Cryptococcus albidus (Naganishia albida) meningitis in a young patient with T-cell acute lymphoblastic leukaemia
Amber Prasad, Minakshi Singh, Priyal Anand

TL;DR
A young leukemia patient was diagnosed with rare fungal meningitis caused by Cryptococcus albidus, highlighting the need for accurate diagnosis and antifungal treatment.
Contribution
This case report highlights the diagnostic challenge and treatment of Cryptococcus albidus meningitis in immunocompromised patients.
Findings
Cryptococcus albidus meningitis was misdiagnosed as HSV encephalitis before confirmation via CSF analysis.
Antifungal therapy with liposomal amphotericin B and flucytosine improved the patient's condition.
Elevated procalcitonin levels may indicate fungal infections in immunocompromised individuals.
Abstract
Cryptococcus albidus, an emerging pathogen, poses diagnostic and therapeutic challenges, especially in immunocompromised patients. We report a case of C. albidus meningitis in a young T-cell acute lymphoblastic leukaemia patient, initially suspected to have Herpes Simplex Virus (HSV) encephalitis. CSF analysis confirmed C. albidus, leading to antifungal therapy with liposomal amphotericin B and flucytosine, resulting in clinical improvement. Elevated procalcitonin levels suggest a potential role in fungal infections. This case underscores the importance of early identification and appropriate treatment in C. albidus meningitis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
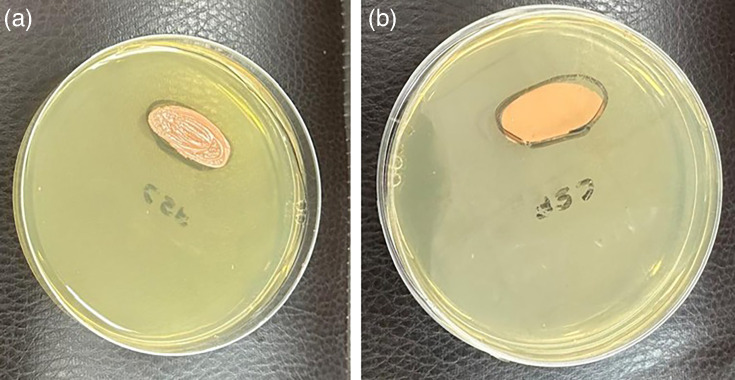 Fig. 1
Fig. 1 Fig. 2
Fig. 2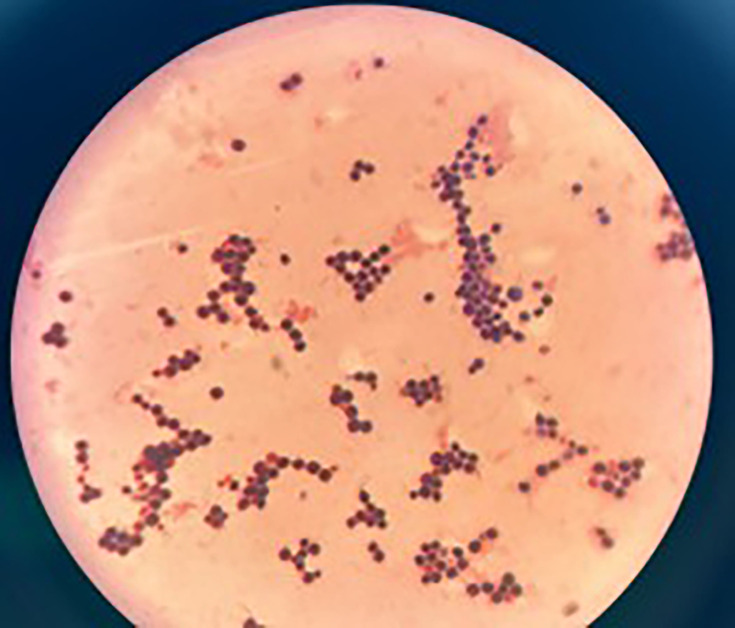 Fig. 3
Fig. 3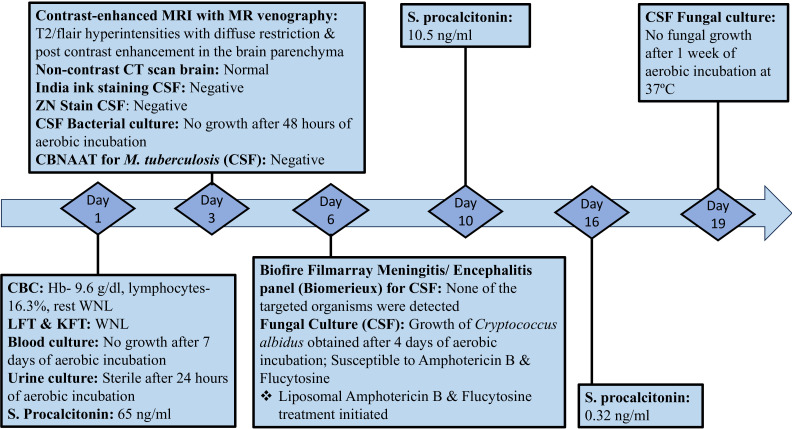 Fig. 4
Fig. 4| Parameter | Day 1 (Initial) | Day 13 (Repeat LP) | Reference range |
|---|---|---|---|
| Opening pressure (cm H2O) | 23 | 18 | 10–20 |
| Appearance | Slightly turbid | Clear | Clear |
| Cell count (cells μl−1) | 180 | 25 | <5 |
| Lymphocytes (%) | 85 | 90 | >80 |
| Neutrophils (%) | 15 | 10 | <1 |
| Protein (mg dl−1) | 95 | 60 | 15–45 |
| Glucose (mg dl−1) | 35 | 50 | 50–75 |
| CSF:serum glucose ratio | 0.42 | 0.65 | >0.6 |
| India ink stain | Negative | Negative | – |
