Analysis of the Relationship Between EGFR Mutations and PD-L1, ALK, and ROS1 Alterations in Patients with Non-Small-Cell Lung Cancer: The Most Extensive Study Conducted in Iran
Sepideh Hadimaleki, Roham Sarmadian, Abolfazl Gilani, Parisa Mehrasa, Ali Esfahani, Mortaza Raeisi, Yousef Roosta, Amir Vahedi

TL;DR
This study from Iran found that EGFR mutations are common in lung cancer patients and are not linked to ALK or PD-L1 changes, highlighting the importance of EGFR testing for treatment decisions.
Contribution
The study provides the most extensive analysis of EGFR, ALK, ROS1, and PD-L1 alterations in NSCLC patients from Iran.
Findings
EGFR mutations were found in 26.4% of NSCLC cases, with a higher frequency in females.
Exon 19 deletion was the most common EGFR mutation, and no significant association was found with ALK or PD-L1.
ROS1 mutations were not detected in the studied population.
Abstract
Objective: Lung cancer, the second most common type of cancer, is the leading cause of cancer-related mortality, with non-small-cell lung carcinoma (NSCLC) being the most prevalent subtype. The presence of EGFR mutations in NSCLC influences tumor behavior and treatment response. The prevalence of EGFR mutation in Iranian patients is limited. This study investigated the frequency of EGFR mutation and its association with PD-L1, ALK, and ROS1 expression in patients with NSCLC from Northwest Iran. Material and Methods: A retrospective analysis was conducted on 647 cases of NSCLC from April 2018 to August 2024 at Imam Reza Hospital in Tabriz, Iran. Histologic diagnoses were confirmed, and patient data were collected. EGFR mutation testing targeted exons 18-21 using Sanger sequencing and Real-Time PCR. ALK and ROS1 rearrangements were assessed using fluorescence in situ hybridization…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
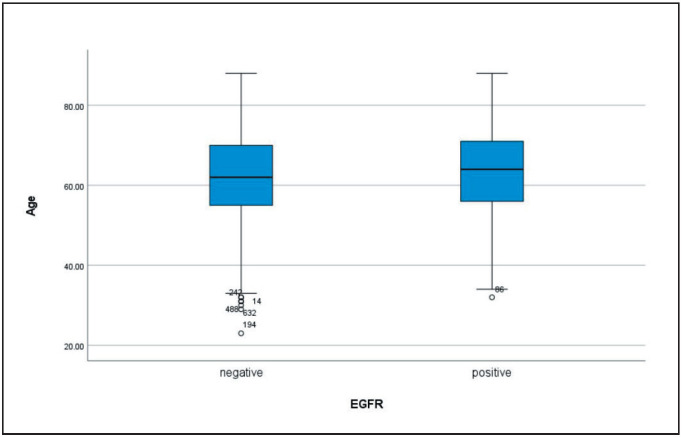 Figure 1
Figure 1|
|
|
|
|
26.4% (171 of 647) |
|
|
2.3% (15 of 647) |
|
|
0% |
|
PD-L1 expression |
54.8% (355 of 647) |
|
|
|
|
Ex19Del |
56.7% |
|
L858R |
21.6% |
|
Ex20ins |
4.1% |
|
S768I |
2.3% |
|
T790M |
4.7% |
|
L861Q |
6.4% |
|
G719X |
1.8% |
|
G787A |
1.8% |
|
G719C |
0.6% |
|
|
|
|
|
|
|
|
Negative |
632 |
97.7% |
0.126 |
|
Positive |
15 |
2.3% | ||
|
PD-L1 |
Negative |
292 |
45.2% |
0.29 |
|
1%-49% |
208 |
32.1% | ||
|
50%< |
147 |
22.7% | ||
|
|
Negative |
647 |
100% |
- |
|
Positive |
0 |
0% |
|
|
|
|
|
|
|
Age |
62 (54-70) |
63 (55-70) |
61 (53-69) |
0.15* |
|
Gender |
0.003** | |||
|
Male |
430 (66.5%) |
98 (22.8%) |
332 (77.2%) | |
|
Female |
217 (33.5%) |
73 (33.6%) |
144 (66.4%) | |
|
|
15 (2.3%) |
5 (2.9%) |
10 (2.1%) |
0.126** |
|
PD-L1 Expression |
0.29** | |||
|
TPS<1% |
292 (45.2%) |
75 (43.9%) |
217 (45.6%) | |
|
TPS:1%-49% |
208 (32.1%) |
55 (32.2%) |
153 (32.1%) | |
|
TPS>50% |
147 (22.7%) |
41 (24%) |
106 (22.3%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations
INTRODUCTION
Lung cancer is the second most common type of cancer and the primary cause of cancer-related fatalities in both men and women (1). It is estimated that lung cancer deaths could reach nearly 3 million by 2035 (2). Generally, lung malignancies are categorized into small-cell lung carcinoma (SCLC) and non-small-cell lung carcinoma (NSCLC), with NSCLC being the most frequently diagnosed type, accounting for over 50% of cases. In NSCLC, the signaling pathways involving the ErbB protein family become dysregulated, leading to increased malignant cell growth, resistance to programmed cell death, and enhanced migration and metastasis (3). The epidermal growth factor receptor (EGFR) is a 170-kilodalton transmembrane protein that belongs to the ErbB family of tyrosine kinases located on chromosome 7. When EGFR is dysregulated, it boosts the activity of intracellular pathways through tyrosine kinase autophosphorylation, resulting in increased DNA synthesis, cell proliferation, invasion, and metastasis (4).
