↗
- 2Camaschella, C. 2019. “Iron Deficiency.” Blood 133: 30–39.30401704 10.1182/blood-2018-05-815944 · doi ↗ · pubmed ↗
- 3Chandyo, R. , M. Ulak , R. Adhikari , H. Sommerfelt , and T. Strand . 2015. “Prevalence of Iron Deficiency and Anemia Among Young Children With Acute Diarrhea in Bhaktapur, Nepal.” Healthcare (Basel) 3: 593–606.27417782 10.3390/healthcare 3030593 PMC 4939584 · doi ↗ · pubmed ↗
- 4Cheung, Y. T. , D. F. Y. Chan , C. K. Lee , et al. 2023. “Iron Deficiency Among School‐Aged Adolescents in Hong Kong: Prevalence, Predictors, and Effects on Health‐Related Quality of Life.” International Journal of Environmental Research and Public Health 20: 2578.36767942 10.3390/ijerph 20032578 PMC 9916133 · doi ↗ · pubmed ↗
- 5Clark, K. M. , M. Li , B. Zhu , et al. 2017. “Breastfeeding, Mixed, or Formula Feeding at 9 Months of Age and the Prevalence of Iron Deficiency and Iron Deficiency Anemia in Two Cohorts of Infants in China.” Journal of Pediatrics 181: 56–61.27836288 10.1016/j.jpeds.2016.10.041PMC 5274569 · doi ↗ · pubmed ↗
- 6Domellöf, M. , B. Lönnerdal , K. G. Dewey , et al. 2002. “Sex Differences in Iron Status During Infancy.” Pediatrics 110: 545–552.12205258 10.1542/peds.110.3.545 · doi ↗ · pubmed ↗
- 7Farhan, H. A. , F. A. A. Al‐Ghannam , K. Wani , et al. 2024. “Associations Between Serum Iron Indices and Self‐Assessed Multiple Intelligence Scores Among Adolescents in Riyadh, Saudi Arabia.” Biomedicine 12: 1578.10.3390/biomedicines 12071578 PMC 1127469439062151 · doi ↗ · pubmed ↗
- 8Gupta, P. M. , C. G. Perrine , Z. Mei , and K. S. Scanlon . 2016. “Iron, Anemia, and Iron Deficiency Anemia Among Young Children in the United States.” Nutrients 8: 330.27249004 10.3390/nu 8060330 PMC 4924171 · doi ↗ · pubmed ↗