| Cryptococcal antigen* | Negative* | Negative* | – |
| Gram stain | No organisms/pus cells | No organisms/pus cells | – |
| Bacterial culture (48 h) | No growth | No growth | – |
| Fungal culture (SDA) | No growth on days 1–3 | – | |
| Biofire ME panel | Negative | Not repeated | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Antifungal resistance and susceptibility · Cytomegalovirus and herpesvirus research
Data Summary
No data were generated during this research, nor are they required for the work to be reproduced.
Introduction
Cryptococcus species are yeasts belonging to the basidiomycetous fungi, recognized as causative agents for various diseases. Among these, Cryptococcus neoformans and Cryptococcus gattii are widely acknowledged as the most prevalent pathogenic species [13]. Nonetheless, there has been a recent upsurge in infections attributed to non-neoformans cryptococcal species like Papiliotrema laurentii (previously known as Cryptococcus laurentii) and Naganishia albida (synonym Cryptococcus albidus) [46]. The primary sources of C. albidus are considered to be environmental, particularly residues found in the canopies of specific trees [7]. C. albidus is an uncommon cause of fungal meningitis, especially in immunocompromised patients, such as those with haematological malignancies. T-cell acute lymphoblastic leukaemia (T-ALL) is associated with immunosuppression, predisposing patients to opportunistic infections [8]. This case highlights the importance of considering rare pathogens in the differential diagnosis of meningitis, particularly in high-risk populations.
Case presentation
A 16-year-old male with a history of T-ALL presented with a 4-day history of headache, followed by 3 days of fever, vomiting and decreased appetite. The fever ranged from 100 to 102 °F, relieved by antipyretics, and vomiting was non-bilious, non-bloody, with food particles and relieved by antiemetics. The headache was frontal, moderate to severe and not fully relieved by medication. He also had three to four episodes of loose stools 2 days prior but no abdominal pain, cough, rash, bleeding or haematuria.