Previous research indicates that EGFR is overexpressed in approximately 10%–41% of lung adenocarcinomas and highlights specific activating mutations in the EGFR gene, particularly in exons 18, 19, 20, and 21, which lead to sensitivity to tyrosine kinase inhibitors (TKIs), such as gefitinib (5). The prevalence of EGFR mutations in non-small-cell lung cancer (NSCLC) varies significantly among different ethnic groups, influencing patient responses to EGFR-targeted therapies. For example, East Asian populations exhibit the highest rates of EGFR mutations, estimated at 30%–50%, which are predominantly responsive to TKIs. In contrast, many African American populations have a considerably lower incidence of EGFR mutations, with most studies suggesting rates of approximately 5%–10%. Nonetheless, recent studies have indicated that African Americans with EGFR mutations can still benefit from TKI therapy (6,7). NSCLC represents a considerable public health challenge in Iran, and it is characterized by a high prevalence of adenocarcinoma and significant rates of EGFR mutations (8).
However, few investigations have been conducted on EGFR gene mutations in Iranian patients with NSCLC. Therefore, the current study aimed to evaluate EGFR mutation frequencies and the association between the rearrangement rates of PD-L1 expression, ALK, and ROS1 with EGFR mutations in 647 patients with NSCLC at the largest referral center in Northwest Iran.
MATERIAL and METHODS
This 6-year retrospective study (April 2018 to August 2024) included 647 patients with confirmed NSCLC. Among them, 171 patients had an EGFR mutation. Data were obtained from patients referred to Imam Reza Hospital in Tabriz, Iran. Demographic characteristics were recorded using the Hospital Information System (HIS). Hematoxylin and eosin (H&E) slides were evaluated by two board-certified pathologists to confirm the histologic diagnosis of NSCLC. Mutation analysis was conducted using formalin-fixed paraffin-embedded (FFPE) tissues obtained from primary or metastatic tumor sites. Genomic DNA was isolated from the patient using a Qiagen (USA) DNA extraction kit. Following DNA extraction, PCR amplification was performed to target exons 18–21 of the EGFR gene. PCR products were then sequenced using the Sanger method. To improve the specificity and sensitivity of the study, PCR of these exons was conducted in both the sense and antisense directions, and the primary PCR product was used in nested PCR. Although we performed real-time PCR with the Diatech Kit for the evaluation of seven mutations (G719x, T790M, S768I, ex20ins, L858R, L861Q, and ex19del), all results, conventional and Real-time, were analyzed and calculated. To comprehensively evaluate key genetic and protein biomarkers in non-small cell lung carcinoma (NSCLC), fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) analyses were employed to assess the status of ALK, ROS1, and PD-L1 in tumor samples.
For detecting the ALK-EML4 fusion gene, FISH analysis was conducted using the Cytocell ALK break-apart probe kit, which targets rearrangements in the ALK gene on chromosome 2p23. Following the manufacturer’s protocol, samples were prepared, and probe hybridization was carried out, followed by washing to ensure signal clarity. Cells displaying split red and green signals under a fluorescence microscope were marked as positive for ALK rearrangement, suggesting potential responsiveness to ALK-targeted therapies. Similarly, to evaluate ROS1 gene rearrangements, FISH analysis was performed using the Diagen ROS1 break-apart probe kit. This assay identifies rearrangements in the ROS1 gene on chromosome 6q22, which may indicate eligibility for ROS1-specific inhibitors. The procedure involved sample preparation, probe hybridization, and subsequent washing, as recommended in the Diagen protocol. Fluorescent signals were analyzed microscopically, with cells showing split red and green signals classified as ROS1-positive. To assess PD-L1 expression, immunohistochemistry (IHC) was performed using the PD-L1 IHC 22C3 pharmDx kit from Master Diagnostics. This assay employs a monoclonal antibody specific for PD-L1 (clone 22C3) and is validated for use on formalin-fixed, paraffin-embedded (FFPE) tissue sections. The IHC protocol included antigen retrieval, primary antibody incubation, and detection with a horseradish peroxidase (HRP) system, and the percentage of positive tumor cells were evaluated under light microscopy, with PD-L1 levels reported as the tumor proportion score (TPS) to indicate the extent of PD-L1 expression in tumor samples.
Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. Continuous variables were presented as the median and interquartile range (IQR) since the data were not normally distributed, as confirmed by the Kolmogorov-Smirnov test. Categorical variables were expressed as frequencies and percentages. For comparisons between groups, the following statistical tests were applied: Mann-Whitney U test, Fisher’s exact test. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 27.0. This study adhered to the Helsinki Declaration and was approved by the Ethics Committee of Tabriz University of Medical Sciences, Tabriz, Iran (Reference number: IR.TBZMED.REC.1398.091).
RESULTS
Our study included 647 cases of NSCLC. Of these, 430 cases were males (66.5%) and 217 cases were females (33.5%). The median age was 62 years (IQR: 54-70). Among the 647 specimens, 633 specimens (97.8%) were obtained from biopsies and 14 (2.2%) specimens were resected surgically. The overall frequencies of the EGFR, ALK, ROS1 alterations are summarized in Table 1.
Among the 171 studied cases (26.4%) with EGFR mutation, 165 cases (96.5%) were primary, and 6 (3.5%) cases were metastatic. Our results showed that EGFR mutations were more frequent in women than in men (33.6% versus 22.8%) (p=0.003). Also, the median age of EGFR-positive cases was 63 (IQR: 55-70), compared to 61 years (IQR: 53-69) in the EGFR-negative group (Mann-Whitney U test, p = 0.15) (Figure 1). The most common EGFR mutation was exon 19 deletion (56.7%), followed by L858R point mutation (21.6%) and exon 20 insertion (4.1%). Other mutations, including G719X, S768I, and L861Q, were observed in smaller proportions (Table 2). ALK rearrangements were detected in 15 cases (2.3%), with no significant association between EGFR mutations and ALK rearrangements (Fisher’s exact test, p = 0.126). The mutual exclusivity of EGFR and ALK mutations was consistent with findings from previous studies. No ROS1 rearrangements were identified in the cohort. PD-L1 expression was categorized as (TPS < 1%: 45.2% of cases, TPS 1–49%: 32.1% of cases, TPS ≥ 50%: 22.7% of cases). There was no significant association between PD-L1 expression and EGFR mutation status (Fisher’s exact test, p = 0.29) (Table 3, Table 4).
Box plot chart of age in two groups (EGFR positive and negative).
While specific histopathological subtypes (e.g., adenocarcinoma, squamous cell carcinoma) were not detailed in the dataset, the high prevalence of EGFR mutations suggests a predominance of adenocarcinoma, as EGFR mutations are more commonly associated with this subtype. Further studies with detailed histopathological data are needed to confirm this finding.
DISCUSSION
EGFR mutations play a pivotal role in the clinical management of NSCLC, influencing both patient demographics and therapeutic responses. As one of the most common genetic alterations in NSCLC, particularly in adenocarcinoma subtypes, EGFR mutations have been extensively studied to understand their implications for targeted therapies. The presence of these mutations is associated with favorable outcomes when treated with EGFR tyrosine kinase inhibitors (TKIs), which have revolutionized the treatment landscape for NSCLC (9). However, the relationship between EGFR mutation status and patient characteristics, such as age, sex, and other gene expressions, is complex and warrants further exploration. This study aimed to elucidate the demographic and molecular characteristics of patients with NSCLC and EGFR mutations in a large Iranian cohort. Patients with EGFR mutations in NSCLC exhibit distinct clinical and demographic characteristics influencing treatment responses. Our findings confirm that EGFR mutations are more prevalent in females (33.6%) than in males (22.8%, p=0.003), consistent with previous studies (10). The higher prevalence of EGFR mutations in females aligns with global trends, particularly in East Asian populations, where EGFR mutations are found in 30-50% of NSCLC cases (11). Additionally, the mean age of EGFR-positive patients (63 years) was slightly higher than that of EGFR-negative patients (61 years), although this difference was not statistically significant. This finding contrasts with some studies in which younger age was associated with a higher likelihood of certain mutations but lower overall rates of EGFR mutations. For instance, a study found that among female NSCLC patients, those aged over 57 years had a higher prevalence of EGFR mutations (70%) compared with younger patients (39%) (12), highlighting the need for further investigation into age-related differences in EGFR mutation prevalence.