On examination, he was oriented, with normal tone and power in both upper and lower limbs. Initial tests included complete blood count, liver function test, kidney function test, procalcitonin and blood and urine cultures. Persistent symptoms led to an Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) Scan of the brain. The contrast-enhanced MRI with MR venography revealed T2/Flair hyperintensities with diffuse restriction and post-contrast enhancement in the brain parenchyma, suggesting the likelihood of HSV encephalitis, though the CT scan showed no significant abnormalities, given its lower sensitivity for Cerebrospinal Fluid (CNS) infections. Cerebrospinal Fluid (CSF) analysis included microscopy, India ink staining, bacterial and fungal cultures, ZN stain and cartridge-based nucleic-acid amplification test (Cepheid GeneXpert) for tuberculosis. The patient was started on acyclovir for suspected HSV encephalitis and showed initial improvement, though the headache persisted.
Subsequently, a Biofire Filmarray Meningitis/Encephalitis panel (ME panel; Biomerieux) was done for CSF, targeting six bacteria, seven viruses and one yeast (C. neoformans). However, the results indicated the absence of pathogens included in the panel, including HSV 1 and HSV 2. Bacterial culture of CSF revealed no growth after 48 h of aerobic incubation at 37 °C. Fungal culture revealed pale pink-coloured, smooth and mucoid colonies on Sabouraud dextrose agar (SDA) after 4 days of aerobic incubation at 37 and 25 °C (Figs13), subsequently identified as C. albidus by VITEK 2 (BioMérieux) using a YST ID card. Antifungal susceptibility testing using the VITEK 2 system (YS08 card), which employs the broth microdilution principle according to Clinical and Laboratory Standards Institute (CLSI) standards for Antimicrobial Susceptibility Testing (AST), confirmed susceptibility to amphotericin B (MIC ≤1 µg ml^−1^) and flucytosine (MIC ≤1 µg ml^−1^). Ophthalmology referral was done in view of ophthalmic complications, but the examination revealed no positive findings. Procalcitonin decreased from 65 to 10.5 ng ml^−1^ after 4 days of treatment, with further normalization to 0.32 ng ml^−1^ on day 10. The patient showed clinical improvement, with resolution of vomiting and headache, though long-term follow-up is needed to monitor for relapse or complications.
Growth on SDA plate after 4 days of aerobic incubation at 37 °C (Reverse and obverse).
Light pink-coloured smooth, mucoid colonies on SDA tubes at 25 °C (reverse and obverse).
Gram stain from growth on SDA showing rounded yeast cells (100X).
Diagnostic assessments
Standard protocols for CSF processing were followed according to CLSI guidelines. All CSF samples were processed within 2 h of collection to ensure optimal recovery of pathogens and accurate cell counts. Blood and CSF samples were collected before initiation of any antimicrobial therapy.
CSF opening pressure was 23 cm H2O initially (slightly elevated), which normalized to 18 cm H2O on repeat lumbar puncture performed on day 13 of antifungal therapy (Table 1).
Microbiological assessment of CSF: the CSF specimen was centrifuged at 1,000 g for 5–10 min, and the supernatant was used for cryptococcal antigen testing. For direct microscopy, one drop of the sediment was placed to prepare an India ink mount. The remaining sediment was transferred into a tube containing the remaining CSF and mixed. Several drops of the sediment were transferred to a slide to make a thick smear. The smear was air-dried, heat-fixed and then Gram staining was performed. No pus cells and no micro-organisms were seen in the direct Gram stain of the CSF deposit, likely due to the lower sensitivity of Gram stain compared to culture. The smear was examined microscopically using the 40X and 100X objectives. A KOH mount was prepared using the resuspended sediment sample and observed under 10X and 40X objectives.