This gender disparity may be attributed to hormonal influences or differences in smoking patterns, as EGFR mutations are more common in never-smokers (12). Although smoking status was not available in our dataset, some studies show that never-smokers have a higher prevalence of EGFR mutations than smokers. For example, in a meta-analysis, the mutation rates were reported at 70% for never-smokers versus 41.9% for smokers, indicating a strong inverse relationship between smoking and the EGFR mutation status (11). In a study by Parvar et al., 81.8% of the patients with EGFR mutations were never-smokers, highlighting the association between nonsmoking status and positive EGFR mutations (13). Moreover, current smokers with EGFR mutations often have worse overall survival compared with non-smokers (14).
Histologically, most EGFR-mutant NSCLC cases are adenocarcinomas, which is the most common lung cancer subtype among non-smokers (15). In East Asian populations, the prevalence of EGFR mutations is 47.9% in adenocarcinoma and 4.6% in lung squamous cell carcinoma, while in Western people, it is 19.2% in lung adenocarcinoma and 3.3% in lung squamous cell carcinoma (16). The most frequent EGFR mutations include exon 19 deletions, occurring in 50-60% of cases, and the L858R point mutation in exon 21, present in about 30% of cases. Less common mutations, such as exon 20 insertions, are also observed at lower frequencies (17). Our study similarly revealed that the most prevalent mutations were exon 19 deletion (56.7%), L858R point mutation (21.6%), and exon 20 insertion (4.1%), consistent with global data. Patients with positive EGFR mutation generally respond favorably to EGFR tyrosine kinase inhibitors (TKIs) such as gefitinib and osimertinib (18,19). Studies have shown that progression-free survival (PFS) is usually longer in patients receiving TKIs compared with those receiving standard chemotherapy, often exceeding 10 months (20). However, the presence of less common mutations, such as exon 20 insertions, underscores the importance of comprehensive molecular testing to guide personalized treatment strategies. In our study, no significant association was observed between PD-L1 expression and EGFR mutation status (p = 0.29). This finding contrasts with some studies that reported higher PD-L1 expression in EGFR-mutant tumors (21,22), while others suggest a negative correlation (23). The lack of consistency in these results may reflect differences in study populations, methodologies, or ethnic gene expression. For instance, Tang et al. reported PD-L1 overexpression in 71.9% of EGFR-mutant NSCLC cases, compared to 57.1% in wild-type cases (22). Meanwhile, Kojima et al. found that EGFR mutations were associated with lower PD-L1 expression and poorer responses to immune checkpoint inhibitors (24). These discrepancies highlight the need for further research to clarify the relationship between EGFR mutations and PD-L1 expression, particularly in diverse populations. Studies have shown that ROS1 rearrangements and EGFR mutations are generally mutually exclusive events in NSCLC (25). For instance, a comprehensive review noted that while ROS1 rearrangements occur in approximately 1-2% of NSCLC cases, concurrent occurrences with EGFR mutations are extremely rare, with only a few documented cases in the literature (26). Prognostically, both mutations improve responses to targeted therapies (21,25). Similarly, in the present study, no ROS1 Rearrangements were detected. Our findings support the mutual exclusivity of EGFR mutations and ALK rearrangements, as only 2.9% of EGFR-positive cases harbored concurrent ALK rearrangements (p = 0.126). This is consistent with previous studies. For example, in a study by Yang et al., out of 2975 EGFR-positive patients, only nine had concurrent mutations involving both genes (27). The rarity of cooccurrence implies that testing for one mutation often leads to the exclusion of testing for the other unless specific clinical characteristics suggest otherwise.
One of the key strengths of this study is its large sample size (n = 647), which is the largest cohort of patients with NSCLC and EGFR mutations studied in Iran to date. This study provides valuable insights into the demographic and molecular characteristics of EGFR-mutant NSCLC in an understudied population. However, several limitations should be acknowledged. First, the lack of data on smoking status, tumor stage, and histopathological subtypes limits our exploration of the relationship between these factors and EGFR mutation status. Second, the retrospective nature of the study may have introduced selection bias. Finally, the absence of survival data precludes an analysis of the impact of EGFR mutations on patient outcomes.