For bacterial culture, the resuspended sediment was inoculated onto blood agar, MacConkey agar and chocolate agar using the streak culture method. Sample was also inoculated in Brain Heart Infusion (BHI) broth and incubated aerobically at 37 °C. The chocolate agar plates were incubated in a candle jar at 37 °C, while the blood agar plates were incubated aerobically at 37 °C.
Candida spp. and C. neoformans are the most common causes of fungal (yeast) meningitis. These were initially ruled out, as no growth was observed on blood agar and chocolate agar, where they typically grow. Further confirmation was obtained through the Biofire ME panel, which specifically targets C. neoformans and is considered a gold standard for rapid pathogen detection. However, this panel does not include C. albidus, explaining why initial screening was negative despite the presence of this rare cryptococcal species.
For fungal culture, the resuspended sediment was inoculated onto SDA plates and tubes using both central inoculation on plates and the streak method in tubes, with duplicate cultures incubated at 25 and 37 °C. The central inoculation on plates allowed observation of overall colony morphology and pigmentation, while the streak inoculation in tubes (as shown in Fig. 2) provided well-isolated single colonies necessary for accurate yeast identification.
Although the Biofire ME panel has limitations, including potential false negatives and lower sensitivity compared to traditional methods for some pathogens, it represents the best available rapid diagnostic tool in our resource-limited setting. While we recognize that bacterial culture is not a definitive gold standard and cannot entirely exclude all bacterial infections, we ruled out the common causes of bacterial meningitis through comprehensive culture methods and the Biofire ME panel, which includes the more common bacterial pathogens (Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae and Streptococcus pneumoniae).
The diagnostic assessments are shown in Fig. 4.
Diagnostic timeline. Day refers to day of admission and day of investigation sent to laboratory. CBC, complete blood count; LFT, liver function test; KFT, kidney function test; CBNAAT, cartridge-based nucleic-acid amplification test.
Differential diagnoses
Viral meningitis was ruled out by the Biofire Filmarray ME panel (Biomerieux).C. neoformans was ruled out by the Biofire Filmarray ME panel (Biomerieux).Bacterial meningitis was ruled out, as there was no bacterial growth on blood agar and chocolate agar after 48 h of aerobic incubation at 37 °C.
Therapeutic interventions
Following identification of C. albidus, treatment was initiated with induction therapy consisting of intravenous liposomal amphotericin B and flucytosine for 15 days. The patient received a 50 mg injection of liposomal amphotericin B diluted in 250 ml of NS over 4 h daily, supplemented with 10 mmol of potassium chloride and 4 mmol of magnesium sulphate. Additionally, tablet flucytosine was initiated, to be taken four times daily in divided doses, amounting to a total of 5,250 mg per day. This was continued for 14 days.
Follow-up and outcome
The patient had significant symptomatic improvement – as the complaints of headache and vomiting subsided and intracranial pressure was normalized. After completion of induction therapy and negative CSF fungal culture, consolidation therapy was started with fluconazole, 800 mg PO daily. The patient was advised for follow-up and for regular monitoring of liver enzymes at least weekly.
Discussion
This case underscores the challenges in diagnosing and managing C. albidus meningitis, particularly in immunocompromised patients. Prompt identification and appropriate antifungal therapy are essential for favourable outcomes. The immune response plays a critical role in Cryptococcus infection pathogenesis, as highlighted by studies on C. neoformans. Adult meningitis studies in high-prevalence settings provide valuable insights into the clinical spectrum and outcomes of cryptococcal disease. This case report contributes to the existing literature by highlighting C. albidus as an emerging pathogen in meningitis cases, especially among immunocompromised individuals. While procalcitonin is commonly utilized as an indicator of bacterial infection, our case presented a notable deviation from this norm. Specifically, we observed a significant elevation in procalcitonin levels associated with fungal meningitis. Remarkably, these levels exhibited a marked decrease following the initiation of antifungal therapy. Elevated procalcitonin levels have been observed in patients with invasive fungal infections, particularly those caused by Candida species [9]. However, the significance of procalcitonin levels in cryptococcal infections remains largely unexplored.
Cunha and Lusins reported a case of C. albidus meningitis in an adult male patient in 1973. CSF India ink was positive, and culture revealed growth of C. albidus. The patient was started on liposomal amphotericin B and symptomatically improved after 1 week of treatment [10]. A case of cryptococcal albidus meningitis in an immunocompromised adult male patient who was already receiving corticosteroids was reported by J.C. Melo et al. from the USA in 1980 [11]. CSF was negative for India ink and the cryptococcal antigen test. Treatment with amphotericin B was started, but unfortunately, the patient had cardiorespiratory arrest on the 89th day of his hospital stay and could not be resuscitated [11]. Aljehani et al. reported a case of C. albidus fungaemia and meningitis in September 2023 in a preterm infant, linked to premature birth, prolonged antibiotics and invasive medical procedures. CSF was negative for India ink and the cryptococcal antigen test. Although HIV-negative, the infant’s condition was exacerbated by intravenous lines and total parenteral nutrition. Treatment with liposomal amphotericin B, excluding flucytosine, proved effective [12].
This case highlights the emerging role of C. albidus as a pathogen in immunocompromised patients, particularly those with T-ALL. The patient’s clinical improvement following antifungal therapy with liposomal amphotericin B and flucytosine underscores the importance of early diagnosis and appropriate treatment. Additionally, elevated procalcitonin levels, typically associated with bacterial infections, suggest a potential role for procalcitonin as a biomarker in fungal infections. This case emphasizes the need for heightened awareness of rare pathogens in meningitis diagnosis and management, particularly in immunosuppressed individuals, and calls for further research to explore the epidemiology, virulence and optimal treatment strategies for C. albidus infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Faress JA Hejal R Pulmonary crytpococcosis due to C albidus in a patient on Infliximab Chest 2004126987 S 10.1378/chest.126.4_Meeting Abstracts.987S · doi ↗
- 2de Castro LEF Sarraf OA Lally JM Sandoval HP Solomon KD et al Cryptococcus albidus keratitis after corneal transplantation Cornea 20052488288310.1097/01.ico.0000157404.34774.1a 16160511 · doi ↗ · pubmed ↗
- 3Hagen F Lumbsch HT Arsic Arsenijevic V Badali H Bertout S et al Importance of resolving fungal nomenclature: the case of multiple pathogenic species in the Cryptococcus genusm Sphere 20172 e 00238-1710.1128/m Sphere.00238-1728875175 PMC 5577652 · doi ↗ · pubmed ↗
- 4Burnik C Altintas ND Ozkaya G Serter T Selçuk ZT et al Acute respiratory distress syndrome due to Cryptococcus albidus pneumonia: case report and review of the literature Med Mycol 20074546947310.1080/1369378070138601517654275 · doi ↗ · pubmed ↗
- 5Khawcharoenporn T Apisarnthanarak A Mundy LM Non-neoformans cryptococcal infections: a systematic review Infection 200735515810.1007/s 15010-007-6142-817401707 PMC 7101977 · doi ↗ · pubmed ↗
- 6Liu X-Z Wang Q-M Göker M Groenewald M Kachalkin AV et al Towards an integrated phylogenetic classification of the tremellomycetes Stud Mycol 2015818514710.1016/j.simyco.2015.12.00126955199 PMC 4777781 · doi ↗ · pubmed ↗
- 7Kamari A Sepahvand A Mohammadi R Isolation and molecular characterization of Cryptococcus species isolated from pigeon nests and eucalyptus trees J Mycol Med 20173202510.29252/cmm.3.2.20PMC 576389429354777 · doi ↗ · pubmed ↗
- 8Fishman JA Opportunistic infections--coming to the limits of immunosuppression?Cold Spring Harb Perspect Med 20133 a 01566910.1101/cshperspect.a 01566924086067 PMC 3784816 · doi ↗ · pubmed ↗