CONCLUSION
This study contributes to the growing body of literature on EGFR mutations in NSCLC by providing data from a large Iranian cohort. Our findings confirm that the EGFR mutations in NSCLC are associated with distinct demographic characteristics such as female sex and older age. The high prevalence of common mutations like exon 19 deletions and L858R underscores the utility of EGFR-TKIs, which generally improve progression-free survival compared with chemotherapy. The lack of a significant association between EGFR mutations and PD-L1 expression underscores the need for further research to clarify the role of immune checkpoint inhibitors in EGFR-mutant NSCLC. Additionally, the mutual exclusivity of EGFR mutations and ALK/ROS1 rearrangements reinforces the importance of sequential molecular testing in NSCLC management. Future studies should aim to include a more diverse patient population, encompassing various ethnicities and geographic regions, to better understand the global prevalence and characteristics of EGFR mutations in NSCLC. Additionally, incorporating data on smoking status, tumor stage, and histopathological subtypes would provide a more comprehensive understanding of the factors influencing EGFR mutation status and treatment outcomes. Finally, prospective studies using survival data are needed to evaluate the long-term impact of EGFR mutations on patient outcomes and to optimize personalized treatment strategies.
Conflict of Interest
The authors have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thomas David, Maloney Mc Kenzie E., Raval Girindra Cureus Concomitant EGFR Mutations and ALK Rearrangements in Lung Adenocarcinoma Treated With Osimertinib 11202315 e 48122 e 4812210.7759/cureus.48122 PMC 1069006838046784 · doi ↗ · pubmed ↗
- 2Mohammadi Sotoudeh, Rezaei Mitra, Shojaeian Fatemeh, Pourabdollah Mihan, Mohammadi Ziazi Leila, Seifi Sharareh, Doroudinia Atousa, Salimi Babak, Khosravi Adnan, Farhangnasab Mohammad Amin Iran J Pathol The Frequency of Epidermal Growth Factor Receptor (EGFR) Mutation in Patients with Lung Adenocarcinoma Referred to a Lung Diseases Hospital; A Cross-Sectional Study from Iran 20221715916510.30699/IJP.2022.533427.267335463723 PMC 9013864 · doi ↗ · pubmed ↗
- 3Siegelin Markus D., Borczuk Alain C. Lab Invest Epidermal growth factor receptor mutations in lung adenocarcinoma 0220149412913710.1038/labinvest.2013.14724378644 · doi ↗ · pubmed ↗
- 4Prabhakar Charles N. Transl Lung Cancer Res Epidermal growth factor receptor in non-small cell lung cancer 042015411011810.3978/j.issn.2218-6751.2015.01.0125870793 PMC 4384217 · doi ↗ · pubmed ↗
- 5Liang Zhiyong, Zhang Jing, Zeng Xuan, Gao Jie, Wu Shafei, Liu Tonghua BMC Cancer Relationship between EGFR expression, copy number and mutation in lung adenocarcinomas 0720101037637610.1186/1471-2407-10-37620637128 PMC 2913962 · doi ↗ · pubmed ↗
- 6Jordan Emmet J., Kim Hyunjae R., Arcila Maria E., Barron David, Chakravarty Debyani, Gao Jian Jiong, Chang Matthew T., Ni Andy, Kundra Ritika, Jonsson Philip, Jayakumaran Gowtham, Gao Sizhi Paul, Johnsen Hannah C., Hanrahan Aphrothiti J., Zehir Ahmet, Rekhtman Natasha, Ginsberg Michelle S., Li Bob T., Yu Helena A., Paik Paul K., Drilon Alexander, Hellmann Matthew D., Reales Dalicia N., Benayed Ryma, Rusch Valerie W., Kris Mark G., Chaft Jamie E., Baselga José, Taylor Barry S., Schultz Nikolaus, Rudin Charles M., Hyman David M., · doi ↗ · pubmed ↗
- 7Rosell Rafael, Moran Teresa, Queralt Cristina, Porta Rut, Cardenal Felipe, Camps Carlos, Majem Margarita, Lopez-Vivanco Guillermo, Isla Dolores, Provencio Mariano, Insa Amelia, Massuti Bartomeu, Gonzalez-Larriba Jose Luis, Paz-Ares Luis, Bover Isabel, Garcia-Campelo Rosario, Moreno Miguel Angel, Catot Silvia, Rolfo Christian, Reguart Noemi, Palmero Ramon, Sánchez José Miguel, Bastus Roman, Mayo Clara, Bertran-Alamillo Jordi, Molina Miguel Angel, Sanchez Jose Javier, Taron Miquel, Spanish Lung Cancer Group N Engl J Med Scree · doi ↗ · pubmed ↗
- 8Payandeh M, Sadeghi M, Sadeghi M Clinicopathological Features of Patients with Non-small-cell Lung Cancer in West of Iran 2016898102